Novel Coronavirus 2019 (COVID-19): Q&A on Global Implications and Responses
In December 2019, hospitals in the city of Wuhan in China’s Hubei Province began seeing cases of pneumonia of unknown origin. Chinese health authorities ultimately connected the condition, later named coronavirus disease 2019 (COVID-19), to a previously unidentified strain of coronavirus. The disease has spread to almost every country in the world, including the United States. WHO declared the outbreak a Public Health Emergency of International Concern on January 30, 2020; raised its global risk assessment to “Very High” on February 28; and labeled the outbreak a “pandemic” on March 11. In using the term pandemic, WHO Director-General Tedros Adhanom Ghebreyesus cited COVID-19’s “alarming levels of spread and severity” and governments’ “alarming levels of inaction.” As of May 14, 2020, WHO had reported more than 4.2 million COVID-19 cases, including almost 300,000 deaths, of which more than 40% of all cases and 55% of all deaths were identified in Europe, and more than 30% of all cases and nearly 30% of all deaths were identified in the United States. Members of Congress have demonstrated strong interest in ending the pandemic domestically and globally. To date, Members have introduced dozens of pieces of legislation on international aspects of the pandemic (see the Appendix).
Individual countries are carrying out not only domestic but also international efforts to control the COVID-19 pandemic, with the WHO issuing guidance, coordinating some international research and related findings, and coordinating health aid in low-resource settings. Countries are following (to varying degrees) WHO policy guidance on COVID-19 response and are leveraging information shared by WHO to refine national COVID-19 plans. The United Nations (U.N.) Office for the Coordination of Humanitarian Affairs (UNOCHA) is requesting almost $7 billion to support COVID-19 efforts by several U.N. entities. International financial institutions (IFIs), including the International Monetary Fund (IMF), the World Bank, and the regional development banks, are mobilizing their financial resources to support countries grappling with the COVID-19 pandemic. The IMF has announced it is ready to tap its total lending capacity, about $1 trillion, to support governments responding to COVID-19. The World Bank can mobilize about $150 billion over the next 15 months, and the regional development banks are also preparing new programs and redirecting existing programs to help countries respond to the economic ramifications of COVID-19.
On January 29, 2020, President Donald Trump announced the formation of the President’s Coronavirus Task Force, led by the Department of Health and Human Services (HHS) and coordinated by the White House National Security Council (NSC). On February 27, the President appointed Vice President Michael Pence as the Administration’s COVID-19 task force leader, and the Vice President subsequently appointed the President’s Emergency Plan for AIDS Relief (PEPFAR) Ambassador Deborah Birx as the “White House Coronavirus Response Coordinator.” On March 6, 2020, the President signed into law the Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020, P.L. 116-123, which provides $8.3 billion for domestic and international COVID-19 response. The Act includes $300 million to continue the U.S. Centers for Disease Control and Prevention’s (CDC) global health security programs and a total of $1.25 billion for the U.S. Agency for International Development (USAID) and Department of State. Of those funds, $985 million is designated for foreign assistance accounts, including $435 million specifically for Global Health Programs. On March 27, 2020, President Trump signed the Coronavirus Aid, Relief, and Economic Security Act (CARES Act), P.L. 116-136, which contains emergency funding for U.S. international COVID-19 responses, including $258 million to USAID through the International Disaster Assistance (IDA) account and $350 million to the State Department through the Migration and Refugee Assistance (MRA) account (P.L. 116-127).
The pandemic presents major consequences for foreign aid, global health, diplomatic relations, the global economy, and global security. Regarding foreign aid, Congress may wish to consider how the pandemic might reshape pre-existing U.S. aid priorities—and how it may affect the ability of U.S. personnel to implement and oversee programs in the field. The pandemic is also raising questions about deportation and sanction policies, particularly regarding Latin America and the Caribbean and Iran. In the 116th Congress, Members have introduced legislation to respond to the COVID-19 pandemic in particular and to address global pandemic preparedness in general. This report focuses on global implications of and responses to the COVID-19 pandemic, and is organized into four broad parts that answer common questions regarding: (1) the disease and its global prevalence, (2) country and regional responses, (3) global economic and trade implications, and (4) issues that Congress might consider. For information on domestic COVID-19 cases and related responses, see CRS Insight IN11253, Domestic Public Health Response to COVID-19: Current Status and Resources Guide, by Kavya Sekar and Ada S. Cornell.
Novel Coronavirus 2019 (COVID-19): Q&A on Global Implications and Responses
Jump to Main Text of Report
Contents
- Introduction
- What are coronaviruses and what is COVID-19?
- How is COVID-19 transmitted?
- What are global COVID-19 case fatality and hospitalization rates?
- Where are COVID-19 cases concentrated?
- COVID-19 Responses of International Institutions
- International Health Regulations
- What rules guide COVID-19 responses worldwide?
- How does WHO respond to countries that do not comply with IHR (2005)?
- How does the Global Health Security Agenda (GHSA) relate to IHR (2005) and pandemic preparedness?
- Multilateral Technical Assistance
- What is WHO doing to respond to the COVID-19 pandemic?
- How are international financial institutions responding to COVID-19?
- What is the U.N. humanitarian response to the COVID-19 pandemic?
- U.S. Support for International Responses
- Emergency Appropriations for International Responses
- U.S. Department of State
- How does the State Department help American citizens abroad?
- What are the authorities and funding for the State Department to carry out overseas evacuations?
- How many evacuations have been carried out due to the COVID-19 pandemic?
- U.S. Agency for International Development (USAID)
- Where is USAID providing COVID-19 assistance?
- What type of assistance does USAID provide for COVID-19 control?
- How do USAID COVID-19 responses relate to regular pandemic preparedness activities?
- U.S. Centers for Disease Control and Prevention (CDC)
- What role is CDC playing in international COVID-19 responses?
- How do CDC COVID-19 responses relate to regular pandemic preparedness activities?
- U.S. Department of Defense (DOD)
- What is the DOD global COVID-19 response?
- Emergency Appropriations for DOD Responses
- To what extent is COVID-19 affecting United States security personnel?
- Regional Implications of and Responses to the COVID-19 Pandemic
- Asia
- What are the implications for U.S.-China relations?
- What are the implications in Southeast Asia?
- What are the implications in Central Asia?
- What are the implications in South Asia?
- What are the implications in Australia and New Zealand?
- What are the implications for U.S. withdrawal from Afghanistan?
- What COVID-19 containment lessons could be learned from Asia?
- Europe
- How are European governments and the European Union (EU) responding?
- How is the pandemic affecting U.S.-European relations?
- Africa
- How are African governments responding?
- How is the Africa CDC responding?
- Middle East and North Africa
- How are Middle Eastern and North African governments responding?
- What are the implications for U.S.-Iran policy?
- Canada, Latin America, and the Caribbean
- How is the Canadian government responding?
- How are Latin American and Caribbean governments responding?
- International Economic and Supply Chain Issues
- What are the implications of the pandemic in China's economy?
- How is COVID-19 affecting the global economy and financial markets?
- How is COVID-19 affecting U.S. medical supply chains?
- Issues for Congress
Figures
Tables
- Table 1. Top 10 Countries with Confirmed COVID-19 Cases and Deaths
- Table 2. COVID-19 Cases and Deaths, by WHO Region
- Table 3. United Nations COVID-19 Appeal: April-December 2020
- Table 4. USAID Global Pandemic Preparedness Funding: FY2017-FY2021 Request
- Table 5. CDC Global Pandemic Preparedness Funding: FY2017-2020 Enacted
- Table A-1. Report Authors
Appendixes
Summary
In December 2019, hospitals in the city of Wuhan in China's Hubei Province began seeing cases of pneumonia of unknown origin. Chinese health authorities ultimately connected the condition, later named coronavirus disease 2019 (COVID-19), to a previously unidentified strain of coronavirus. The disease has spread to almost every country in the world, including the United States. WHO declared the outbreak a Public Health Emergency of International Concern on January 30, 2020; raised its global risk assessment to "Very High" on February 28; and labeled the outbreak a "pandemic" on March 11. In using the term pandemic, WHO Director-General Tedros Adhanom Ghebreyesus cited COVID-19's "alarming levels of spread and severity" and governments' "alarming levels of inaction." As of May 14, 2020, WHO had reported more than 4.2 million COVID-19 cases, including almost 300,000 deaths, of which more than 40% of all cases and 55% of all deaths were identified in Europe, and more than 30% of all cases and nearly 30% of all deaths were identified in the United States. Members of Congress have demonstrated strong interest in ending the pandemic domestically and globally. To date, Members have introduced dozens of pieces of legislation on international aspects of the pandemic (see the Appendix).
Individual countries are carrying out not only domestic but also international efforts to control the COVID-19 pandemic, with the WHO issuing guidance, coordinating some international research and related findings, and coordinating health aid in low-resource settings. Countries are following (to varying degrees) WHO policy guidance on COVID-19 response and are leveraging information shared by WHO to refine national COVID-19 plans. The United Nations (U.N.) Office for the Coordination of Humanitarian Affairs (UNOCHA) is requesting almost $7 billion to support COVID-19 efforts by several U.N. entities. International financial institutions (IFIs), including the International Monetary Fund (IMF), the World Bank, and the regional development banks, are mobilizing their financial resources to support countries grappling with the COVID-19 pandemic. The IMF has announced it is ready to tap its total lending capacity, about $1 trillion, to support governments responding to COVID-19. The World Bank can mobilize about $150 billion over the next 15 months, and the regional development banks are also preparing new programs and redirecting existing programs to help countries respond to the economic ramifications of COVID-19.
On January 29, 2020, President Donald Trump announced the formation of the President's Coronavirus Task Force, led by the Department of Health and Human Services (HHS) and coordinated by the White House National Security Council (NSC). On February 27, the President appointed Vice President Michael Pence as the Administration's COVID-19 task force leader, and the Vice President subsequently appointed the President's Emergency Plan for AIDS Relief (PEPFAR) Ambassador Deborah Birx as the "White House Coronavirus Response Coordinator." On March 6, 2020, the President signed into law the Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020, P.L. 116-123, which provides $8.3 billion for domestic and international COVID-19 response. The Act includes $300 million to continue the U.S. Centers for Disease Control and Prevention's (CDC) global health security programs and a total of $1.25 billion for the U.S. Agency for International Development (USAID) and Department of State. Of those funds, $985 million is designated for foreign assistance accounts, including $435 million specifically for Global Health Programs. On March 27, 2020, President Trump signed the Coronavirus Aid, Relief, and Economic Security Act (CARES Act), P.L. 116-136, which contains emergency funding for U.S. international COVID-19 responses, including $258 million to USAID through the International Disaster Assistance (IDA) account and $350 million to the State Department through the Migration and Refugee Assistance (MRA) account (P.L. 116-127).
The pandemic presents major consequences for foreign aid, global health, diplomatic relations, the global economy, and global security. Regarding foreign aid, Congress may wish to consider how the pandemic might reshape pre-existing U.S. aid priorities—and how it may affect the ability of U.S. personnel to implement and oversee programs in the field. The pandemic is also raising questions about deportation and sanction policies, particularly regarding Latin America and the Caribbean and Iran. In the 116th Congress, Members have introduced legislation to respond to the COVID-19 pandemic in particular and to address global pandemic preparedness in general. This report focuses on global implications of and responses to the COVID-19 pandemic, and is organized into four broad parts that answer common questions regarding: (1) the disease and its global prevalence, (2) country and regional responses, (3) global economic and trade implications, and (4) issues that Congress might consider. For information on domestic COVID-19 cases and related responses, see CRS Insight IN11253, Domestic Public Health Response to COVID-19: Current Status and Resources Guide, by Kavya Sekar and Ada S. Cornell.
Introduction
In December 2019, a new disease, later called COVID-19, emerged in China and quickly spread around the world. The disease presents major consequences for global health, foreign relations, the global economy, and global security. International institutions and country governments are taking a variety of responses to address these challenges. In the 116th Congress, Members have introduced legislation to respond to COVID-19 in particular and to address global pandemic preparedness in general that are now occurring on a global scale. This report focuses on global implications of and responses to the COVID-19 pandemic, and is organized into four broad parts that answer common questions regarding: (1) the disease and its global prevalence, (2) country and regional responses, (3) global economic and trade implications, and (4) issues that Congress might consider. For information on domestic COVID-19 cases and related responses, see CRS Insight IN11253, Domestic Public Health Response to COVID-19: Current Status and Resources Guide, by Kavya Sekar and Ada S. Cornell.
What are coronaviruses and what is COVID-19?1
Coronaviruses that typically infect humans are common pathogens, which can cause mild illnesses with symptoms similar to the common cold, or severe illness, potentially resulting in death of the victim. Prior to COVID-19, two "novel" coronaviruses (i.e., coronaviruses newly recognized to infect humans) have caused serious illness and death in large populations, namely severe acute respiratory syndrome (SARS) in 2002-2003 and Middle East Respiratory Syndrome (MERS), which was first identified in 2012 and continues to have sporadic transmission from animals to people with limited human-to-human spread.2
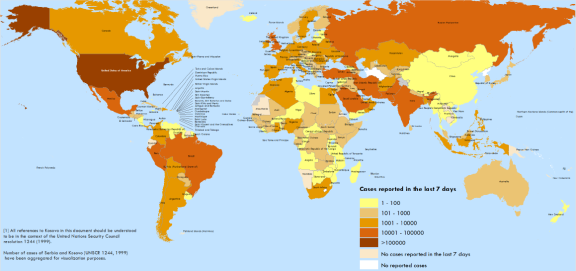
The origin of COVID-19 is unknown, although genetic analysis suggests an animal source.3 The World Health Organization (WHO) first learned of pneumonia cases from unknown causes in Wuhan, China, on December 31, 2019. In the first days of January 2020, Chinese scientists isolated a previously unknown coronavirus in the patients, and on January 11, Chinese scientists shared its genetic sequence with the international community. (See CRS Report R46354, COVID-19 and China: A Chronology of Events (December 2019-January 2020), by Susan V. Lawrence.) The virus is now present in most countries (Figure 1). For the purposes of this report, CRS refers to COVID-19 as the virus and the syndrome people often develop when infected.4
 |
|
Source: World Health Organization, COVID-19 Situation Report 114, May 13, 2020. |
How is COVID-19 transmitted?5
Health officials and researchers are still learning about COVID-19. According to the U.S. Centers for Disease Control and Prevention (CDC), the virus is thought to spread mainly from person-to-person between individuals who are in close contact with each other (less than six feet), through respiratory droplets produced when an infected person coughs or sneezes.6 Health officials and researchers are still determining the virus's incubation period, or time between infection and onset of symptoms. CDC is using 14 days as the outer bound for the incubation period, meaning that the agency expects someone who has been infected to show symptoms within that period.
The CDC has confirmed that asymptomatic cases (infected individuals who do not have symptoms) can transmit the virus, though "their role in transmission is not yet known."7 A study of the 3,711 passengers on the Diamond Princess cruise ship found that 712 people (19.2% of the cruise ship passengers) tested positive for COVID-19. Almost half (331) of the positive cases were asymptomatic at the time of testing.8
What are global COVID-19 case fatality and hospitalization rates?9
The COVID-19 case fatality rate is difficult to determine; milder cases are not being diagnosed, death is delayed, and wide disparities exist in case detection worldwide. In addition, the case fatality rate in any given context may depend on a number of factors including the demographics of the population, density of the area, and the quality and availability of health care services. Scientists are using different methods to estimate case fatality and estimates range. One study of those diagnosed with COVID-19 estimated case fatality rates for Wuhan, China and other parts of China at 1.4% and 0.85%, respectively.10 Another estimated 3.6% within China and 1.5% outside the country,11 with a third recommending using a range of 0.2%-3.0%.12
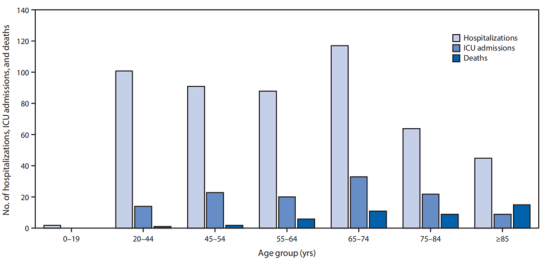
Current data suggest the elderly and those with preexisting medical conditions (including asthma, high blood pressure, heart disease, cancer, and diabetes) are more likely to become severely sickened by COVID-19. One study in China showed that 80% of those killed by the virus were older than 60 years and 81% of surveyed COVID-19 cases were mild.13 Another study showed that 87% of all hospitalized COVID-19 patients in China were aged between 30 and 79 years, though the study did not further disaggregate the data by age.14 Whereas the CDC found that the elderly had higher death rates, more than half (55%) of reported COVID-19 hospitalizations between February 12 and March 16, 2020, were of individuals younger than 65 years (Figure 2).15
Where are COVID-19 cases concentrated?16
As of May 13, 2020, national governments reported to the WHO more than 4 million cases of COVID-19 and almost 300,000 related deaths worldwide. Ten countries accounted for over 70% of all reported cases and almost 80% of all reported deaths (Table 1). The pandemic epicenter has shifted from China and Asia to the United States and Europe. China and Belgium are no longer among the 10 countries with the highest number of deaths, and Russia and Brazil joined the ranks. Almost 90% of all reported cases were identified in the WHO Americas and Europe regions (Table 2).17 Cases are continuing to rise in the Americas, where 88% of all cases were found in the United States (74%), Brazil (9%), and Canada (4%). In Europe, the cases are more widely distributed, and seven countries comprise 77% of all cases: Russia (14%), Spain (13%), United Kingdom (13%), Italy (12%), Germany (10%), Turkey (8%) and France (8%).
|
Country |
Cases |
Deaths |
% of All Cases |
% of All Deaths |
|
United States |
1,320,054 |
79,634 |
31.6 |
27.7 |
|
Russia |
242,271 |
2,212 |
5.8 |
0.8 |
|
Spain |
228,030 |
26,920 |
5.5 |
9.4 |
|
United Kingdom |
224,467 |
32,692 |
5.4 |
11.4 |
|
Italy |
221,216 |
30,911 |
5.3 |
10.8 |
|
Germany |
171,306 |
7,634 |
4.1 |
2.7 |
|
Brazil |
168,331 |
11,519 |
4.0 |
4.0 |
|
Turkey |
141,475 |
3,894 |
3.4 |
1.4 |
|
France |
138,161 |
26,948 |
3.3 |
9.4 |
|
Iran |
110,767 |
6,733 |
2.7 |
2.3 |
|
Top 10 Total |
2,968,078 |
229,097 |
71.2 |
79.7 |
|
Grand Total |
4,170,424 |
287,399 |
100.0 |
100.0 |
Source: WHO, Coronavirus Disease 2019 (COVID-19) Situation Report 114, May 13, 2020.
|
WHO Region |
Cases |
Deaths |
% of All Cases |
% of All Deaths |
|
Europe |
1,780,316 |
159,799 |
42.7 |
55.6 |
|
Americas |
1,781,564 |
106, 504 |
42.7 |
37.1 |
|
Western Pacific |
163,201 |
6,578 |
3.9 |
2.3 |
|
Eastern Mediterranean |
284,270 |
9,259 |
6.8 |
3.2 |
|
Southeast Asia |
110,932 |
3,746 |
2.7 |
1.3 |
|
Africa |
49,429 |
1,500 |
1.2 |
0.5 |
|
Diamond Princess |
712 |
13 |
0.0 |
0.0 |
|
Total |
4,170,424 |
287,399 |
100.0 |
100.0 |
Source: WHO, Coronavirus Disease 2019 (COVID-19) Situation Report 114, May 13, 2020.
Note: WHO regions at https://www.who.int/chp/about/regions/en/, accessed on April 6, 2020.
COVID-19 Responses of International Institutions
Individual countries carry out both domestic and international efforts to control the COVID-19 pandemic, with the WHO issuing guidance, coordinating some international research and related findings, and coordinating health aid in low-resource settings. Countries follow (to varying degrees) WHO policy guidance on COVID-19 response and leverage information shared by WHO to refine national COVID-19 plans. The United Nations (U.N.) Office for the Coordination of Humanitarian Affairs (UNOCHA) is requesting $6.7 billion to support COVID-19 efforts by several U.N. entities (see "Multilateral Technical Assistance" section).18
International Health Regulations19
What rules guide COVID-19 responses worldwide?
WHO is the U.N. agency responsible for setting norms and rules on global health matters, including on pandemic response. The organization also develops and provides tools, guidance and training protocols. In 1969, the World Health Assembly (WHA)—the governing body of WHO—adopted the International Health Regulations (IHR) to stop the spread of six diseases through quarantine and other infectious disease control measures. The WHA has amended the IHR several times, most recently in 2005.20 The 2005 edition, known as IHR (2005), provided expanded means for controlling infectious disease outbreaks beyond quarantine. The regulations include a code of conduct for notification of and responses to disease outbreaks with pandemic potential, and carry the expectation that countries (and their territories) will build the capacity, where lacking, to comply with IHR (2005). The regulations mandate that WHO Member States
- build and maintain public health capacities for disease surveillance and response;
- provide or facilitate technical assistance to help low-resource countries develop and maintain public health capacities;
- notify WHO of any event that may constitute a Public Health Emergency of International Concern (PHEIC) and respond to requests for verification of information regarding such event; and
- follow WHO recommendations concerning public health responses to the relevant PHEIC.
Per reporting requirements of the IHR (2005), China and other countries are monitoring and reporting COVID-19 cases to WHO. Observers are debating the extent to which China is fully complying with IHR (2005) reporting rules (see "Asia" and the Appendix).
How does WHO respond to countries that do not comply with IHR (2005)?
IHR (2005) does not have an enforcement mechanism. WHO asserts that "peer pressure and public knowledge" are the "best incentives for compliance."21 Consequences that WHO purports non-compliant countries might face include a tarnished international image, increased morbidity and mortality of affected populations, travel and trade restrictions imposed by other countries, economic and social disruption, and public outrage.
China's response to the COVID-19 outbreak may deepen debates about the need for an IHR enforcement mechanism. On one hand, questions about the timeliness of China's reporting of the COVID-19 outbreak and questions about China's transparency thereafter might bolster arguments in favor of an enforcement mechanism. On the other hand, some have questioned whether the WHA would vote to abdicate some of its sovereignty to provide WHO enforcement authority.
How does the Global Health Security Agenda (GHSA) relate to IHR (2005) and pandemic preparedness?
IHR (2005) came into force in 2007, with signatory countries committing to comply by 2012. In 2012, only 20% of countries reported to the WHO that they had developed IHR (2005) core capacities, and many observers asserted the regulations needed a funding mechanism to help resource-constrained countries with compliance. In 2014, the WHO launched the Global Health Security Agenda (GHSA) as a five-year (2014-2018) multilateral effort to accelerate IHR (2005) implementation, particularly in resource-poor countries lacking the capacity to adhere to the regulations. The GHSA appeared to advance global pandemic preparedness capacity; more than 70% of surveyed countries reported in 2017 being prepared to address a global pandemic.22 Regional disparities persisted, however; about 55% of surveyed countries in the WHO Africa region reported being prepared for a pandemic, compared to almost 90% of countries surveyed in the WHO Western Pacific region. In 2017, participating countries agreed to extend the GHSA through 2024. For more information on the GHSA, see CRS In Focus IF11461, The Global Health Security Agenda (GHSA): 2020-2024, by Tiaji Salaam-Blyther.
Multilateral Technical Assistance
What is WHO doing to respond to the COVID-19 pandemic?23
In February 2020, WHO released a $675 million Strategic Preparedness and Response Plan for February through April 2020. WHO aims to provide international coordination and operational support, bolster country readiness and response capacity—particularly in low-resource countries—and accelerate research and innovation. As of May 8, private donors and 26 countries have contributed $536.5 million towards the plan, including $30.3 million from the United States.24 Countries have pledged an additional $198.5 million towards the plan. As of April 22, WHO has used the funds to
- purchase and ship personal protective equipment (PPE) to 133 countries, including
- 2,566,880 surgical masks and masks,
- 1,641,900 boxes of gloves,
- 184,478 gowns,
- 29,873 goggles, and
- 79,426 face shields;
- supply 1,500,000 diagnostic kits to 126 countries;
- develop online COVID-19 training courses in 13 languages; and
- enroll more than 100 countries in WHO-coordinated trials to accelerate identification of an effective vaccine and treatment, which include
- 1,200 patients,
- 144 studies, and
- 6 candidate vaccines in clinical evaluation and 77 in preclinical evaluation.25
In April 2020, the WHO issued an updated plan that provided guidance for countries preparing for a phased transition from widespread transmission to a steady state of low-level or no transmission, among other things.26 The update did not include a request for additional funds.
Also in April 2020, the WHO hosted a virtual event with the President of France, the President of the European Commission, and the Bill & Melinda Gates Foundation where heads of state, the G20 President, the African Union Commission Chairperson, the U.N. Secretary General and leaders from a variety of nongovernmental organizations, including Gavi, the Vaccine Alliance, and the Coalition for Epidemic Preparedness and Innovation (CEPI), pledged their commitment to the Access to COVID-19 Tools (ACT Accelerator).27 The participants, and other partners who have since joined the effort, committed to "work towards equitable global access" to COVID-19 countermeasures (including vaccines and therapies). A pledging conference, hosted by the European Union (EU), took place on May 4 to support the effort. As of May 6, donors have pledged $7.4 billion for the ACT Accelerator and other global COVID-19 responses. The United States neither participated in the launch nor provided funding for the ACT Accelerator.
Debates about whether health commodities are a public good are long-standing and have intensified in recent years. For decades, countries have willingly donated virus samples to the WHO for international research. During a 2005-2007 H5N1 avian flu outbreak, however, Indonesia refused to share samples of the virus, asserting that companies were selling patented vaccines created from the donated samples at a price Indonesians could not afford.28 The WHO and its Member States, through the WHA, have not yet developed an agreement that satisfies poor countries concerned about affordability and wealthier countries (where most global pharmaceutical companies are based) concerned about recapturing research and development costs. The WHO has sought to negotiate prepurchasing agreement during each major outbreak since the H5N1 debacle. French officials, for example, have characterized any COVID-19 commodity that might be developed as a "public good," and they have criticized statements by a French pharmaceutical company on committing to provide the U.S. government first access to a COVID-19 vaccine that the company produces.29 The WHO has established the Solidarity Trial to coordinate international COVID-19-related research and development. Participating parties, including countries, pharmaceutical companies, and nongovernmental organizations, agree to openly share virus information and commodities developed with donated specimens.30 The EU and its Member States, and nine other countries, have drafted a resolution to be considered at the upcoming World Health Assembly on a unified international COVID-19 response, including on "the need for all countries to have unhindered timely access to quality, safe, efficacious and affordable diagnostics, therapeutics, medicines and vaccines ... for the COVID-19 response."31
How are international financial institutions responding to COVID-19?32
The international financial institutions (IFIs), including the International Monetary Fund (IMF), the World Bank, and specialized multilateral development banks (MDBs), are mobilizing unprecedented levels of financial resources to support countries grappling with the health and economic effects of the COVID-19 pandemic.33 About 100 countries—more than half of the IMF's membership—have requested IMF loans, and the IMF has announced it is ready to tap its total lending capacity, about $1 trillion, to support governments responding to COVID-19.34 In April 2020, the World Bank pledged to mobilize about $160 billion through 2021, and other multilateral development banks committed about $80 billion over the same time period.35 MDB support is expected to cover a wide range of activities, including strengthening health services and primary health care, bolstering disease monitoring and reporting, training front-line health workers, encouraging community engagement to maintain public trust, and improving access to treatment for the poorest patients. In addition, at the urging of the IMF and the World Bank, the G-20 countries in coordination with private creditors have agreed to suspend debt payments for low-income countries through the end of 2020.
Policymakers are discussing a number of policy actions to further bolster the IFI response to the COVID-19 pandemic. Examples include changing IFI policies to allow more flexibility in providing financial assistance, pursuing policies at the IMF to increase member states' foreign reserves, and providing debt relief to low-income countries. Some of these policy proposals would require congressional legislation. Through the stimulus legislation (P.L. 116-136), Congress accelerated authorizations requested by the Administration in the FY2021 budget for the IMF, two lending facilities at the World Bank, and two lending facilities at the African Development Bank.
What is the U.N. humanitarian response to the COVID-19 pandemic?36
Outside of the WHO, other U.N. entities and their implementing partners are considering how to maintain ongoing humanitarian operations while preparing for COVID-19 cases should they arise.37 On March 17, 2020, the International Organization for Migration (IOM) and the U.N. High Commissioner for Refugees (UNHCR) announced they were suspending global resettlement travel for refugees due to the COVID-19 travel bans.38 Cessation of resettlement may reinforce population density in refugee camps and other settlements, which might further complicate efforts to address COVID-19 outbreaks in such settings.
Many experts agree that even prior to the COVID-19 pandemic, the scope of current global humanitarian crises was unprecedented.39 The U.N. Office for the Coordination of Humanitarian Affairs (UNOCHA) estimated that in 2020, nearly 168 million people in 53 countries would require humanitarian assistance and protection due to armed conflict, widespread or indiscriminate violence, and/or human rights violations.40 The 2020 U.N. global humanitarian annual appeal totaled an all-time high of more than $28.8 billion, excluding COVID-19 responses.41 The appeal also focused on the needs of displaced populations, which numbered more than 70 million people, including 25.9 million refugees, 41.3 million internally displaced persons (IDPs) and 3.5 million asylum seekers.42 In addition, natural disasters are also key drivers of displacement each year.43
Humanitarian experts agree that the conditions in which vulnerable, displaced populations live make them particularly susceptible to COVID-19 spread and present significant challenges to response and containment.44 Overcrowded living spaces and insufficient hygiene and sanitation facilities make conditions conducive to contagion.45 In many situations, disease control recommendations are not practical. Space is not available to create isolation and "social-distancing," for example, and limited access to clean water and sanitation make regular and sustained handwashing difficult.46 In addition, low or middle-income countries that are likely to struggle to respond effectively to the pandemic host 85% of refugees worldwide.47 So far, relatively few COVID-19 cases have been reported among the displaced and those affected by conflict or natural disasters, although there is a widespread lack of testing.48
On March 25, 2020, the United Nations launched a $2.01 billion global appeal for the COVID-19 pandemic response to "fight the virus in the world's poorest countries, and address the needs of the most vulnerable people" through the end of the year.49 According to the United Nations, as of early May, donors had so far provided $923 million toward the initial appeal and contributed $608 million outside the plan.50 On May 7, 2020, the United Nations announced it had tripled the appeal to $6.7 million and expanded its coverage to 63 countries as it became clear that COVID-19's "most devastating and destabilizing effects will be felt in the world's poorest countries."51 While the United Nations does not expect the pandemic to peak in the world's poorest countries for another three to six months, already there are reports of "incomes plummeting and jobs disappearing, food supplies falling and prices soaring, and children missing vaccinations and meals."52 The updated plan brings together humanitarian appeals from other U.N. agencies in an effort to coordinate emergency health and humanitarian responses (see Table 3).
UNOCHA will coordinate the U.N.-wide response, but most of the activities will be carried out by specific U.N. entities, non-governmental organizations, and other implementing partners. U.N. guidance for scaling up responses in refugee and IDP settings includes addressing mental health and psychological aspects, adjusting food distribution, and developing prevention and control mechanisms in schools.53 Some experts recommend incorporating COVID-19 responses within existing humanitarian programs to ensure continuity of operations and to protect aid personnel while facilitating their access in areas where travel has been restricted.54
|
Type of Response Plan |
Health |
Nonhealth |
Total |
|
Global support services |
0.0 |
0.0 |
1,010 |
|
Humanitarian Response Plans |
1,300 |
2,180 |
3,490 |
|
Regional Refugee Response Plans |
265 |
729 |
994 |
|
Regional Refugee and Migrant Response Plan |
132 |
306 |
439 |
|
Other plans |
92 |
65 |
157 |
|
New plans |
235 |
394 |
629 |
|
Total |
2,024 |
3,674 |
6,708 |
Source: UNOCHA, Global Humanitarian Response Plan COVID-19: United Nations Coordinated Appeal April – December 2020, May Update, May 7, 2020.
Notes: Each U.N. agency's role in implementing the plan is described briefly on pp. 40-43 of the above cited report.
U.S. Support for International Responses
On January 29, 2020, President Donald Trump announced the formation of the President's Coronavirus Task Force, led by the Department of Health and Human Services (HHS) and coordinated by the White House National Security Council (NSC).55 On February 27, the President appointed Vice President Michael Pence as the Administration's COVID-19 task force leader, and the Vice President subsequently appointed the head of the President's Emergency Plan for AIDS Relief (PEPFAR), Ambassador Deborah Birx, as the White House Coronavirus Response Coordinator.56 International COVID-19 response efforts carried out by U.S. federal government departments and agencies, including those in the Task Force, are described below.57
Emergency Appropriations for International Responses58
On March 6, 2020, the President signed into law P.L. 116-123, Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020, which provides $8.3 billion for domestic and international COVID-19 response.59 The Act includes $300 million to continue the CDC's global health security programs and a total of $1.25 billion for the U.S. Agency for International Development (USAID) and Department of State. USAID- and Department of State-administered aid includes the following:
- Global Health Programs (GHP). $435 million for global health responses (see "U.S. Agency for International Development (USAID)"), including $200 million for USAID's Emergency Reserve Fund (ERF).60
- International Disaster Assistance (IDA). $300 million for relief and recovery efforts in the wake of the COVID-19 pandemic.
- Economic Support Fund (ESF). $250 million to address COVID-19-related "economic, security, and stabilization requirements."
The Act also provides $1 million to the USAID Office of Inspector General to support oversight of COVID-19-related aid programming.
On March 27, 2020, President Trump signed P.L. 116-136, Coronavirus Aid, Relief, and Economic Security Act, which contains emergency funding for U.S. international COVID-19 responses, including the following:
- International Disaster Assistance (IDA). $258 million to "prevent, prepare for, and respond" to COVID-19.
- Migration and Refugee Assistance (MRA). $350 million to the State Department-administered MRA account to "prevent, prepare for, and respond" to COVID-19.
U.S. Department of State61
How does the State Department help American citizens abroad?
Section 43 of the State Department Basic Authorities Act of 1956 (P.L. 84-885; hereinafter, the Basic Authorities Act) requires the State Department to serve as a clearinghouse of information on any major disaster or incident that affects the health and safety of U.S. citizens abroad.62 The department implements this statutory responsibility through its Consular Information Program (CIP), which provides a range of products, including but not limited to country-specific information web pages, Travel Advisories, Alerts, and Worldwide Cautions. Travel Advisories range from Level 1 (Exercise Normal Precautions) to Level 4 (Do Not Travel).
On March 31, 2020, the State Department issued an updated Level 4 Global Health Advisory advising U.S. citizens to avoid all international travel due to the global impact of COVID-19.63 Level 4 Travel Advisories do not constitute a travel ban. Instead, they advise U.S. citizens not to travel because of life threatening risks and, in some cases, limited U.S. government capability to provide assistance to U.S. citizens.64 The State Department's Level 4 Global Health Advisory notes that because the State Department has authorized the departure of U.S. personnel abroad who are "at higher risk of a poor outcome if exposed to COVID-19," U.S. embassies and consulates may have more limited capacity to provide services to U.S. citizens abroad.65
CIP products are posted online and disseminated to U.S. citizens who have registered to receive such communications through the Smart Traveler Enrollment Program (STEP). The Assistant Secretary for Consular Affairs is responsible for supervising and managing the CIP. 66 State Department regulations provide that when health concerns rise to the level of posing a significant threat to U.S. citizens, the State Department will publish a web page describing the health-related threat and resources.67 The Bureau of Consular Affairs has developed such a web page for the COVID-19 pandemic.68 Additionally, the State Department has created a website providing COVID-19-related information and resources for every country in the world.69 Furthermore, on March 24, 2020, the State Department began publishing a daily COVID-19 newsletter, developed for Members of Congress and congressional staff, intended to "dispel rumor, combat misinformation, and answer any outstanding questions regarding the Department's overseas crisis response efforts."70
What are the authorities and funding for the State Department to carry out overseas evacuations?
The Omnibus Diplomatic Security and Antiterrorism Act of 1986 (P.L. 99-399) authorizes the Secretary of State to carry out overseas evacuations. Section 103 of this law requires the Secretary to "develop and implement policies and programs to provide for the safe and efficient evacuation of United States Government personnel, dependents, and private United States citizens when their lives are endangered."71 In addition, the Basic Authorities Act authorizes the Secretary to make expenditures for overseas evacuations. Section 4 of this law authorizes both expenditures for the evacuation of "United States Government employees and their dependents" and "private United States citizens or third-country nationals, on a reimbursable basis to the maximum extent practicable," leaving American citizens or third-country nationals generally responsible for the cost of evacuation, although emergency financial assistance may be available for destitute evacuees.72 Furthermore, the Basic Authorities Act limits the scope of repayment to "a reasonable commercial air fare immediately prior to the events giving rise to the evacuation."73
In practice, even when the State Department advises private U.S. citizens to leave a country, it will advise them to evacuate using existing commercial transportation options whenever possible. This is reflected in the State Department's current Level 4 Global Health Advisory, which states that "[i]n countries where commercial departure options remain available, U.S. citizens who live in the United States should arrange for immediate return."74 In more rare circumstances, when the local transportation infrastructure is compromised, the State Department will arrange chartered or non-commercial transportation for U.S. citizens to evacuate to a safe location determined by the department. Following the outbreak of COVID-19, the State Department has made such arrangements for thousands of U.S. citizens throughout the world, initially those in Wuhan, China and, shortly thereafter, U.S. citizen passengers who were quarantined on the Diamond Princess cruise ship in Yokohama, Japan. As demand for repatriation surged, the State Department leveraged new options to evacuate U.S. citizens, including "commercial rescue flights." To facilitate these flights, the department worked with the airline industry to help them secure the needed clearances to carry out evacuation flights in high-demand countries.75 The State Department said that these flights enabled it to focus its own resources to send chartered flights where "airspace, border closures, and internal curfews have been the most severe."76 While evacuations are still ongoing, the department estimated in late April that around 40% of U.S. citizens who were evacuated for reasons related to COVID-19 returned to the United States on commercial rescue flights.77
Congress authorizes funding for the evacuation-related activities through the Emergencies in the Diplomatic and Consular Service (EDCS) account, which is part of the annual Department of State, Foreign Operations, and Related Programs (SFOPS) appropriation. For FY2020, Congress appropriated $7.9 million for this account.78 Congress typically funds this account through no-year appropriations, thereby authorizing the State Department to indefinitely retain funds.79 The State Department is able to further fund emergency evacuations using transfer authorities provided by Congress. In recent SFOPS appropriations, for example, Congress has authorized the State Department to transfer and merge funds appropriated to the Diplomatic Programs, Embassy Security, Construction, and Maintenance, and EDCS accounts for emergency P.L. 116-123, evacuations.80
In addition to the funds and transfer authorities provided in annual appropriations legislation, Congress appropriated an additional $588 million for State Department operations (including $264 million appropriated through P.L. 116-123 and $324 million appropriated through P.L. 116-136) to "prevent, prepare for, and respond to coronavirus," including by carrying out evacuations. P.L. 116-123 also increased the amount of funding the State Department is authorized to transfer from the Diplomatic Programs account to the EDCS account for emergency evacuations during FY2020 from $10 million to $100 million.81
How many evacuations have been carried out due to the COVID-19 pandemic?
The State Department began arranging evacuations of U.S. government personnel and private U.S. citizens in response to the COVID-19 pandemic on January 28, 2020, when the department started evacuating over 800 American citizens from Wuhan, China. An additional 300 American citizens who were passengers aboard the Diamond Princess cruise ship were subsequently evacuated in February. When COVID-19 continued to spread and was declared a global pandemic by WHO, the State Department accelerated its efforts to evacuate Americans amid actions by countries to close their borders and implement mandatory travel restrictions. On March 19, 2020, the State Department established a repatriation task force to coordinate and support these efforts. As of May 11, 2020, the State Department had coordinated the repatriation of more than 85,000 Americans on 886 flights.82 The State Department's current Level 4 Global Health Advisory warns that while the department is "making every effort to assist U.S. citizens overseas who wish to return to the United States, funds "may become more limited or even unavailable."83 Some Members of Congress have applauded the State Department's efforts to scale up consular assistance to U.S. citizens abroad during the COVID-19 pandemic. Other Members have expressed concern that as COVID-19 spread worldwide, the State Department was slow to communicate with and provide options to Americans abroad seeking repatriation.84
U.S. Agency for International Development (USAID)85
Where is USAID providing COVID-19 assistance?
USAID is providing assistance to more than 100 affected and at-risk developing countries facing the threat of COVID-19.86 USAID identified these countries through a combination of the following criteria:
- trend of increasing confirmed cases of COVID-19, especially with evidence of local transmission;
- imported cases with high risk for local transmission due to connectivity to a hotspot;
- low scores on the Global Health Security Index87 classification of health systems and on the Global Health Security Agenda Joint External Evaluation, which measures compliance with IHR (2005);
- other vulnerabilities (unstable political situation, displaced populations); and
- the existence of other U.S. global health programs that could be leveraged.
USAID is also providing funding to multilateral organizations, including the WHO, UNICEF, and the International Federation of the Red Cross and Red Crescent Societies for COVID-19 assistance, and to facilitate coordination with other donors.
What type of assistance does USAID provide for COVID-19 control?
On February 7, 2020, USAID committed $99 million from the Emergency Reserve Fund (ERF) for Contagious Infectious Diseases. USAID received $986 million from the first emergency supplemental appropriation and an additional $353 million from the second. Examples of activities to which USAID resources will be programed include
- assisting target countries to prepare their laboratories for COVID-19 testing,
- implementing a public-health emergency plan for points of entry,
- activating case-finding and event-based surveillance for influenza-like illnesses,
- training and equipping rapid-response teams,
- investigating cases and tracing the contacts of infected persons, and
- adapting health worker training materials for COVID-19.
As of May 1, 2020, USAID pledged to provide $653 million for international COVID-19 response, $215 million of which has been obligated.88 The pledged amounts include $99 million from the ERF, $100 million from the Global Health Programs (GHP) account, $300 million in humanitarian assistance from the International Disease Assistance (IDA) account, and $153 million from the Economic Support Fund (ESF).
How do USAID COVID-19 responses relate to regular pandemic preparedness activities?
Congress appropriates funds for USAID global health security and pandemic preparedness activities through annual State, Foreign Operations, and Related Programs appropriations (Table 4). From FY2009 through FY2019, the bulk of USAID's pandemic preparedness activities have been implemented through the Emerging Pandemic Threats (EPT) program. Those efforts comprised USAID's contribution towards advancing the Global Health Security Agenda (see "International Health Regulations") and are being leveraged for COVID-19 responses worldwide. Key related activities include
- strengthening surveillance systems to detect and report disease transmission;
- upgrading veterinary and other national laboratories;
- strengthening programs to combat antimicrobial resistance (AMR) in the public health and animal-health sectors;
- training community health volunteers in epidemic control and designing community-preparedness plans;
- conducting simulation exercises to prepare for future outbreaks; and
- establishing or strengthening emergency supply-chain programs specially designed to deliver critically needed commodities (e.g., personal protective equipment) to affected communities during outbreaks.
The PREDICT project was a key part of the EPT program. According to USAID, the second phase of the project, PREDICT-2 (2015-2019), helped nearly 30 countries detect and discover viruses with pandemic potential. The project has
- detected more than 1,100 unique viruses, 931 of which were novel viruses (such as Ebola and coronaviruses);
- sampled over 163,000 animals and people; and
- provided $207 million from 2009 through 2019.
USAID has responded to 42 outbreaks through PREDICT-2, which ended in March 2020 (following a three-month extension). In May 2020, USAID announced that it will use the lessons learned through PREDICT to inform its new STOP Spillover project. The STOP Spillover project is aimed at building capacity in partner countries to stop the spillover of zoonotic diseases into humans. USAID aims to "award the STOP Spillover project by the end of September 2020, through a competitive process, as PREDICT sunsets as scheduled."89
Table 4. USAID Global Pandemic Preparedness Funding: FY2017-FY2021 Request
(current U.S. $ millions)
|
Fiscal Year |
Amount |
|
FY2017 Enacted |
72.5 |
|
FY2018 Enacted |
72.5 |
|
FY2019 Enacted |
100.0 |
|
FY2020 Enacted |
100.0 |
|
FY2021 Requested |
115.0 |
Source: Congressional budget justifications and appropriations legislation.
Notes: Excludes emergency appropriations for controlling the 2014-2016 Ebola outbreak in West Africa.
U.S. Centers for Disease Control and Prevention (CDC)90
What role is CDC playing in international COVID-19 responses?
CDC has staff stationed in more than 60 countries who have been providing technical support, where relevant, and is receptive to bilateral requests for assistance or requests for assistance through the Global Outbreak Alert and Response Network (GOARN). CDC is working with WHO and other partners, including USAID and the Department of State, to assess needs and accelerate COVID-19 control, particularly by helping countries to implement WHO recommendations related to the diagnosis and care of patients, tracking the epidemic, and identifying people who might have COVID-19.
Through supplemental appropriations (P.L. 116-123), Congress provided CDC $300 million for global disease detection and emergency response. CDC plans to obligate $150 million of the funds by the end of FY2020. Related efforts will focus on
- disease surveillance,
- laboratory diagnostics,
- infection prevention and control,
- border health and community mitigation, and
- vaccine preparedness and disease prevention.
CDC is reportedly working closely with USAID and Department of State to ensure a coordinated U.S. government approach to the COVID-19 pandemic. CDC is prioritizing countries based on
- the current status of COVID-19 in country and future trajectory of its spread;
- the ability to effectively implement activities given CDC presence, capacity and partnerships in the country; and
- the capacity to provide support to other countries in the region.
CDC staff are working with colleagues in partner countries to conduct investigations that will help inform COVID-19 response efforts.
How do CDC COVID-19 responses relate to regular pandemic preparedness activities?
Through the Global Health Protection line item of annual Labor-HHS appropriations, CDC works to enhance public health capacity abroad and improve global health security, particularly through GHSA (Table 5). CDC works to bolster global health security and pandemic preparedness in 19 countries by focusing on enhancing the core foundations of what CDC views as strong public health systems—comprehensive disease surveillance and integrated laboratory systems, a strong public health workforce, and capable emergency management structures.
Programs within CDC's global health security portfolio include the following:
- The Field Epidemiology Training Program (FETP) trains a global workforce of field epidemiologists to increase countries' ability to detect and respond to disease threats, address the global shortage of skilled epidemiologists, and deepen relationships between CDC and other countries. Over 70 countries have participated in FETP with more than 10,000 graduates.
- National Public Health Institutes (NPHI) help more than 26 partner countries carry out essential public health functions and ensure accountability for public health resources. The program focuses on improving the collection and use of public health data, as well as the development, implementation, and monitoring of public health programs.
- Global Rapid Response Team (GRRT) is a team of public health experts who remain ready to deploy for supporting emergency response and helping partner countries achieve core global health capabilities. The GRRT focuses on field-based logistics, communications, and management operations. Since the GRRT's inception, more than 500 CDC staff have provided over 30,000 person-days of response support. From January through March 2020, CDC staff has completed more than 100 deployments for COVID-19 response. Core and surge members support domestic deployments to quarantine stations and repatriation sites, international deployments, WHO and country office operations, and the Emergency Operations Center in Atlanta.
- The Public Health Emergency Management (PHEM) program trains public health professionals affiliated with international ministries of health on emergency management and exposes them to the CDC Public Health Emergency Operations Center. To date, the program has graduated 142 fellows from 37 countries (plus the African Union).
|
Fiscal Year |
Amount |
|
FY2017 Enacted |
58.2 |
|
FY2018 Enacted |
108.2 |
|
FY2019 Enacted |
108.2 |
|
FY2020 Enacted |
183.2 |
Source: Correspondence with CDC, March 27, 2020.
Notes: In the Labor, HHS Appropriations, these activities are described as Global Public Health Protection. For the purposes of this report, these activities are referred to as pandemic preparedness.
U.S. Department of Defense (DOD)
What is the DOD global COVID-19 response?91
DOD is conducting medical surveillance for COVID-19 worldwide.92 Related activities entail daily monitoring of reported cases, including persons under investigation (PUI), confirmed cases, and locations of such individuals,93 as well as surveillance for COVID-19 at China's southern border.94 DOD is supporting the U.S. CDC with additional laboratory capabilities. The DOD Laboratory Network, which includes military facilities in the United States and in certain overseas locations, has made available to interagency network laboratories its "detection and characterization capabilities … to support COVID-19-related activities across the globe."95 The Secretary of Defense also has directed geographic combatant commanders96 to "execute their pandemic plans in response to the [COVID-19] outbreak."97
Emergency Appropriations for DOD Responses98
The Families First Coronavirus Response Act (P.L. 116-127) became law on March 18, 2020. Title II of Division A of the act included $82 million for the Defense Health Program to waive all TRICARE cost-sharing requirements related to COVID-19.99
The Coronavirus Aid, Relief, and Economic Security Act (CARES Act; P.L. 116-136) became law on March 27, 2020. Title III of Division B of the act included $10.5 billion in emergency funding for DOD. Of the $10.5 billion, $4.9 billion (47%) is for the Defense Health Program (DHP), according to the bill text. The DHP funding included $1.8 billion for patient care and procurement of medical and protective equipment; $1.6 billion to increase capacity in military treatment facilities; $1.1 billion for private-sector care; and $415 million to develop vaccines and to procure diagnostic tests, according to a summary released by the Senate Appropriations Committee.100 H.R. 748 also provided
- $2.5 billion for the defense industrial base, including $1.5 billion in defense working capital funds and $1 billion in Defense Production Act purchases;
- $1.9 billion in operations and maintenance (O&M) funding for the Services, in part to support deployment of the hospital ships USNS COMFORT and USNS MERCY to ease civilian hospital demand by caring for non-COVID patients; and
- $1.2 billion in military personnel (MILPERS) funding for Army and Air National Guard personnel deployments.
DOD has not detailed how much of the emergency funding may be used to support international activities related to COVID-19, though DOD has stated it is working with the Department of Health and Human Services and the Department of State to provide support in dealing with the pandemic.101 As part of missions that began in March, Air National Guard C-17 cargo aircraft have transported hundreds of thousands of coronavirus testing swabs from Italy to the United States.102 The swabs have been distributed to medical facilities around the country at the direction of the Department of Health and Human Services.103
To what extent is COVID-19 affecting United States security personnel?104
The degree to which U.S. security operations around the world may be affected due to personnel becoming infected has yet to be determined.105 Numerous media reports suggest that various parts of the U.S. military have seen a significant number of servicemembers contract or die from COVID-19 related symptoms. Citing operational security concerns, on March 30, 2020 the Department of Defense (DOD) directed military service commanders not to share the number of personnel affected by the COVID-19. In justifying this policy the DOD stated, "We will not report the aggregate number of individual service member cases at individual unit, base or Combatant Commands. We will continue to do our best to balance transparency in this crisis with operational security."106 Also, as of April 1, 2020, reportedly the Department of Homeland Security had nearly 9,000 employees whose exposure to COVID-19 that has taken them out of the workforce,107 and deployed U.S. Naval vessels, such as the USS Theodore Roosevelt, have had their operational effectiveness called into question.108
Regional Implications of and Responses to the COVID-19 Pandemic
Asia
What are the implications for U.S.-China relations?109
U.S.-China relations were fraught well before the outbreak of COVID-19, with the two governments engaging in a bitter trade war, competing for influence around the globe, and clashing over such issues as their activities in the South China Sea, China's human rights record, and China's Belt and Road Initiative. The pandemic appears to have increased the acrimony. On February 3, when the COVID-19 outbreak was at its peak in China, a spokesperson for China's Foreign Ministry blasted the United States for its response to the crisis there. "The U.S. government hasn't provided any substantive assistance to us, but it was the first to evacuate personnel from its consulate in Wuhan, the first to suggest partial withdrawal of its embassy staff, and the first to impose a travel ban on Chinese travelers," the spokesperson charged. "What it has done could only create and spread fear."110 Days later, Secretary of State Michael R. Pompeo announced the United States would make available up to $100 million in existing funds "to assist China and other impacted countries," and that the State Department had facilitated the delivery to China of 17.8 tons of personal protection equipment and medical supplies donated by the private sector.111
As COVID-19 transmission has accelerated in the United States, the Trump Administration has stepped up criticism of China's early response to the outbreak. Secretary Pompeo told an interviewer on March 24, "unfortunately, the Chinese Communist Party covered this up and delayed its response in a way that has truly put thousands of lives at risk."112 Spokespeople for the State Department and China's Foreign Ministry have traded COVID-19-related accusations on Twitter. On March 12, a Chinese spokesperson tweeted, "It might be US army who brought the epidemic to Wuhan."113 Secretary Pompeo accused China of waging a disinformation campaign "designed to shift responsibility," and President Trump for several days referred to COVID-19 as "the Chinese virus."114
On April 17, in announcing his decision to withhold U.S. funding from the World Health Organization, President Trump accused the multilateral institution of having "pushed China's misinformation about the virus, saying it was not communicable and there was no need for travel bans."115 Administration officials have also repeatedly suggested that a Chinese research institution may have been the source of the virus.116 On April 30, 2020, when asked if he had seen anything "that gives you a high degree of confidence that the Wuhan Institute of Virology was the origin of the virus," the President replied, "Yes, I have."117 The same day, the Office of the Director of National Intelligence stated that the intelligence community would continue efforts "to determine whether the outbreak began through contact with infected animals or if it was the result of an accident at a laboratory in Wuhan," indicating continuing uncertainties about the virus's origin.118
China has pushed back against U.S. allegations, including in a "Reality Check" document tweeted by a Chinese Foreign Ministry spokesperson responding to 24 U.S. allegations, which the spokesperson calls "lies."119 (The document argues, for example, that the Wuhan Institute of Virology "does not have the capability to design and synthesize a new coronavirus, and there is no evidence of pathogen leaks or staff infections in the Institute.") Chinese spokespeople have gone on the offensive in criticizing the U.S. response to COVID-19 and have doubled down on spreading a conspiracy theory that the virus could have originated in the United States. On May 8, a Chinese Foreign Ministry spokesperson tweeted, "The #US keeps calling for transparency & investigation. Why not open up Fort Detrick & other bio-labs for international review? Why not invite #WHO & int'l experts to the U.S. to look into #COVID19 source & response?"120
Some U.S.-based analysts have expressed alarm about the downward spiral in bilateral relations. Some see neither the United States nor China helping to coordinate a global response to the pandemic, and argue, "U.S.-China strategic competition is giving way to a kind of 'managed enmity' that is disrupting the world and forestalling the prospect of transnational responses to transnational threats."121 Others suggest, "There will be time later to assess the early mistakes of China and others in greater detail, but the virus is out there now and we should be tackling it together." Some have called for cooperation in vaccine development and distribution, and in addressing the economic crisis the virus is causing in the developing world."122
Writing in The Washington Post, China's Ambassador to the United States suggested on May 5 that China would still be open to cooperation. "Blaming China will not end this pandemic," he wrote. "On the contrary, the mind-set risks decoupling China and the United States and hurting our efforts to fight the disease, our coordination to reignite the global economy, our ability to conquer other challenges and our prospects of a better future."123 In a May 14, 2020, Fox News interview, President Trump said, however, that he had no desire to speak to China's leader Xi Jinping. He suggested that to punish China, "we could cut off the whole relationship." Apparently referring to the U.S. trade deficit with China, which was $378.6 billion in 2019, the President added, "You'd save $500 billion if you cut off the whole relationship."124
Several Members of Congress have introduced legislation criticizing China's response to the COVID-19 pandemic (see Appendix).
What are the implications in Southeast Asia?125
Southeast Asia was one of the first regions to experience COVID-19 infections and the outbreak could have broad social, political, and economic implications in the months ahead and possibly years ahead. The region's countries are deeply tied together through trade and the movement of labor, links that could be reshaped if the outbreak leads to broad policy changes. Their economies have already been affected by disruptions to these links, and broad economic networks and supply chains could be reshaped if the outbreak leads to broad policy changes.
As an example, Malaysia banned overseas travel on March 18, affecting approximately 300,000 Malaysians who work in neighboring Singapore. Malaysia, however, changed tack on April 14 and allowed Malaysians in Singapore to return if they agreed to be tested and placed in quarantine. In Singapore, widespread outbreaks among migrant laborers, mostly from South Asia, who live in crowded dormitories, have led to the region's largest number of COVID-19 infections.
Other regional issues include the following:
- Indonesia and the Philippines, the region's two most populous nations, appear to be experiencing widening outbreaks and may have a significantly larger COVID-19 case count than their public health systems are able to detect and address.126
- Malaysia and Thailand, which have undergone substantial political turmoil in recent years, have relatively new governments that could face legitimacy questions based on their responses to the pandemic and as their economies begin the process of opening.127
- Some nations, including the Philippines and Cambodia, have taken actions that raise concerns about human rights and freedoms. Philippine President Rodrigo Duterte has imposed strict lockdown measures that one U.N. official criticized as "highly militarized," and these measures have resulted in more than 120,000 arrests, disproportionally affecting poor urban residents.128 Human rights groups have criticized a draft emergency order by Cambodia's government that would give it greater control over traditional and social media.129
- Some of the region's poorest countries, including Burma and Laos, have reported relatively few COVID-19 cases, highlighting questions about transparency in nations that may be particularly vulnerable given their underdeveloped health systems.
Much of the Southeast Asian diplomatic calendar, which drives regional cooperation on a wide range of issues including trade and public health, has been cancelled or has moved to virtual meetings. The International Institute for Strategic Studies (IISS) has cancelled this year's iteration of its annual Shangri-la Dialogue, slated for June 5-7, after consultations with the government of Singapore.130
What are the implications in Central Asia?131
In Central Asia, the economic impacts of the pandemic may affect the roles of Russia and China in the region. Given disruptions to trade and cross-border movement, the pandemic could reverse recent progress on regional connectivity, a U.S. policy priority in Central Asia. The COVID-19 pandemic is placing significant economic pressure on Central Asian countries due to declines in domestic economic activity, economic disruptions in China and Russia, and the fall in hydrocarbon prices. China has cut the volume of natural gas imports from Central Asia due to falling demand, and analysts speculate that Chinese investment in the region may also shrink. Turkmenistan sends almost all of its gas exports to China and is particularly vulnerable, as the Turkmen government uses gas exports to service billions of dollars of Chinese loans. The economic impact of the pandemic will likely interrupt the flow of remittances from Russia, where millions of Kyrgyz, Tajik, and Uzbek citizens work as labor migrants, accounting for significant percentages of their countries' GDPs.132
Some measures implemented to combat the spread of COVID-19 could provide governments in the region with the means to suppress political and media freedoms. Human Rights Watch has stated that Central Asian governments are failing to uphold their human rights obligations by limiting access to information and arbitrarily enforcing pandemic-related restrictions. In Kazakhstan, authorities have detained government critics and journalists on suspicion of "disseminating knowingly false information during a state of emergency," a charge that can be punished by up to seven years in prison. Kyrgyz authorities restricted the ability of independent media outlets to report for over a month using provisions in the country's state of emergency. The government of Tajikistan has been suppressing information on the pandemic, refusing to answer media questions and blocking a website that crowdsources information on COVID-19 fatalities in the country.133
What are the implications in South Asia?134
The seven countries of South Asia are home to about 1.8 billion people, nearly one-quarter of the world's population. In most South Asian countries, per capita spending on health care is relatively low and medical resources and capacities are limited.135 Dense populations and lack of hygiene are facilitating factors for pandemics, and with medical equipment needed to address the crisis in short supply, South Asia nations are likely to face serious risk.136 As of May 1, 2020, the United States had provided nearly $6 million in health assistance to help India slow the spread of COVID-19 and nearly $15 million to assist Pakistan's response.137
The COVID-19 crisis has put a broad hold on activities related to U.S.-India and regional multilateral security cooperation, as well as delayed sensitive negotiations on U.S.-India trade disputes. The postponement of a planned March visit to New Delhi by Secretary of Defense Mark Esper had led to worries by some of inertia in bilateral defense relations.138 With India and Pakistan still engaged in a deep-rooted militarized rivalry, any generalized South Asian crisis, especially in the disputed region of Kashmir, could lead to societal breakdowns and/or open interstate conflict between these two nuclear-armed countries.
India. Several U.S. and Indian firms are cooperating on research for a coronavirus vaccine.139 India is home to several major vaccine manufacturers and is the world's leading producer of hydrocholoquine, an anti-malarial drug President Trump has touted as a potential treatment for COVID-19. In April, the U.S. President suggested that the United States might retaliate against India if New Delhi bans export of the drug and fails to fulfill an existing large-scale U.S. purchase order. India has agreed to allow limited exports.140
The COVID-19 crisis has led to more acute questioning of the political leadership in India, where since last year Prime Minister Narendra Modi has faced mass protests over new citizenship laws and persecution of Muslims. Reports indicate that the health pandemic is fueling greater oppression and persecution of Indian Muslims, with that community coming under blame for the pandemic from some quarters. Accusations also have arisen that the New Delhi government is using the pandemic as a cover for increased efforts to limit press freedoms. India's Jammu and Kashmir territory—which came under a strict security lockdown in August 2019 and lost statehood in November—reportedly faces a "double lockdown" with the pandemic and resulting severe physical and psychological hardships. The New Delhi government may be using the pandemic as cover to further consolidate its grip on the disputed Kashmir Valley.141
In Pakistan, Prime Minister Imran Khan was already dealing with widespread disaffection related to his government's performance and legitimacy. In late March, the powerful military "stepped in and sidelined" the civilian leadership after the Khan government's national pandemic response was criticized for perceived indecisiveness. By some accounts, the Pakistan government has also "caved in to the demands of clerics" regarding lockdown regulations.142
In Bangladesh, social distancing is difficult for many living in densely populated areas. In addition, over 1 million displaced Rohingya reside in overcrowded and unsanitary camps along Bangladesh's border with Burma. Of these Rohingya, approximately 630,000 live in the Kutupalong camp, which may be the world's largest refugee camp. The population density in the camps—104,000 people per square mile in Kutupalong—poses challenges for social distancing, quarantine, and isolation. Any COVID-19 transmission in the camps would likely quickly overwhelm medical facilities and services, and because of the camps' porous perimeters, risk spreading into neighboring Bangladeshi towns and villages.143 Bangladesh reportedly quarantined a number of Rohingya on Bhansan Char island to prevent the spread of COVID-19.144
What are the implications in Australia and New Zealand?145
In both Australia and New Zealand, relations with China have been further strained by the COVID-19 pandemic. In April 2020, Australia expressed its support for an international investigation into the origins and spread of the pandemic, a call that raised sensitivities in the PRC.146 China's Ambassador Cheng Jingye in an Australian newspaper interview warned "that pursuing an inquiry could spark a Chinese consumer boycott."147 Opposition Foreign Affairs spokesperson Penny Wong has signaled Labor's support of the government on the issue. In the view of one commentator, such attempts at "intimidation" and "economic coercion" make it "now plain for all to see that the CCP is waging political war on Australia, using trade as a weapon. This is Australia's moment of clarity."148
In May, China berated New Zealand for supporting Taiwan's participation at the World Health Organization.149 New Zealand Foreign Minister Winston Peters stated, "[w] e have to stand up for ourselves" when asked about China's response to New Zealand's position on Taiwan.150
What are the implications for U.S. withdrawal from Afghanistan?151
The presence and spread of COVID-19 in Afghanistan is adding new confusion to the Afghan peace process, already complicated by an extended political crisis in Kabul. The February 29, 2020 agreement signed by U.S. and Taliban negotiators commits the United States to withdraw about 3,500 of the 12,000 troops it has in Afghanistan by mid-June 2020 (with commensurate drawdowns of international forces). There have since been conflicting reports about how the COVID-19 pandemic is impacting that timeline. Most notably, the United States announced on March 18 that it is pausing the movement of personnel into and out of theater due to concerns about COVID-19.152 More recent reports indicate that the withdrawal is proceeding apace, if not ahead of schedule, and NBC News reported in April 2020 that President Trump has called for further accelerating the withdrawal of U.S. troops out of Afghanistan because of the pandemic.153 The U.S.-Taliban agreement also called for negotiations between the Taliban and Afghan government representatives to begin by March 10, but thus far no formal negotiations have taken place or been scheduled. Some limited engagements were held over Skype, due to the pandemic, but talks are chiefly held up by a disputed prisoner exchange.154
Further spread of COVID-19 in Afghanistan could present opportunities for compromise and intra-Afghan cooperation. For example, Afghan government representatives have expressed support for Taliban efforts to combat the virus in areas they control.155 In addition, while the Taliban have reportedly targeted health workers in the past, a Taliban spokesman announced that the group "assures all international health organizations and WHO of its readiness to cooperate and coordinate with them in combatting" COVID-19, a commitment they appear to have upheld.156 At the same time, some observers dismiss the Taliban's response as a propagandistic attempt to undermine the legitimacy of the Afghan government, and charge that the Taliban's dramatic escalation of violence since February 2019 is the main factor impeding the country's response to the pandemic.157 Afghanistan may be at particularly high risk of a widespread COVID-19 outbreak, due in part to its weak public health infrastructure and its porous border with Iran, a regional epicenter of the pandemic where up to three million Afghan refugees live. More than 277,000 Afghans have returned to Afghanistan from Iran since January 1, 2020.158
What COVID-19 containment lessons could be learned from Asia?
Asian governments outside mainland China were the first to deal with COVID-19. Five jurisdictions, in particular, have received wide praise for their COVID-19 control approaches: Taiwan, Hong Kong, South Korea, Australia, and New Zealand. Singapore was also praised for its initial actions to control the virus, although a large "second wave" of infections has pointed to vulnerabilities that even jurisdictions perceived as well-run still face. All of these jurisdictions have drawn on their experiences in addressing previous public health emergencies, including outbreaks caused by SARS, swine and avian flu, and MERS. Those experiences fostered bureaucratic and public attentiveness to public health challenges and prompted governments to develop active protocols for screening, testing, isolating infected individuals, and tracing their contacts. Prior experience may also have conditioned people in those places to follow standard infection control measures (frequent hand-washing, mask-wearing, and social distancing) and to more readily accept quarantines and movement restrictions. Some of these jurisdictions have begun the process of loosening restrictions related to COVID-19, which may provide lessons for the United States and others.
Taiwan.159 Taiwan (which officially calls itself the Republic of China, or ROC), is located just 81 miles off the coast of mainland China. On December 31, 2019, the same day China notified the WHO China Office of pneumonia cases of unknown origin, Taiwan officials had begun to board planes arriving from Wuhan to evaluate passengers who had fever or pneumonia symptoms.160 Travel alerts, routine passenger screenings, and directives to self-quarantine soon followed, and by early February, Taiwan barred residents of mainland China from entry. Taiwan also extended indefinitely a suspension of cross-Strait flights from all but five airports in mainland China, previously set to expire at the end of April.161 On January 20, Taiwan both confirmed its first COVID-19 case and activated a Central Epidemic Command Center (CECC) to lead and coordinate the government's response to the COVID-19 crisis.162 The CECC is part of the National Health Command Center, a 24/7 central command headquarters created in 2004 following the SARS outbreak.163 The government also integrated its national health insurance, customs, and immigration databases to facilitate case identification and tracking.164 The concentration of public health expertise among Taiwan's top leaders likely contributed to the government's attentive response. Taiwan's vice president, vice president-elect, vice premier, and minister of health are all public health experts.165
The government has also issued strict and transparent guidance to contain the spread of the virus, which its citizens largely appear to have followed. Taiwan has tested widely for the virus, including mandatory tests for certain groups and tests for patients with respiratory illnesses that tested negative for the flu.166 Directives to conduct "self-health management" or self-quarantine have been enforced by harnessing cellphone location data and punishing violators with steep fines.167 The government's daily press conferences and frequent broadcasts of public service announcements have heightened public awareness and facilitated compliance with best practices.168 Taiwan also created informational apps, to help citizens track the spread of the virus and locate supplies of masks.169 In February and March, the government announced economic relief and stabilization measures, including approximately USD$2 billion to assist Taiwan industries affected by the outbreak, and payments totaling $465 to individuals who were quarantined or providing care for the quarantined.170
Hong Kong.171 Initially, the government of Hong Kong, a Special Administrative Region (HKSAR) of the People's Republic of China, resisted taking aggressive measures to prevent a COVID-19 outbreak. Public criticism of what many considered an insufficient and inconsistent initial response appears to have contributed to the government's subsequent decision to act. A newly formed union of doctors and nurses working for the Hong Kong Hospital Authority held a strike on February 3, 2020, demanding the HKSAR government close the city's border with mainland China, for example.172 The HKSAR government closed all but two of the land crossings with mainland China the next day. The government implemented a mandatory 14-day quarantine for all arrivals to Hong Kong on March 17, 2020, which remains in effect.173 The HKSAR government has also indefinitely closed Hong Kong's borders to all non-resident arrivals (except people from Mainland China, Macau and Taiwan who have not been to another country in the previous 14 days).174 The government has also developed an extensive range of public service announcements, web pages, and other modes of informing the public about COVID-19.175
Although the HKSAR government may have hesitated, Hong Kong's public quickly adopted social distancing and anti-contamination behaviors developed during previous viral outbreaks. Similarly, medical professionals quickly implemented anti-viral protocols.176
After 14 days without a confirmed local case of contagion and only a few "imported cases," on May 5, 2020, the HKSAR government began to selectively relax its restrictions, reopening government offices and selective businesses while maintaining the requirement to wear masks in public and prohibiting gatherings of more than eight people.177 The same day, it also announced that it would provide every Hong Kong resident with a free reusable face mask that complies with the American Society for Testing & Materials F2100 Level 1 Standard in terms of particle and bacterial filtration efficiency.178 The HKSAR government, however, also noted that restrictions may be reinstated if there is an increase in local cases.
Singapore.179 Singapore, a Southeast Asian city-state of 5.7 million people, has offered lessons perceived as both positive and cautionary in its handling of the pandemic. Singapore was one of the first nations outside China to report COVID-19 cases, with its first infection reported on January 23. Public health experts have praised Singapore's rapid early actions, including extensive monitoring of cases and their contacts, temperature checks at building entrances, and clear public messaging. Singapore health officials conducted detailed interviews of affected individuals, requiring those who had come into contact with them to quarantine themselves. The Health Ministry developed the capacity to test more than 2,000 individuals a day.180 Individuals who come within two meters of an infected individual or spend 30 minutes with one are required to undergo testing and to quarantine or be placed under observation. Individuals found to have misled health officials are subject to criminal penalties including fines and the threat of imprisonment.181 The Health Ministry issues daily updates on individual cases and the numbers of people under care or protective quarantine, including details of where each individual who has tested positive lives.
Despite its early successes curbing the spread, Singapore has experienced a significant "second wave" of cases, leading authorities to close schools and most businesses, steps that they had avoided earlier.182 Many of the new cases have come from crowded quarters where migrant workers live, and the expansion has left Singapore with Southeast Asia's largest number of COVID-19 infections, as of May 11.183
South Korea.184 After cases were confirmed in South Korea in late January, authorities pursued an aggressive testing regimen and public communication strategy. South Korea describes its strategy as the three "T"s: tracking, testing, and treatment. By early May, the number of new cases per day had fallen to 6.4.185 As of early May, nearly 660,000 citizens had been tested for the virus186—the highest rate of testing per capita in the world—at over 600 sites, including pop-up facilities and drive-through sites.187 Results are generally provided within 24 hours.188 The case fatality ratio (1.64% as of March 30) has also been low, which health officials attribute to early detection and treatment, as well as universal health care.189 As of early May, South Korea has been able to stabilize the outbreak without lockdowns or wholesale travel bans, in part, experts argue, by being transparent and disseminating information about the virus' spread, including possible infections at the neighborhood level. President Moon Jae-in has stepped aside to allow national health officials to take the lead in delivering twice-daily messages to the public. After MERS killed 38 people in 2015, South Korea reformed its health policy by granting the government greater powers to monitor and track individual patients and to allow private companies to rapidly produce tests. Shortly after the COVID-19 outbreak hit, authorities were able to test 10,000 patients daily.190 Authorities can now test over 20,000 patients per day.191
Australia.192 Observers believe that Australia's mitigation efforts (including self-isolation, movement restrictions, a two-week quarantine for those entering the country), the public's general adherence to rules, and widespread testing and tracing of contacts may be responsible for a relatively successful effort to contain the pandemic in Australia.193 Australia reportedly has one of the highest per capita testing rates in the world.194 In April 2020, the Australian government launched "Covidsafe," an application that traces every person running it with other application users that have tested positive for COVID-19. Using Bluetooth, the app records others that have been within 1.5 meters for 15 minutes or more who also have the app.195 Within three days of its release, 3 million Australian had reportedly signed up for the app.196
New Zealand.197 New Zealand confirmed its first case of coronavirus on February 28, 2020. The late date of the first outbreak, New Zealand's relative isolation, swift early response, and widespread testing all appear to have helped New Zealand to effectively deal with the virus.198 On March 14, with only six confirmed COVID-19 cases in the country, Prime Minister Jacinda Ardern announced that all entering New Zealand would have to self-isolate for two weeks and that the existing travel ban for those coming from China and Iran would remain in place.199 From March 19, the New Zealand border has been closed to almost all travelers, with only New Zealand citizens, residents, and their immediate families allowed to enter the country.200 This was a significant move for the country, which has an estimated 4 million international visitors a year,201 and where tourism accounted for approximately 5.8% of GDP for the year ending March 2019.202 Since April 9, arrivals have been placed in "managed isolation facilities," and those deemed to be high risk have been placed in quarantine facilities.203
New Zealand has moved from lockdown to an easing of restrictions in a relatively short period of time. Prime Minister Ardern announced on March 23 that New Zealand would enter a level 4 lockdown204 on March 25, when it had less than 150 cases.205 New Zealand then moved to alert level 3 on April 27. It subsequently moved to alert level 2 on May 13, under which most businesses will be open, tertiary education will open, travel between regions of the country, and gatherings up to 10 people will be allowed. Border controls and physical distancing requirements will remain, wide scale testing will continue, and those unwell or who have been in contact with the sick will be isolated.206 New Zealand and Australia have reached an agreement to lift travel restrictions between their two countries and establish a Trans-Tasman COVID Safe Zone, or travel bubble, as soon as it is safe to do so.207
Europe208
How are European governments and the European Union (EU) responding?
On March 13, 2020, WHO officials characterized Europe as the new global epicenter of the COVID-19 pandemic, noting that more cases were being reported each day in Europe than were reported in China at the height of its epidemic.209 As of May 15, about 1.2 million infections and nearly 155,000 deaths had been reported across the 27-member European Union (EU) and United Kingdom (UK).210 Italy, Spain, and the UK have been particularly hard hit, but infection rates grew across Europe throughout the month of March. Ukraine, Russia, and other parts of the former Soviet Union also reported a growing number of new COVID-19 cases.
Since mid-April, a growing number of European governments have expressed cautious optimism that their countries have passed the peak of the crisis. Many European countries, including France, Germany, Italy, and Spain, have announced and begun to implement staged "re-opening" plans, slowly rolling back some of the "lockdown" measures implemented in March. Government officials caution, however, that reopening measures are strictly conditions-based and could be halted if infection rates grow.
European leaders have characterized the pandemic as Europe's biggest challenge since the Second World War, with potentially severe economic consequences and far-reaching social and political implications beyond the public health impact.211 European governments and the EU are enacting an array of policy responses. Authorities in most European countries initially imposed strict limitations on the movement of people and are undertaking significant fiscal and monetary measures. Key measures taken in Europe to combat the pandemic include the following:
- Initial "lockdowns" transitioning to cautious reopening. On March 9, Italy became the first country to impose a nationwide quarantine, prohibiting "non-essential" movement within the country and closing all non-essential businesses; France, Germany, the United Kingdom, and others followed with similar restrictions. Almost all European countries closed schools and some types of businesses and have restricted public gatherings to varying degrees. Numerous European governments mobilized their military forces to assist response efforts, including constructing makeshift hospitals. In some countries, government authorities scaled back public transportation and introduced curfews.
- In mid-April, some European countries began announcing plans for a gradual reopening of their societies and economies in the coming months, but the pace of reopening measures vary across Europe, and leaders caution that such measures would be contingent on a clear reduction in infection rates. European governments have generally stressed the importance of a staged approach to reopening, allowing for regional differences depending on regional infection rates and hospital and testing capacity. They also have sought to implement widespread testing and contact tracing capacity.
- Economic stimulus. Many analysts predict that the COVID-19 pandemic could cause a financial crisis in Europe that might be several times worse than the 2008 global recession. European governments and the EU have announced an array of measures to mitigate a severe economic downturn. Measures include loan programs and credit guarantees for companies, income subsidies for affected workers, tax deferrals, and debt repayment deferments. On May 14, the Italian government announced a €55 billion (about $60 billion) stimulus plan. In France, President Emmanuel Macron has pledged to provide unlimited budgetary support to companies and workers, which the government says could cost upward of €45 billion ($48 billion). Germany has announced direct fiscal support of €236 billion (about $256 billion) and a €500 billion ($536 billion) loan program.212 Other countries have announced similar relief measures.
On March 18, the European Central Bank, which manages the EU's common currency (the euro), announced a Pandemic Emergency Purchase Program (PEPP) of about €750 billion ($803 billion) aimed at calming markets and stemming a debt crisis in the Eurozone (the 19 EU member states that use the euro as their currency).213 On April 9, Eurozone leaders agreed to a new financial assistance package of at least €540 billion (roughly $590 billion). This package includes access to credit lines through the European Stability Mechanism (ESM, the Eurozone's "bail-out" fund) worth approximately €240 billion ($261 billion) for health-related costs, establishment of a European Investment Bank fund to back up to €200 billion ($219 billion) in loans for businesses, and a €100 billion ($110 billion) unemployment benefit support plan. Reaching consensus on this financial package was contentious and exposed divisions among EU member states. The package does not include establishing common EU debt instruments (or "corona bonds")—one of the most controversial proposals supported by hardest-hit countries such as Italy, Spain, and France—but EU leaders will likely continue to discuss this option and other potential economic measures.214
- Border closures. Numerous European governments have enacted national border controls and some have restricted entry only to national citizens. These measures have complicated efforts to maintain the free movement of goods, services, and people (key elements of the EU's single market) on which the EU's highly integrated economy depends. National border controls and closures within the EU's internal border-free Schengen Area215—in which individuals may travel without passport checks among 22 EU member states and four non-EU countries—resulted in long delays at several borders. On March 16, 2020, EU leaders agreed to implement a temporary ban on "non-essential travel" into the EU and the Schengen Area for most foreign nationals from outside countries (including the United States), partly in an effort to preserve freedom of movement within the EU. This ban on nonessential travel into the EU and the Schengen Area is expected to remain in place until at least June 15. Many analysts contend that the disparate national reactions to the COVID-19 pandemic are endangering the EU's single market and Schengen system, with possible long-term implications for the EU's future.216
How is the pandemic affecting U.S.-European relations?
Managing the spread of COVID-19 has added new tensions to already strained U.S.-European relations. The EU—a frequent target of criticism from President Trump—expressed dismay with the announcement from the Trump Administration on March 11, 2020 of a travel ban on foreign nationals arriving in the United States from the Schengen Area. In a joint statement on March 12, EU leaders noted that COVID-19 was a global crisis that "requires cooperation rather than unilateral action" and expressed disapproval that the U.S. travel ban was imposed "without consultation."217 U.S. officials countered that the travel ban decision had to be taken quickly and was based on the WHO's assessment of sustained transmission in the Schengen Area.218 The Trump Administration subsequently extended the travel ban beyond the Schengen Area to the UK and Ireland. Nevertheless, some analysts on both sides of the Atlantic asserted that the U.S. travel ban was scapegoating the EU, threatened future U.S.-EU relations, and imperiled broader U.S.-European political and security alliances. 219
Some European leaders and EU officials also object to certain elements of the U.S. international response to the COVID-19 pandemic. Many European policymakers have criticized President Trump's decision to halt U.S. funding to the WHO pending a review of its role in allegedly mismanaging the pandemic response. EU officials have expressed concern that U.S. economic sanctions are blocking humanitarian supplies for hard-hit countries such as Iran and Venezuela. Some European officials, including in Germany and France, have complained about U.S. efforts to outbid them in the global marketplace for facemasks and other critical medical equipment. Some critics have also bemoaned the lack of coordinated U.S.-European leadership in mobilizing a global response to control the pandemic and address its wider societal and economic consequences.
Africa220
How are African governments responding?
As of May 12, 2020, all countries in sub-Saharan Africa ("Africa") except Lesotho had confirmed COVID-19-cases. South Africa had 11,000-plus cases, 25% of Africa's total. Most early cases were imported, notably from Europe, or linked to such cases. Africa's known COVID-19 caseloads have lagged those of more developed countries, and Africa's per capita incidence of COVID-19 remains very low in global comparison. Most countries in Africa, however, now have confirmed local COVID-19 transmission chains, and in some countries cases are surging.
Prevention and mitigation strategies vary considerably in the region. Many governments have sought to increase COVID-19 testing capacity (though some have inadequate access to testing supplies), and to isolate confirmed and presumptive infected persons and trace their contacts. Many have improved their capacities in these areas since the start of the pandemic (see next section), in some cases building on lessons from past Ebola virus outbreak responses.221 Many African health systems, however, have limited capacities. Per capita ratios of doctors and health workers, rates of health spending, and hospital beds are some of the lowest globally, and supplies of healthcare goods (e.g., drugs, ventilators, and oxygen supplies) are low.222 Socioeconomic challenges also hinder prevention measures centering on hygiene (e.g., handwashing) and social distancing. Many Africans lack access to clean water or sanitation facilities, and live in high-density areas (e.g., informal urban settlements or displaced person camps). COVID-19 co-morbidity with other diseases widespread in the region (e.g., HIV and malaria) and/or chronic health problems (e.g., diabetes and malnutrition) may increase the risk from COVID-19 in Africa.
Most countries have launched public outreach campaigns centered on personal hygiene promotion, the use of facial masks, and social or physical distancing. Residential lockdowns, business restrictions, prohibitions on large gatherings, and school and university closures have been common. Some countries, however, have implemented only some of these various responses, or implemented them in limited geographic areas.223 Governments in multiple countries have authorized restrictive measures under pandemic national states of disaster or emergency. In several countries, security forces enforcing lockdowns and other restrictions have violated human rights, at times in the face of social unrest over the effects of these restrictive measures. In some countries, observers fear that incumbent regimes may use their emergency authorities to extend their powers or time in office, or, as some have, to restrict press freedoms or opposition activity.224
Given that many Africans make a precarious hand-to-mouth living in the informal sector, lockdowns have caused intense economic pain in the region, and governments have been eager to permit normal commercial activity to resume. A number of African governments began easing restrictive measures in late April, though in some countries, a spike in COVID-19 cases has accompanied or followed such actions.225
Experts are concerned that the pandemic's broader economic impacts could be particularly devastating in Africa, where many countries rely on tourism and/or commodity exports, notably to China.226 Both tourism and exports have declined sharply due to COVID-19-linked interruptions and declines in world economic activity, trade, and travel. In food import-dependent countries, food insecurity may also increase, due to these factors as well as lock-down linked restrictions. Remittances from abroad also have dropped. Africa's heavy reliance on imports of consumer and industrial goods from China may also suffer, alongside business sectors tied to these imports (e.g., digital technology and local retail sectors).227 Exports of mined and energy commodities, which comprise roughly 75% of African exports by value, may be particularly hard-hit. Africa's oil export-dependent countries may face a double threat: a global oil price collapse initially driven by a now-ended price war among selected producers and an ongoing collapse in global oil demand.228 African airlines also are suffering steep losses. Multiple central banks have acted to increase economy-wide liquidity and many governments are making resource reallocations or are slated to receive international assistance to finance COVID-19 responses.229
How is the Africa CDC responding?
The African Union (AU) Africa Centres for Disease Control and Prevention (Africa CDC), at times in partnership with the WHO and other international actors, is helping African governments to enhance the capacity of their public health systems to detect and respond to COVID-19.230 Africa CDC support has centered on training personnel on disease detection and surveillance at national laboratories and ports of entry, providing COVID-19 test kits and other health commodities (e.g., personal protection equipment or PPE), and other health response capacity-building.231 The Africa CDC has provided COVID-19 detection training to at least 40 country labs, almost all of which are now able to independently test for the disease. These labs are supported by a regional COVID-19 specimen referral and verification system comprising expert labs in Senegal and South Africa, with ten more planned region-wide.232 The Africa CDC also has created a regional COVID-19 task force under a regional response plan, has activated its Emergency Operations Center and Incident Management System, and is aiding information sharing among AU member states.233 The Africa CDC also has trained epidemiologists in disease event tracking and risk analysis, including through its Regional Collaborating Centres (RCCs), and is providing COVID-19 medical and technical advice and pandemic briefings to AU member states.234
Middle East and North Africa235
How are Middle Eastern and North African governments responding?
As of May 2020, all 17 countries in the Middle East and North Africa region, in addition to the Palestinian territories, had confirmed local transmission of COVID-19.236 Iran was an early epicenter of the pandemic; as of May, Iranian cases represent roughly 40% of all confirmed cases in the region. The six Arab Gulf states also have emerged as a focal point; as of May these states (combined) also represent nearly 40% of the region's confirmed cases.237 Observers and U.S. government officials have expressed concern that some states have sought to downplay the extent of the spread of the virus in their countries.238 Many countries in the region also lack the capability to conduct comprehensive testing.
Starting in March, many countries suspended international and domestic passenger flights, closed land and sea crossings with neighboring states, imposed curfews, and closed commercial, educational, and religious sites. Some governments also passed emergency legislation and expanded surveillance as part of their response to the pandemic. In some cases, observers argued that these measures may have been designed in part to suppress political opposition.239
- In Egypt, parliament expanded the country's emergency law; Human Rights Watch warned that most of the new authorities granted to the government are unrelated to public health issues.240
- In Algeria, the government of recently elected President Abdelmadjid Tebboune banned all public gatherings of more than two people, including protest rallies, which had been held weekly for political reforms since February 2019.241
- In Israel, the government approved temporary emergency regulations for security officials to monitor COVID-19 patients and potential victims via their mobile phones.
Economies in the region have been hard hit by the collapse in global energy prices and tourism. As in other regions, government efforts to contain the spread of the virus have also involved the suspension of most public commerce and trade, resulting in a severe blow to economic activity that is expected to generate increased unemployment. In April, the IMF projected that the region comprising the Middle East, North Africa, Afghanistan, and Pakistan would contract by 3.1% in 2020, with oil exporters in the region contracting by 4.2%.242 Rising unemployment, particularly concentrated among the youth, could have implications for political stability in the region. A prolonged global economic slowdown associated with COVID-19 also could dampen global demand for oil and natural gas resources exported from countries in the Middle East and North Africa for a prolonged period, with corresponding diminishing effects on export revenues and the fiscal health of some regional governments.
Starting in late April, some countries began lifting some internal restrictions on movement and commercial activity—including Tunisia, where nationwide lockdown measures appeared to contribute to a drop in new confirmed cases—and Lebanon, where cases appeared to spike following the easing of restrictions.243 The WHO Eastern Mediterranean Regional (EMR) office warned, "Without careful planning, and in the absence of scaled up public health and clinical care capacities, [a] premature lifting of physical distancing measures is likely to lead to an uncontrolled resurgence in COVID‑19 transmission and an amplified second wave of cases."244
The WHO has highlighted the particular risks posed by the spread of the virus to states such as Syria, Libya, and Yemen, noting that years of conflict, natural disasters, and previous outbreaks
have left these countries with weakened health systems, shortages in health workers, and limited access to even the most basic medical care services. Millions of already vulnerable people in these countries are also more prone to infectious diseases due to overcrowded living conditions, weakened immunity due to years of food insecurity, and insufficient treatment for other underlying medical conditions. Many of these countries are also politically fragmented, resulting in limited humanitarian access to populations in some areas, and challenges in the sharing of information between controlling parties and WHO in a timely and transparent manner.245
In addition, other areas of elevated risk in the region include the following:
- The Gaza Strip. The Hamas-controlled Gaza Strip has reported 20 COVID-19 cases as of May 11, and officials from international organizations have voiced concerns about a possible outbreak given the acute humanitarian challenges in Gaza. The densely populated territory of nearly 2 million Palestinians has a weak health infrastructure and many other challenges related to sanitation and hygiene.246 On May 8, the U.N. Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) updated an emergency flash appeal from $14 million to $93.4 million to prepare and respond to COVID-19-related needs for Palestinian refugees in Gaza, the West Bank, Jordan, Lebanon, and Syria through July 2020. The Trump Administration stopped U.S. contributions to UNRWA in 2018 and all bilateral aid to the West Bank and Gaza in 2019.247 For FY2020, Congress appropriated $75 million from the Economic Support Fund for humanitarian and development purposes in the West Bank and Gaza, and some Members of Congress have called for the Administration to obligate some of this assistance for Gaza.248
- The Hajj (Saudi Arabia). Each year, millions of Muslims travel to Saudi Arabia for a religious pilgrimage to Mecca. This journey, known as the Hajj, is a pillar of the Islamic faith. Saudi authorities have invested considerable attention and resources to averting infectious disease outbreaks during the Hajj, having faced 2009 H1N1 Pandemic, SARS, and MERS. In February 2020, Saudi leaders suspended umrah pilgrimage visits to the kingdom (which can be done at any time of year in contrast to the Hajj) and limited access to holy sites in Mecca and Medina. In late March, Saudi officials asked Muslims to delay making Hajj travel plans until the effects of the pandemic were clearer. It remains to be seen whether the Hajj pilgrimage will go forward as scheduled in July and August 2020.
- U.S. Military Facilities. The United States maintains a significant military presence in the region, and has partnered closely with local forces. U.S. forces remain in Iraq and are consolidating base locations. U.S. training of Iraqi military personnel has been suspended due to COVID-19 risks, and U.S. officials stated in late March that future training would use "fewer bases with fewer people."249
What are the implications for U.S.-Iran policy?
The spread of COVID-19 in Iran has raised questions about the possible effects of U.S. sanctions on Iran's response capacity.250 The Trump Administration's policy of "maximum pressure" on Iran imposes economic sanctions on every sector of Iran's economy. Iranian officials and some global health officials assert that the U.S. sanctions are weakening Iran's ability to contain the virus by reducing the availability of medical equipment.251 Sales to Iran of humanitarian items, including medicine and medical equipment, are generally exempt from U.S. sanctions. The reluctance of banks worldwide, however, to finance any transactions involving Iran, fearing penalties by the United States for sanctions violations, has reportedly affected Iran's ability to import all types of goods, including those that are exempt from sanctions. As the disease spread in Iran in February 2020, the United States has offered Iran an unspecified amount of assistance to help it deal with the outbreak, but Iran's government has refused the aid. In early March 2020, U.S. officials issued guidance indicating that transactions involving Iran's foreign exchange assets held abroad, when used to buy humanitarian items, would not face U.S. sanctions.252 However, the Administration opposes Iran's request for a $5 billion loan from the International Monetary Fund (IMF) that Iran says it needs to cope with the COVID-19 crisis; the Administration asserts that Iran has ample amounts of funds for medical imports and would use the loan proceeds to support pro-Iranian armed factions in various countries.253 Under the IMF's voting rules, the U.S. voting power is not sufficient to unilaterally veto specific IMF program requests, even though the United States has the largest share at the IMF and can veto major policy decisions at the IMF.254 Although over the past two decades Congress has supported increased sanctions on Iran, some Members of Congress have called on the Administration to relax sanctions on Iran, at least temporarily, to help Iran deal with the COVID-19 pandemic and thereby help curb the disease's broader spread.255
Canada, Latin America, and the Caribbean256
How is the Canadian government responding?
Canada's federal, provincial, and territorial governments have worked closely together to manage the country's response to the COVID-19 pandemic. While the federal government has provided broad public health guidelines intended to slow the spread of the virus, provincial and territorial governments have implemented varying measures in accordance with local conditions. As of early May 2020, all of the provinces had developed phased reopening plans, and some had begun loosening restrictions on certain business, education, and recreational activities while maintaining physical distancing guidelines.
The federal, provincial, and territorial governments also have cooperated on efforts to secure personal protective equipment, testing materials, and other medical supplies. Nevertheless, provincial health services, which administer the Canadian health system, reportedly have experienced some shortages. Prime Minister Justin Trudeau has acknowledged that Canada's National Emergency Strategic Stockpile did not have sufficient supplies prior to the pandemic, but federal officials maintain that they have been able to fulfill every request for personal protective equipment received from the provinces.257
Prime Minister Trudeau has worked with the Canadian Parliament to enact a series of measures intended to mitigate the economic impact of the pandemic. As of late April 2020, their announced assistance measures amounted to an estimated C$146 billion ($104 billion)—equivalent to about 7% of Canada's projected gross domestic product (GDP) for 2020.258 These include a new Canada Emergency Response Benefit that provides C$2,000 ($1,424) every 4 weeks for up to 16 weeks for workers who have lost their incomes due to COVID-19, and a new Canada Emergency Wage Subsidy that covers 75% of employees' wages, up to C$847 ($603) per week, for up to 12 weeks.259 Prime Minister Trudeau has signaled his intention to extend such programs as necessary. To provide additional support to the economy and financial system, the Bank of Canada cut its benchmark interest rate from 1.75% to 0.25%, and launched its first-ever quantitative easing program to purchase government and commercial debt.260 Canada's Parliamentary Budget Officer forecasts that the country's real GDP will contract by 12% in 2020, but expects an economic recovery to begin in the second half of the year.261
The Canadian and U.S. governments have coordinated decisions concerning their shared border. On March 21, they closed the border to all nonessential travel. Although the closure initially was to last 30 days, both governments agreed to extend it until May 21. The Canadian government reportedly has requested that the closure remain in place until June 21; several provincial governments are opposed to a quick reopening of the border given the scope of the COVID-19 outbreak in the United States.262 The Canadian and U.S. governments generally have prioritized keeping the border open to trade. In April 2020, however, the Trump Administration invoked the Defense Production Act of 1950 (50 U.S.C. §§4501 et seq.) to restrict certain medical exports. Prime Minister Trudeau urged the United States not to interrupt the flow of essential goods and services, and the Administration ultimately exempted Canada from the export restrictions.263
How are Latin American and Caribbean governments responding?
The ability of countries in Latin America and the Caribbean to mitigate a COVID-19 outbreak varies across the region, and responses have been diverse. The pandemic appears to have arrived in Latin American and the Caribbean later than many other regions and has yet to peak. A 2019 Global Health Security Index included Brazil, Argentina, Chile, and Mexico among countries most prepared for a pandemic, and considered Venezuela, Honduras, Jamaica, the Bahamas, Haiti, Guyana, Belize, and Guatemala to be among the least prepared.264 Although all countries in the region aspire to universal health coverage, many lack sufficient doctors, hospitals, medical supplies and other critical infrastructure, and face challenges of inequality and economic fragility as they grapple with the pandemic.265
The patchwork of response efforts across 33 countries, including a cautious lifting of control measures in some countries in May 2020, has relied on incomplete data to guide policy since most countries have not conducted widespread testing. In Mexico, Brazil, and Nicaragua, where presidents have downplayed the threat of the pandemic, many analysts suggest the actual level of infection is essentially unknown, with some independent estimates suggesting it is a magnitude higher than what health authorities have reported.266 The information available suggests some countries are suffering severe outbreaks, while others, such as Paraguay, appear to have relatively few cases.267
According to several observers, the region's vulnerability is heightened by diminished health spending and low government capacity, following several years of economic stagnation. Venezuela is of particular concern since protracted political and economic crises had already weakened its health system. An estimated 4.8 million Venezuelans have fled the country, and new immigration controls by neighboring countries are unlikely to stop Venezuelans from crossing the region's porous borders.
As the most urbanized region in the world, Latin American and the Caribbean nations face challenges enforcing social distancing by quarantine and curfew.268 In some cities, such as Guayaquil, Ecuador, outbreaks have already overwhelmed medical systems.269 In rural areas, and urban slums, there is limited access to clean water and sewage treatment and minimal health infrastructure. Indigenous communities, Afro-descendants, migrants, refugees, and internally displaced persons often face formidable barriers to health care. Quarantine restrictions in some cases have created a dangerous rise in hunger and desperation since a large proportion of the population depends on daily earnings, often through informal employment, to make ends meet.270
Many governments have taken extraordinary measures to respond to the pandemic. Some have been accused of abuses of power and violations of human rights for arresting and imprisoning quarantine violators, harshly treating prison uprisings and jailed gang members (notably in El Salvador),271 and delaying elections.272 Many governments also have begun to implement far-reaching economic support measures, although their fiscal capacities to support businesses and bolster social safety nets varies considerably. The IMF estimates the region's economic growth will contract this year by 5.2%.273
International Economic and Supply Chain Issues274
What are the implications of the pandemic in China's economy?
COVID-19 emerged amidst an economic downturn in China with officials navigating U.S.-China bilateral tariffs, working to curb consumer inflation (due in part to domestic pork shortages resulting from African swine fever), and moving to rein in government spending and shadow lending. COVID-19 containment measures significantly slowed economic activity in China, and halted production almost entirely in some areas of the country, particularly Hubei province.275 In early February, China's central bank pumped $57 billion into the banking system, capped banks' interest rates on loans for major firms, and extended deadlines for banks to curb shadow lending. China's central bank is seeking to stabilize China's currency and shore up liquidity in China's banking system, which remains the primary channel through which the government is providing business relief. 276 Despite these measures, China experienced a 6.8% contraction in GDP growth in the first quarter of 2020, the first GDP contraction recorded in China since China's National Bureau of Statistics began releasing quarterly GDP figures in 1992.277
Many firms in China are still struggling to return to full capacity as some restrictions on travel and distribution of goods and workers remain and additional reported pockets of outbreaks continue in different parts of China.278 In addition, COVID-19's global spread has led to a sharp global economic downturn and reduced global demand for Chinese exports. China's recovery is also constrained by a contraction in global transportation and logistics and tourism and services trade.
The economic impact of COVID-19 has also raised questions about the capacity of the United States and China to implement the Phase One Trade Agreement signed in January 2020, which commits China to purchasing $200 billion in additional exports over the next two years.279 Recent analysis of both U.S. and Chinese first quarter trade data indicates that China is not on track to meet its purchase commitments—according to U.S. trade data, China's imports of agricultural products, a major component of the purchase agreements, grew by a modest 3.2%, while China's imports of U.S. manufactured goods and energy shrank.280 Reports in China's state media have suggested that some elements of China's leadership might be considering invalidating and renegotiating the phase one agreement.281
How is COVID-19 affecting the global economy and financial markets?
A growing list of economic indicators makes it clear that the viral outbreak is negatively affecting global economic growth on a scale that has not been experienced since at least the global financial crisis of 2008-2009.282 Global trade and GDP are forecast to decline sharply through at least the first half of 2020. The global pandemic is affecting a broad swath of international economic and trade activities, from services generally to tourism and medical supplies, global value chains, financial markets, and a range of social activities, to name a few. The health and economic crises could have a particularly negative impact on developing economies that are constrained by limited financial resources and where health systems could quickly become overloaded.
The economic situation remains highly fluid. Labeling the projected decline in global economic activity as the Great Lockdown, the IMF forecasted on April 14, 2020 that the global economy could decline by 3.0% in 2020, before growing by 5.8% in 2021, constituting the "worst recession since the Great Depression, surpassing that seen during the global financial crisis a decade ago."283 Estimates by the Organization for Economic Cooperation and Development (OECD) indicate the virus could trim global economic growth by as much as 2.0% per month if current conditions persist, or 24% on an annual basis. Global trade could also fall by 13% to 32%, depending on the depth and extent of the global economic downturn. Increasing rates of unemployment are raising the prospects of wide-spread social unrest and demonstrations in developed economies where lost incomes and health insurance are threatening living standards and in developing economies where populations reportedly are growing concerned over access to basic necessities and the prospects of rising levels of poverty.
Over the seven-week period from mid-March to early May 2020, more than 33 million Americans filed for unemployment insurance. On May 8, 2020, the Bureau of Labor Statistics (BLS) reported that 20 million Americans lost their jobs in April 2020, pushing the total number of unemployed Americans to 23 million and raising the unemployment rate to 14.7%, the highest since the Great Depression of the 1930s. The report indicated that all major industry sectors experienced job losses, with the heaviest losses in the leisure and hospitality industries. Preliminary data indicate that U.S. GDP in the first quarter 2020 fell by 4.8% at an annual rate, the largest quarterly decline in GDP since the fourth quarter of 2008 during the global financial crisis. The U.S. economy is projected to contract by 5.9%, about twice the rate of decline experienced in 2009 during the financial crisis. The forecast assumes that the pandemic fades in the second half of 2020 and that the containment measures can be reversed.
The IMF also argues that recovery of the global economy could be weaker than projected as a result of lingering uncertainty about possible contagion, lack of investor and consumer confidence, and permanent closure of businesses and shifts in the behavior of firms and households.284 Global trade, measured by trade volumes, slowed in the last quarter of 2019 and was expected to decline further in 2020, as a result of weaker global economic activity associated with the pandemic.
Uncertainty about the length and depth of pandemic-related economic effects and the effectiveness of pandemic control measures are shaping perceptions of risk and volatility in financial markets and corporations. Financial markets worldwide, particularly in the United States, Asia, and Europe, are volatile as investors are concerned that the virus is creating a global crisis that could be prolonged and expansive.285 Similar to the 2008-2009 global financial crisis, central banks are rapidly becoming the lender of last resort and are attempting to address financial market volatility. Developments continue to evolve rapidly and the market dynamics have led some observers to question if these events mark the beginning of a full-scale global financial crisis.286
Financial market dislocation can potentially increase liquidity constraints and credit market tightening, as firms hoard cash, with negative effects on economic growth. In some financial markets, fund managers have started selling government securities to increase their cash reserves, pushing down government bond prices. Financial markets are also responding to increased government bond issuances in the United States and Europe to fund COVID-19-related spending, further increasing government debt.
How is COVID-19 affecting U.S. medical supply chains? 287
COVID-19 has revealed U.S. and global supply chain vulnerabilities across a range of sectors, particularly PPE, which relies directly on China-based manufacturing. During the 2002-2003 SARS outbreak, China accounted for 8% of global manufacturing exports; in 2018, China was the source of approximately 19% of global manufacturing exports, including intermediate goods vital to global manufacturing supply chains.288
An area of particular concern to Congress in the current environment is U.S. shortages of medical supplies—including personal protective equipment (PPE) and pharmaceuticals—as the United States steps up efforts to contain COVID-19 with limited domestic stockpiles and insufficient U.S. industrial capacity. Because of China's role as a global supplier of PPE, medical devices, antibiotics, and active pharmaceutical ingredients (API), reduced exports from China have led to shortages of critical medical supplies in the United States.289 According to China Customs data, in 2019 China exported $9.8 billion in medical supplies and $7.4 billion in organic chemicals—a figure that includes active pharmaceutical ingredients and antibiotics—to the United States. While there are no internationally agreed guidelines and standards for classifying these products, U.S. imports of pharmaceuticals, medical equipment and products, and related supplies are estimated to have been approximately $20.7 billion (or 9.2% of U.S. imports), according to CRS calculations using official U.S. data.290
In early February 2020, the Chinese government nationalized control of the production and distribution of medical supplies in China, directing all production for domestic use.291 The Chinese government also directed the national bureaucracy, local governments, and Chinese industry to secure supplies from the global market.292 This effort likely exacerbated medical supply shortages in the United States and other countries, particularly in the absence of domestic emergency measures that might have locked in domestic contracts, facilitated an earlier start to alternative points of production, and restricted exports of key medical supplies. In addition to formal and informal PPE export restrictions that China reportedly has placed on domestic producers of PPE, several prominent U.S. companies with PPE production capacity located in China, including 3M, have indicated they do not have PRC government authorization to export.293As China's manufacturing sector recovers while the United States and other countries are grappling with COVID-19, the Chinese government may selectively release some medical supplies for overseas delivery. Those decisions are likely to be driven, at least in part, by political calculations, as has been the case with many countries around the world.294
Issues for Congress295
The COVID-19 pandemic has raised questions about domestic and international preparedness and the appropriate responses to pandemic control. Although the United States has long-supported the delivery of PPE through its international pandemic preparedness programs, this practice has come into question while the numbers of COVID-19 cases and deaths climb in the United States. As of April 15, 2020, the United States had the highest number of COVID-19 cases and deaths worldwide, accounting for roughly 30% of all COVID-19 cases globally. In March, some Members of Congress began questioning the delivery of PPE by USAID to foreign countries while some governors and mayors reported shortages of the commodities.296
The United States provides annual funding for foreign assistance, approximately $20 billion of which is administered by USAID each year. USAID programs operate in more than 120 countries worldwide and are intended to meet specific development objectives. In many of these countries, widespread poverty, weak public institutions, and diverse pre-existing governance challenges are likely to be exacerbated by the pandemic. To preserve these investments and past policy progress, protect U.S. foreign policy interests in the region, save lives, and help combat the negative socioeconomic effects of the pandemic in the region, Congress may seek to address additional help aid recipients might request to control the pandemic and its effects.
Congress might also consider how the pandemic may affect partner governments' absorption capacities, and the manner and degree to which U.S. assistance may complement or coincide with nationally-determined pandemic responses. Congress may also wish to consider how responding to the challenges created by the pandemic may reshape pre-existing U.S. aid priorities—and how it may affect the ability of U.S. personnel to implement and oversee programs in the field. Relatedly, Congress may wish to ensure that U.S. responses are robustly coordinated with those of other donor governments and multilateral functional agencies—and to ensure that such efforts are transparent and cost-effective, and that donor assistance is complementary and non-duplicative.
The pandemic is also having other effects on foreign affairs that Congress might consider. Some have questioned, for example, how U.S. immigration policy might impact COVID-pandemic control efforts. Some Members of Congress and officials representing Latin American and Caribbean governments have expressed concern that COVID-19-related screening procedures for deportations are not sufficient to prevent the importation of COVID-19 cases from the United States and have asked the U.S. Immigration and Customs Enforcement (ICE) to suspend deportations.297 A number of people deported from the United States to Latin America have reportedly tested positive with COVID-19 or have reportedly been exposed to someone with COVID-19. Other Members of Congress continue to support the Administration's border policies, which the Administration maintains are conducted in a manner that accounts for the dangers of COVID-19.298
Congress continues to debate the extent to which the United States should contribute to multilateral organizations for COVID-19 control. Some Members, for example, are arguing for withholding contributions to the WHO, while others are urging the Administration to pay outstanding assessments to the organization and support ongoing WHO COVID-19 efforts.299
Appendix. Supplemental Information
Selected Legislation Introduced or Enacted in the 116th Congress Related to International COVID-19 Incidence or International Pandemic Preparedness300
H.Res. 962, Expressing support for assisting East African countries afflicted by the plague of desert locusts. Referred to the House Committee on Foreign Affairs on May 8, 2020.
S. 3669, A bill to respond to the global COVID-19 pandemic, and for other purposes. Referred to the Senate Committee on Foreign Relations on May 7, 2020.
S.Res. 567, A resolution commending career professionals at the Department of State for their extensive efforts to repatriate United States citizens and legal permanent residents during the COVID-19 pandemic. Referred to the Senate Committee on Foreign Relations on May 7, 2020.
S. 3600, Li Wenliang Global Public Health Accountability Act of 2020. Referred to the Senate Committee on Foreign Relations on May 5, 2020.
S. 3598, Repatriation Reimbursement Act. Referred to the Senate Committee on Commerce, Science, and Transportation on May 4, 2020.
S. 3592, Stop COVID Act of 2020. Referred to the Senate Committee on the Judiciary on May 4, 2020.
S. 3588, Justice for Victims of Coronavirus Act. Referred to the Senate Committee on Foreign Relations on May 4, 2020.
S.Res. 556, A resolution designating May 1, 2020, as the "United States Foreign Service Day" in recognition of the men and women who have served, or are presently serving, in the Foreign Service of the United States, and honoring the members of the Foreign Service who have given their lives in the line of duty. Referred to the Senate Committee on the Judiciary on May 4, 2020.
H.R. 6657, WUHAN Rescissions Act. Referred to the House Committee on Appropriations on May 1, 2020.
H.R. 6665, To direct the Secretary of State, in consultation with the Secretary of Health and Human Services, to submit a report on the actions of the World Health Organization to address the spread of the virus responsible for COVID-19, and for other purposes. Referred to the House Committee on Foreign Affairs on May 1, 2020.
H.Res. 944, Expressing the sense of the House of Representatives that the People's Republic of China should be held accountable for its handling of COVID-19. Referred to the House Committee on Foreign Affairs on April 28, 2020.
H.R. 6610, Director of Pandemic and Biodefense Preparedness and Response Act. Referred to the House Committee on Energy and Commerce, and in addition to the House Committees on Transportation and Infrastructure, Armed Services, Foreign Affairs, and Intelligence (Permanent Select), for a period to be subsequently determined by the Speaker, in each case for consideration of such provisions as fall within the jurisdiction of the committee concerned on April 23, 2020. Referred to the Subcommittee on Economic Development, Public Buildings, and Emergency Management by the Committee on Transportation and Infrastructure on April 24, 2020.
H.R. 6599, COVID Research Act of 2020. Referred to the Committee on Energy and Commerce, and in addition to the Committee on Science, Space, and Technology, for a period to be subsequently determined by the Speaker, in each case for consideration of such provisions as fall within the jurisdiction of the committee concerned on April 23, 2020.
H.R. 6598, SOS ACT Act. Referred to the Committee on Financial Services, and in addition to the Committee on Foreign Affairs, for a period to be subsequently determined by the Speaker, in each case for consideration of such provisions as fall within the jurisdiction of the committee concerned on April 23, 2020.
H.Res. 940, Recognizing the commencement of Ramadan, the Muslim holy month of fasting and spiritual renewal, and commending Muslims in the United States and throughout the world for their faith. Referred to the House Committee on Foreign Affairs on April 23, 2020.
H.Res. 939, Supporting the World Bank Group to lead a worldwide COVID-19 economic recovery effort. Referred to the House Committee on Financial Service on April 23, 2020.
H.R. 6595, Expanding Vital American Citizen Services Overseas (EVACS) Act of 2020. Referred to the House Committee on Foreign Affairs on April 22, 2020.
H.R. 6541, PPE Act of 2020. Referred to the Committee on Energy and Commerce, and in addition to the Committee on Financial Services, for a period to be subsequently determined by the Speaker, in each case for consideration of such provisions as fall within the jurisdiction of the committee concerned on April 17, 2020.
H.R. 6531, Medical Supplies for Pandemics Act of 2020. Referred to the House Committee on Energy and Commerce on April 17, 2020.
H.R. 6524, Compensation for the Victims of State Misrepresentations to the World Health Organization Act of 2020. Referred to the House Committee on the Judiciary on April 17, 2020.
H.R. 6522, PPP Expansion Act of 2020. Referred to the House Committee on Small Business on April 17, 2020.
H.R. 6519, Holding the Chinese Communist Party Accountable for Infecting Americans Act of 2020. Referred to the House Committee on the Judiciary on April 17, 2020.
H.Con.Res. 97, Establishing the Joint Select Committee on the Events and Activities Surrounding China's Handling of the 2019 Novel Coronavirus. Referred to the House Committee on Rules on April 17, 2020.
H.R. 6504, To direct the Secretary of Health and Human Services, acting through the Director of the Centers for Disease Control and Prevention, to develop a plan to improve surveillance with respect to diseases that are viral pandemic threats, and for other purposes. Referred to the House Committee on Energy and Commerce on April 14, 2020.
H.Res. 922, Expressing the sense of the House of Representatives that all nations should permanently close live wildlife markets and that the People's Republic of China should cease spreading disinformation regarding the origins of coronavirus. Referred to the House Committee on Foreign Affairs, and in addition to the House Committees on Natural Resources, Agriculture, and Energy and Commerce on April 14, 2020.
H.R. 6500, To reduce Federal spending and fund the acquisition of unexpired personal protective equipment (including face masks) for the strategic national stockpile by terminating taxpayer financing of Presidential election campaigns. Referred to the House Committee on Ways and Means, and in addition to the Committee on House Administration, on April 14, 2020.
H.R. 6481, To rescind the appropriation made for migration and refugee assistance in the Coronavirus Aid, Relief, and Economic Security Act and redirect the funds to U.S. Customs and Border Protection and U.S. Immigration and Customs Enforcement. Referred to the House Committee on Appropriations on April 10, 2020.
H.R. 6480, To require the President, after the World Health Organization declares a global pandemic, to report to the Congress on the status of Federal planning to respond to the pandemic. Referred to the House Committee on Energy and Commerce, and in addition to the Committee on Financial Services on April 10, 2020.
H.Res. 919, Condemning the United Nations' decision to appoint China a seat on its Human Rights Council. Referred to the House Committee on Foreign Affairs on April 10, 2020.
H.R. 2166, Global Health Security Act of 2019. Directs the President to create the Global Health Security Agenda Interagency Review Council to implement the Global Health Security Agenda, an initiative launched by nearly 30 nations to address global infectious disease threats. Ordered to be reported on March 4, 2020, and introduced in the House on April 9, 2020.
H.Res. 917, Expressing the sense of the House of Representatives that the United States should withhold the contribution of Federal funds to the World Health Organization until Director-General Tedros Ghebreyesus resigns and an international commission to investigate the World Health Organization is established. Referred to the House Committee on Foreign Affairs on April 7, 2020.
H.R. 6471, To posthumously award a Congressional Gold Medal to Dr. Li Wenliang, in recognition of his efforts to save lives by drawing awareness to COVID-19 and his call for transparency in China. Referred to the House Committee on Financial Services, and in addition to the Committee on House Administration on April 7, 2020.
H.R. 6429, To establish in the Legislative Branch a National Commission on the Coronavirus Disease 2019 Pandemic in the United States. Referred to the House Subcommittee on Economic Development, Public Buildings, and Emergency Management on April 6, 2020.
H.R. 6440, To establish the National Commission on the COVID-19 Pandemic. Referred to the House Committee on Energy and Commerce on April 3, 2020.
P.L. 116-136, Coronavirus Aid, Relief, and Economic Security Act or the CARES Act. Enacted H.R. 748 on March 27, 2020.
H.R. 6410, To direct the President to use authority under the Defense Production Act of 1950 to ensure an adequate supply of equipment necessary for limiting the spread of COVID-19. Referred to the House Committee on Financial Services on March 27, 2020.
H.R. 6398, To provide for the expedited procurement of equipment needed to combat COVID-19 under the Defense Production Act of 1950. Referred to the House Subcommittee on Economic Development, Public Buildings, and Emergency Management on March 27, 2020.
H.R. 6406, To require personal protective equipment to be included in the strategic national stockpile, and to require the Federal Government to procure such equipment from United States sources, and for other purposes. Referred to the Subcommittee on Economic Development, Public Buildings, and Emergency Management on March 27, 2020.
H.R. 6405, To direct the President, in consultation with the Secretary of the Treasury, to develop and carry out a strategy to seek reimbursement from the People's Republic of China of funds made available by the United States Government to address the Coronavirus Disease 2019 (COVID-19). Referred to the House Committee on Foreign Affairs on March 26, 2020.
S. 3586, Eliminating Leftover Expenses for Campaigns from Taxpayers (ELECT) Act of 2020. Referred to the Senate Committee on Finance on March 25, 2020.
H.R. 6390, To require the President to use authorities under the Defense Production Act of 1950 to require emergency production of medical equipment to address the COVID-19 outbreak. Referred to the House Committee on Financial Services on March 25, 2020.
H.R. 6393, To require the Secretary of Defense to submit to Congress a report on the reliance by the Department of Defense on imports of certain pharmaceutical products made in part or in whole in certain countries, to establish postmarket reporting requirements for pharmaceuticals, and for other purposes. Referred to the House Committee on Ways and Means, and in addition to the House Committees on Armed Services, Oversight and Reform, and Energy and Commerce on March 25, 2020. As of April 15, 2020, no text of the bill was available.
S.Res. 552, A resolution supporting an international investigation into the handling by the Government of the People's Republic of China of COVID-19 and the impact of handling COVID-19 in that manner on the people of the United States and other nations. Referred to the Senate Committee on Foreign Relations on March 24, 2020.
H.Res. 907 and S.Res. 553, Expressing the sense of the House of Representatives that the Government of the People's Republic of China made multiple, serious mistakes in the early stages of the COVID-19 outbreak that heightened the severity and spread of the ongoing COVID-19 pandemic, which include the Chinese Government's intentional spread of misinformation to downplay the risks of the virus, a refusal to cooperate with international health authorities, internal censorship of doctors and journalists, and malicious disregard for the health of ethnic minorities. Referred to the House Committee on Foreign Affairs on March 24, 2020.
S. 3573, American-Made Protection for Healthcare Workers and First Responders Act. Referred to the Senate Committee on Health, Education, Labor, and Pensions on March 24, 2020.
S. 3570, A bill to provide for the expedited procurement of equipment needed to combat COVID-19 under the Defense Production Act of 1950. Referred to the Senate Committee on Banking, Housing, and Urban Affairs on March 23, 2020.
S. 3568, Medical Supply Chain Emergency Act of 2020. Referred to the Senate Committee on Banking, Housing, and Urban Affairs on March 23, 2020.
H.R. 6379, Take Responsibility for Workers and Families Act, Referred to the House Committee on Appropriations, and in addition to the House Committees on the Budget, and Ways and Means on March 23, 2020.
H.R. 6373, To increase the amount available under the Defense Production Act of 1950 to respond to the coronavirus epidemic, and for other purposes. Referred to the House Committee on Financial Services on March 23, 2020.
H.R. 6371, To amend the Securities Exchange Act of 1934 to require issuers to disclose risks related to global pandemics, and for other purposes. Referred to the House Committee on Financial Services on March 23, 2020.
H.R. 6319, To establish a Congressional COVID-19 Aid Oversight Panel, to authorize the Special Inspector General for the Troubled Asset Relief Program to coordinate audits and investigations in connection with the receipt of Federal aid related to COVID-19, and for other purposes. Referred to the House Committee on Financial Services on March 23, 2020.
H.Res. 906, Calling on the President to invoke the Defense Production Act to respond to COVID-19. Referred to the House Committee on Financial Services on March 23, 2020.
S. 3548, Coronavirus Aid, Relief, and Economic Security Act or the CARES Act. Referred to the Senate Committee on Finance on March 21, 2020.
H.R. 6310, To require the Secretary of Defense to make testing for the coronavirus disease 19 available to all members of the Armed Forces deployed to an area in which the United States Central Command has responsibility. Referred to the House Committee on Armed Services, March 19, 2020.
H.R. 6482, A bill to require the Secretary of Health and Human Services to maintain a list of the country of origin of all drugs marketed in the United States, to ban the use of Federal funds for the purchase of drugs manufactured in China, and for other purposes. Referred to the Senate Committee on Finance on March 19, 2020.
S. 3538, Strengthening America's Supply Chain and National Security Act. Referred to the Senate Committee on Finance, March 19, 2020.
S. 3537, Protecting Our Pharmaceutical Supply Chain from China Act of 2020. Referred to the Senate Committee on Finance, March 19, 2020.
S.Res. 547, A resolution encouraging the President to use authorities provided by the Defense Production Act of 1950 to scale up the national response to the coronavirus crisis. Referred to the Senate Committee on Banking, Housing, and Urban Affairs, March 18, 2020.
S. 3530, A bill to amend the National Security Act of 1947 to require the President to designate an employee of the National Security Council to be responsible for pandemic prevention and response, and for other purposes. Referred to the Senate Committee on Homeland Security and Governmental Affairs on March 18, 2020.
S. 3507, A bill to require the Secretary of Defense to make testing for the coronavirus disease 19 available to all members of the Armed Forces deployed to an area in which the United States Central Command has responsibility. Referred to the Senate Committee on Armed Services on March 17, 2020.
S. 3510, A bill to transfer all border wall funding to the Department of Health and Human Services and USAID to combat coronavirus. Referred to the Committee on Homeland Security and Government Affairs on March 17, 2020.
H.R. 6288, Responsibly Responding to Pandemics Act. Referred to the House Subcommittee on Economic Development, Public Buildings, and Emergency Management, March 16, 2016.
H.R. 6205, Assistance for Workers Harmed by COVID-19 Act. Amends the Trade Act of 1974 to provide adjustment assistance to certain workers adversely affected by disruptions in global supply chains from COVID–19, and for other purposes. Referred to the House Committee on Ways and Means on March 11, 2020.
P.L. 116-123, Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020. Provides $7.8 billion in supplemental appropriations to aid in domestic and global COVID-19 preparedness and response activities, including $6.5 billion for the Department of Health and Human Services (HHS), $0.02 billion for the Small Business Administration and $1.3 billion for foreign operations activities provided across several agencies and funding mechanisms. Parts of the HHS amounts are to be made available for international activities. Enacted H.R. 6074 on March 6, 2020.
S.Amdt. 1506, To rescind unobligated balances for certain international programs to offset the amounts appropriated in this bill to respond to the coronavirus outbreak. Motion to table the amendment was agreed to in the Senate on March 5, 2020.
S.Res. 497, A resolution commemorating the life of Dr. Li Wenliang and calling for transparency and cooperation from the Government of the People's Republic of China and the Communist Party. Agreed to in the Senate on March 3, 2020 without amendment and an amended preamble by unanimous consent.
H.R. 6070, Border Health Security Act of 2020. To establish grant programs to improve the health of border area residents and for all hazards preparedness in the border area including bioterrorism, infectious disease, and noncommunicable emerging threats, and for other purposes. Referred to the House Committee on Energy and Commerce and Committee on Foreign Affairs on March 3, 2020.
S.Res. 511, A resolution supporting the role of the United States in helping save the lives of children and protecting the health of people in developing countries with vaccines and immunization through GAVI, the Vaccine Alliance. Referred to the Senate Committee on Foreign Relations, February 27, 2020.
S.Res. 505, A resolution expressing the sense of the Senate that the United States will continue to provide support to international partners to help prevent and stop the spread of coronavirus. Referred to the Senate Committee on Foreign Relations on February 13, 2020.
H.R. 2166 and S. 3302, Global Health Security Act of 2020. Establishes a Special Advisor for Global Health Security within the Executive Office of the President to coordinate U.S. government global health security activities, convene and chair a Global Health Security Interagency Review Council, and submit a biannual report to Congress on related activities, among other things. Referred to the Senate Committee on Foreign Relations on February 13, 2020.
H.R. 5730, National Strategy for Pandemic Influenza Update Act. To direct the Homeland Security Council and the National Security Council, in consultation with Federal departments and agencies responsible for biodefense, to update the National Strategy for Pandemic Influenza, and for other purposes. Referred to the House Committees on Energy and Commerce, Armed Services, Foreign Affairs, Intelligence, and Agriculture on January 30, 2020.
P.L. 116-22, Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. To advance research and development of innovative tools to improve pandemic preparedness, including directing the Secretary of Health and Human Services to submit a report to the Senate Committee on Health, Education, Labor, and Pensions and the House Committee on Energy and Commerce on U.S. efforts to coordinate with other countries and international partners during recent public health emergencies with respect to the research and advanced research on, and development of, qualified pandemic or epidemic products. Enacted S. 1379 on June 24, 2019.
H.R. 269, Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. Related to S. 1379, which became P.L. 116-22. Placed on Senate Legislative Calendar under General Orders, January 10, 2019.
|
Author |
Title |
Section/Subsection |
|
Kristin Archick |
Specialist in European Affairs |
Europe |
|
June Beittel |
Analyst in Latin American Affairs |
Canada, Latin America, and the Caribbean; Issues for Congress |
|
Paul Belkin |
Analyst in European Affairs |
Europe |
|
Maria Blackwood |
Analyst in Asian Policy |
What are the implications in Central Asia? |
|
Caitlin Campbell |
Analyst in Asian Affairs |
Taiwan |
|
Emma Chanlett-Avery |
Specialist in Asian Affairs |
South Korea |
|
Nicolas Cook |
Specialist in African Affairs |
Africa; Issues for Congress |
|
Ben Dolven |
Specialist in Asian Affairs |
What are the implications in Southeast Asia?; Singapore |
|
Hannah Fischer |
Information Research Specialist |
Selected Legislation Introduced or Enacted in the 116th Congress Related to International COVID-19 Incidence or International Pandemic Preparedness |
|
Cory Gill |
Analyst in Foreign Affairs |
U.S. Department of State; |
|
Carla Humud |
Analyst in Middle Eastern Affairs |
Middle East and North Africa |
|
James K. Jackson |
Specialist in International Trade and Finance |
International Economic and Supply Chain Issues |
|
Kenneth Katzman |
Specialist in Middle Eastern Affairs |
Middle East and North Africa |
|
K. Alan Kronstadt |
Specialist in South Asian Affairs |
What are the implications in South Asia? |
|
Susan V. Lawrence |
Specialist in Asian Affairs |
What are the implications for U.S.-China relations? |
|
Rhoda Margesson |
Specialist in International Humanitarian Policy |
What is the U.N. humanitarian response to the COVID-19 pandemic? |
|
Michael F. Martin |
Specialist in Asian Affairs |
Hong Kong |
|
Brendan W. McGarry |
Analyst in U.S. Defense Budget |
Emergency Appropriations for DOD Responses; |
|
Bryce H.P. Mendez |
Analyst in Defense Health Care Policy |
What is the DOD global COVID-19 response? |
|
Peter Meyer |
Specialist in Latin American Affairs |
Canada, Latin America, and the Caribbean |
|
Emily Morgenstern |
Analyst in Foreign Assistance and Foreign Policy |
Issues for Congress |
|
Rebecca Nelson |
Specialist in International Trade and Finance |
How are international financial institutions responding to COVID-19?; International Economic and Supply Chain Issues |
|
John Rollins |
Specialist in Terrorism and National Security |
To what extent is COVID-19 affecting United States security personnel? |
|
Tiaji Salaam-Blyther |
Specialist in Global Health |
What are coronaviruses and what is COVID-19?; How is COVID-19 transmitted?; What are global COVID-19 case fatality and hospitalization rates?; Where are COVID-19 cases concentrated?; Introduction; International Health Regulations; What is WHO doing to respond to the COVID-19 pandemic?; U.S. Agency for International Development (USAID); U.S. Centers for Disease Control and Prevention (CDC); Issues for Congress |
|
Andres Schwarzenberg |
Analyst in International Trade and Finance |
International Economic and Supply Chain Issues |
|
Michael Sutherland |
Analyst in International Trade and Finance |
International Economic and Supply Chain Issues |
|
Karen Sutter |
Specialist in Asian Trade and Finance |
International Economic and Supply Chain Issues |
|
Maureen Taft-Morales |
Specialist in Latin American Affairs |
Issues for Congress |
|
Sara Tharakan |
Analyst in Global Health |
What are coronaviruses and what is COVID-19?; What are global COVID-19 case fatality and hospitalization rates?; Where are COVID-19 cases concentrated?; Introduction; Emergency Appropriations for International Responses |
|
Clayton Thomas |
Analyst in Middle Eastern Affairs |
What are the implications for U.S. withdrawal from Afghanistan? |
|
Bruce Vaughn |
Specialist in Asian Affairs |
What are the implications in South Asia?; What are the implications in Australia and New Zealand?; Australia; New Zealand |
|
Martin Weiss |
Specialist in International Trade and Finance |
How are international financial institutions responding to COVID-19?; International Economic and Supply Chain Issues |
Author Contact Information
Footnotes
| 1. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health, and Sara Tharakan, Analyst in Global Health. |
| 2. |
CDC, "Human Coronavirus Types," accessed February 14, 2020, https://www.cdc.gov/coronavirus/types.html. |
| 3. |
For background on COVID-19, see the CDC, "Coronavirus Disease 2019 (COVID-19): Situation Summary, Updated April 19, 2020; and WHO, "Q&A on coronaviruses (COVID-19)," Q&A, April 8, 2020. |
| 4. |
The International Committee on Taxonomy of Viruses initially named the virus novel coronavirus (2019-nCoV), and WHO later dubbed it severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), see https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it. The virus can cause disease in humans called coronavirus disease 2019 (COVID-19). |
| 5. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health. |
| 6. |
CDC, "Transmission—2019 Novel Coronavirus," accessed March 22, 2020. |
| 7. |
CDC, "Healthcare Professionals: Frequently Asked Questions and Answers – Transmission," updated March 30, 2020, accessed March 31, 2020. |
| 8. |
Leah F. Moriarty et al., "Public Health Responses to COVID-19 Outbreaks on Cruise Ships Worldwide, February-March 2020," Morbidity and Mortality Weekly Report, vol. 69, March 23, 2020. |
| 9. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health, and Sara Tharakan, Analyst in Global Health. |
| 10. |
Joseph T. Wu et al., "Estimating clinical severity of COVID-19 from transmission dynamics in Wuhan, China," Nature Medicine, March 19, 2020. |
| 11. |
David Baud et al., "Real estimates of mortality following COVID-19 infection," The Lancet Infectious Diseases, March 12, 2020. |
| 12. |
Nick Wilson et al., "Case-Fatality Risk Estimates for COVID-19 Calculated by Using a Lag Time for Fatality," Emerging Infectious Diseases, Vol. 26, No. 6, June 2020. |
| 13. |
Zhang Yanping, "The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China," Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Control and Prevention, Chinese Journal of Epidemiology, vol. 41, 2020. |
| 14. |
Zunyou Wu and Jennifer McGoogan, "Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China," JAMA Network, February 24, 2020. |
| 15. |
Ibid. |
| 16. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health and Sara Tharakan, Analyst in Global Health and International Development. |
| 17. |
See WHO web page on WHO regions at https://www.who.int/chp/about/regions/en/, accessed on April 6, 2020. |
| 18. |
UNOCHA, Global Humanitarian Response Plan COVID-19: United Nations Coordinated Appeal April – December 2020, March 2020. |
| 19. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health. |
| 20. |
For more information on the IHR, see the IHR (2005) web page at https://www.who.int/ihr/about/en/. |
| 21. |
WHO, Frequently asked questions about the International Health Regulations (2005), 2009. |
| 22. |
See WHO, Global Health Observatory (GHO) Data, IHR Core Capacities Implementation: Preparedness, at https://www.who.int/gho/ihr/monitoring/preparedness/en/, accessed on March 30, 2020. |
| 23. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health. |
| 24. |
WHO web page on funding for the COVID-19 response plan, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/donors-and-partners/funding, accessed on April 13, 2020. The U.S. contributions were provided before President Donald Trump announced on April 15, 2020, that he is "placing a hold on all funding to the WHO while its mismanagement of coronavirus pandemic is investigated." See White House, "President Donald J. Trump is Demanding Accountability from the World Health Organization," Fact Sheet, April 15, 2020. |
| 25. |
WHO web page on funding for the COVID-19 response plan, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/donors-and-partners/funding, accessed on April 13, 2020. |
| 26. |
WHO, COVID-19 Strategy Update, April 14, 2020. |
| 27. |
WHO, "Global leaders unit to ensure everyone everywhere can access new vaccines, tests and treatments for COVID-19," press release, April 24, 2020. |
| 28. |
Kenan Mullis, "Playing Chicken with Bird Flu: Viral Sovereignty, the Right to Exploit Natural Genetic Resources, and the Potential Human Rights Ramifications," American University International Law Review, (2009); and Laurie Garrett and David Fidler, "Sharing H5N1 Viruses to Stop a Global Influenza Pandemic," PLoS Medicine, vol. 4, no. 11 (November 2007). |
| 29. |
Sylvie Corbet, "Sanofi walks back after saying US would get vaccine first," Associated Press News, May 14, 2020; and Henri-Pierre André and Matthias Blamont, "Sanofi CEO pledges virus vaccine for all after French backlash," Reuters, May 14, 2020. |
| 30. |
WHO webpage on the Solidarity Trials, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-clinical-trial-for-covid-19-treatments, accessed on May 14, 2020. |
| 31. |
Draft Resolution on a WHA73: "Covid-19 Response," May 18, 2020. |
| 32. |
Written by Rebecca Nelson and Martin Weiss, Specialists in International Trade and Finance. For more information, see CRS Report R46342, COVID-19: Role of the International Financial Institutions, by Rebecca M. Nelson and Martin A. Weiss. |
| 33. |
International Monetary Fund, IMF Makes Available $50 Billion to Help Address Coronavirus, March 4, 2020; World Bank, World Bank Group Announces Up to $12 Billion Immediate Support for COVID-19 Country Response¸ March 3, 2019. |
| 34. |
IMF Managing Director Kristalina Georgieva, Remarks to the G20 Finance Ministers, April 15, 2020. |
| 35. |
World Bank President David Malpass, "Remarks to G20 Finance Ministers," April 15, 2020. |
| 36. |
Written by Rhoda Margesson, Specialist in International Humanitarian Policy. |
| 37. |
International Monetary Fund, "IMF Makes Available $50 Billion to Help Address Coronavirus," March 4, 2020; World Bank, "World Bank Group Announces Up to $12 Billion Immediate Support for COVID-19 Country Response¸" March 3, 2019. |
| 38. |
U.N. News, "COVID-19: Agencies Temporarily Suspend Refugee Resettlement Travel," March 17, 2020. |
| 39. |
UNOCHA, Global Humanitarian Overview 2020, December 2019. |
| 40. |
U.N. Office for the Coordination of Humanitarian Assistance (UNOCHA), Global Humanitarian Overview 2020, December 2019. |
| 41. |
The United States is the largest humanitarian assistance donor, consistently providing nearly one-third of total global contributions. It also often takes the lead in coordinating humanitarian policy and diplomacy. |
| 42. |
Refugees are distinct from migrants because of their specific status and protections under international law. While economic migrants, which numbered approximately 272 million in 2019 (approximately 3.5% of the global population), move voluntarily often to leave poverty and unemployment to seek better opportunities or family reunification, increasingly vulnerable migrants are forced to flee, which only compounds global displacement challenges. International Organization for Migration (IOM), World Migration Report, 2020, November 27, 2019. |
| 43. |
UNOCHA, Global Humanitarian Overview 2020, December 2019; Internal Displacement Monitoring Center, Global Report on Internal Displacement 2019, May 10, 2019; International Rescue Committee, "Climate Change: Climate Change Displacement is Happening Now," March 19, 2019; UNHCR, "Climate Change and Displacement," October 15, 2019. |
| 44. |
Kurtzer, Jacob, "The Impact of COVID-19 on Humanitarian Crises," CSIS: Critical Questions, March 19, 2020; Colum Lynch and Robbie Gramer, "The Next Wave: U.N. and Relief Agencies Warn the Coronavirus Pandemic Could Leave an Even Bigger Path of Destruction in the World's Most Vulnerable and Conflict-riven Countries," Foreign Policy, March 23, 2020; Roald, Høvring, "Ten Things You Should Know About Coronavirus and Refugees, Norwegian Refugee Council, March 16, 2020. |
| 45. |
For example, this includes displaced populations caught in conflict in northwest Syria, crowded camps such as those in Bangladesh and the Dadaab camp in Kenya, and a highly vulnerable population in Yemen that is on the brink of famine and facing cholera outbreaks. |
| 46. |
The New Humanitarian, "Behind the Headlines: How will COVID-19 impact crisis zones?" Live Stream, March 19, 2020. |
| 47. |
UNHCR, Global Trends in Forced Displacement, June 19, 2019 (data for 2018, which is the latest available.) |
| 48. |
Low or middle-income countries host 85% of refugees worldwide. UNHCR, Global Trends in Forced Displacement, June 19, 2019 (data for 2018, which is the latest available.) See also, CDC, "Coronavirus Disease 2019 (COVID-19), World Map: Locations with Confirmed COVID-19 Cases, by WHO Region," March 24, 2020. |
| 49. |
UNOCHA, Global Humanitarian Response Plan COVID-19: United Nations Coordinated Appeal April – December 2020, March 25, 2020. |
| 50. |
UNOCHA, Global Humanitarian Response Plan COVID-19: United Nations Coordinated Appeal April-December 2020, May update, May 7, 2020. |
| 51. |
Ibid. |
| 52. |
UN News, "COVID-19: UN and partners launch $6.7 billion appeal for vulnerable countries," press release, May 7, 2020. |
| 53. |
Inter-Agency Standing Committee, COVID-19 Outbreak Readiness and Response, accessed March 24, 2020. |
| 54. |
The New Humanitarian, "Behind the Headlines: How will COVID-19 impact crisis zones?" Live Stream, March 19, 2020; Colum Lynch and Robbie Gramer, "The Next Wave: U.N. and Relief Agencies Warn the Coronavirus Pandemic Could Leave an Even Bigger Path of Destruction in the World's Most Vulnerable and Conflict-riven Countries," Foreign Policy, March 23, 2020. |
| 55. |
White House, Statement from the Press Secretary Regarding the President's Coronavirus Task Force, Washington, DC, January 29, 2020. |
| 56. |
White House, Remarks by President Trump, Vice President Pence, and Members of the Coronavirus Task Force in Press Conference, Washington, DC, February 27, 2020. White House, Vice President Pence Announces Ambassador Debbie Birx to Serve as the White House Coronavirus Response Coordinator, Washington, DC, February 27, 2020. |
| 57. |
Members of the Task Force include: Dr. Deborah Birx, White House Coronavirus Response Coordinator; Secretary Alex Azar, HHS; Robert O'Brien, Assistant to the President for National Security Affairs; Dr. Robert Redfield, CDC Director; Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases at NIH, Deputy Secretary Stephen Biegun, Department of State, Ken Cuccinelli, Acting Deputy Secretary Department of Homeland Security, Joel Szabat, Acting Under Secretary for Policy, Department of Transportation; Matthew Pottinger, Assistant to the President and Deputy National Security Advisor; Rob Blair, Assistant to the President and Senior Advisor to the Chief of Staff; Joseph Grogan, Assistant to the President and Director of the Domestic Policy Council; Christopher Liddell, Assistant to the President and Deputy Chief of Staff for Policy Coordination; and Derek Kan, Executive Associate Director, Office of Management and Budget (OMB). |
| 58. |
Written by Sara Tharakan, Analyst in Global Health. |
| 59. |
This section focuses on funds specified by Congress for international activities. Funds from other sources, such as the Infectious Disease Rapid Response Reserve Fund (IDRRF), may be made available for international responses. |
| 60. |
Congress authorized the ERF through the Consolidated Appropriations Act of 2017, P.L. 115-31, "to enable the United States and the international public health community to respond rapidly to emerging health threats." |
| 61. |
Written by Cory Gill, Analyst in Foreign Affairs. |
| 62. |
See 22 U.S.C. §2715. |
| 63. |
U.S. Department of State, "Global Level 4 Health Advisory – Do Not Travel." |
| 64. |
U.S. Department of State, "7 FAM 042 Appendix A: Travel Advisory Information," Foreign Affairs Manual. |
| 65. |
U.S. Department of State, "Global Level 4 Health Advisory – Do Not Travel." |
| 66. |
U.S. Department of State, "7 FAM 000 Appendix A: Consular Information Program," Foreign Affairs Manual. |
| 67. |
U.S. Department of State, "7 FAM 057.1 Appendix A: Health Information Definition," Foreign Affairs Manual. |
| 68. |
U.S. Department of State, "Current Outbreak of Coronavirus Disease 2019." |
| 69. |
U.S. Department of State, "COVID-19 Country Specific Information." |
| 70. |
U.S. Department of State, "Coronavirus Congressional Information." |
| 71. |
See 22 U.S.C. §4802. |
| 72. |
See 22 U.S.C. §2671 |
| 73. |
See 22 U.S.C. §2671. |
| 74. |
U.S. Department of State, "Global Level 4 Health Advisory – Do Not Travel." |
| 75. | |
| 76. |
U.S. Department of State, "Briefing on COVID-19: Updates on Health Impact and Assistance for American Citizens Abroad, April 3, 2020." |
| 77. | |
| 78. |
See Division G, Title I, of P.L. 116-94. |
| 79. |
White House, Office of Management and Budget, "A Budget for America's Future," Appendix, p. 813. As a result, the department has carried over large balances of unexpired, unobligated EDCS funds each year. Prior to the onset of the COVID-19 pandemic, the Office of Management and Budget (OMB) estimated that the State Department would carry forward $248 million in EDCS funds in FY2021. |
| 80. |
See Section 7009(a) of P.L. 116-94. |
| 81. |
See Section 403 of P.L. 116-123. |
| 82. |
U.S. Department of State, "Department of State Coronavirus Repatriation Statistics." |
| 83. |
U.S. Department of State, "Global Level 4 Health Advisory – Do Not Travel." |
| 84. |
Sam Mintz, "Americans remain stranded abroad as State Department struggles to respond," Politico, March 25, 2020. |
| 85. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health. |
| 86. |
Countries include: Afghanistan, Albania, Angola, Armenia, Azerbaijan, Bangladesh, Belarus, Bosnia and Herzegovina, Burkina Faso, Burma, Cambodia, Cameroon, the Caribbean, Central Africa Republic, Colombia, Cote d'Ivoire, Democratic Republic of the Congo, Ethiopia, Georgia, Haiti, India, Indonesia, Iraq, Jamaica, Kazakhstan, Kenya, Kosovo, Kyrgyzstan, Laos, Libya, Moldova, Mongolia, Morocco, Mozambique, Nepal, Nigeria, North Macedonia, Pacific Islands, Pakistan, Papua New Guinea, Philippines, Rwanda, Senegal, Serbia, Somalia, South Africa, South Sudan, Sri Lanka, Sudan, Syria, Tajikistan, Tanzania, Thailand, Timor Leste, Tunisia, Turkmenistan, Ukraine, Uzbekistan, Venezuela, Vietnam, Zambia, Zimbabwe, and Regional Efforts in Asia. See U.S. Department of State Fact Sheet "Humanitarian and Health Assistance Response to COVID-19" March 26, 2020. |
| 87. |
For more information on the Global Health Security Index, see https://www.nti.org/about/projects/global-health-security-index/. |
| 88. |
USAID, COVID-19-Global Response, Fact Sheet #2, Fiscal Year 2020, May 5, 2020. |
| 89. |
USAID, "USAID: Investments in Global Health Security By the U.S. Agency for International Development," Fact Sheet, May 7, 2020. |
| 90. |
Written by Tiaji Salaam-Blyther, Specialist in Global Health. |
| 91. |
Written by Bryce H.P. Mendez, Analyst in Defense Health Care Policy. |
| 92. |
DOD defines health surveillance as "regular or repeated collection, analysis, and interpretation of health-related data and the dissemination of information to monitor health of a population and to identify potential risks to health, thereby enabling timely interventions to prevent, treat, or control disease and injury." DOD defines medical surveillance as "ongoing, systematic collection, analysis, and interpretation of data derived from instances of medical care or medical evaluation, and the reporting of population-based information for characterizing and countering threats to a population's health, well-being, and performance." DOD Directive 6490.02, Comprehensive Health Surveillance, updated August 28, 2017, p. 11. |
| 93. |
Military Health System (MHS), "MHS prepared to support interagency coronavirus response," February 6, 2020. The Defense Health Agency's Armed Forces Health Surveillance Branch is conducting the daily monitoring. For more on this branch, see https://health.mil/Military-Health-Topics/Combat-Support/Armed-Forces-Health-Surveillance-Branch/Global-Emerging-Infections-Surveillance-and-Response. |
| 94. |
Ibid. Naval Medical Research Unit-2 in Phnom Penh, Cambodia is performing this surveillance activity. For more on the research unit, see https://www.med.navy.mil/sites/nmrca/SitePages/Home.aspx. |
| 95. |
MHS, "MHS prepared to support interagency coronavirus response," February 6, 2020. For more on the DOD Laboratory Network and interagency network laboratories, see https://www.icln.org/about/index.html. |
| 96. |
Combatant commanders lead U.S. military operations in certain geographic areas of responsibility. For more on combatant commanders, see CRS In Focus IF10542, Defense Primer: Commanding U.S. Military Operations, by Kathleen J. McInnis. |
| 97. |
Certain military orders directing the planning or execution of military operations are often classified or not made public. However, references are made to a "SECDEF-approved EXORD [execute order] that directs USNORTHCOM to execute its pandemic plan 3551-13 and supporting geographic combatant commanders to execute their pandemic plans in response to the NCoV outbreak" in U.S. Navy, Naval Administrative Message 039/20, "Updated DOD Guidance for Monitoring Personnel Returning from China during the Novel Coronavirus Outbreak," February 11, 2020. Also see, U.S. Marine Corps, Marine Corps Administrative Message 082/20, "U.S. Marine Corps Disease Containment Preparedness Planning Guidance for 2019 Novel Coronavirus (2019 nCoV), February 11, 2020. |
| 98. |
Written by Brendan W. McGarry, Analyst in U.S. Defense Budget. |
| 99. |
DOD's Military Health System (MHS) offers health care benefits and services through its TRICARE program to approximately 9.5 million beneficiaries composed of servicemembers, military retirees, and family members. For more information, see CRS In Focus IF10530, Defense Primer: Military Health System, by Bryce H. P. Mendez. |
| 100. |
U.S. Congress, Senate Committee on Appropriations, "Shelby Urges Swift Passage of Comprehensive Coronavirus Bill," press release, March 25, 2020. |
| 101. |
Department of Defense, Coronavirus: DOD Response website, accessed April 17, 2020. |
| 102. |
Department of Defense, Department of the Air Force, Air National Guard, Tennessee Air National Guard, "Two Memphians bring much-needed supplies home," press release, April 3, 2020. |
| 103. |
Ellen Mitchell, "Air Force moves 500K coronavirus test swabs from Italy to US," The Hill, March 18, 2020. |
| 104. |
Written by John Rollins, Specialist in Terrorism and National Security. |
| 105. |
The section of the paper focuses on personnel-related issues as it pertains to conducting normal operations. Another significant concern, not addressed in this section, entails the possible redirection of personnel and financial and equipment resources redirected from traditional security missions to address COVID-19 concerns. |
| 106. |
Ellen Mitchell, "Pentagon orders military bases to stop releasing specific COVID-19 numbers," March 30, 2020. |
| 107. |
Molly O'Toole, "Coronavirus has sidelined roughly 9,000 Homeland Security employees, internal report shows," April 1, 2020. |
| 108. |
Lucy Craymer, "Virus Grounds a U.S. Aircraft Carrier as Crew Quarantined in Guam," The Wall Street Journal, April 1, 2020. |
| 109. |
Written by Susan V. Lawrence, Specialist in Asian Affairs. |
| 110. |
Ministry of Foreign Affairs of the People's Republic of China, "Foreign Ministry Spokesperson Hua Chunying's Daily Briefing Online," February 3, 2020. |
| 111. |
U.S. Embassy and Consulates in China, "The United States Announces Assistance to the COVID-19," February 7, 2020. |
| 112. |
U.S. Department of State, "Secretary Michael R. Pompeo with Tony Perkins of Washington Watch," March 24, 2020. |
| 113. |
Tweet by Zhao Lijian, March 12, 2020. Zhao was alluding to a conspiracy theory that a U.S. military athlete participating in the October 2019 World Military Games in Wuhan could have brought the virus to China. For discussion, see Renée DiResta, "For China, the 'USA Virus' Is a Geopolitical Ploy," The Atlantic, April 11, 2020. |
| 114. |
U.S. Department of State, "Secretary Michael R. Pompeo's Remarks to the Press," March 17, 2020; and The White House, "Remarks by President Trump, Vice President Pence, and Members of the Coronavirus Task Force in Press Briefing," March 18, 2020. |
| 115. |
The White House, "Remarks by President Trump in Press Briefing," April 14, 2020, https://www.whitehouse.gov/briefings-statements/remarks-president-trump-press-briefing/. |
| 116. |
See, for example, U.S. Department of State, "Secretary Michael R. Pompeo with Hugh Hewitt of The Hugh Hewitt Show," April 17, 2020, https://www.state.gov/secretary-michael-r-pompeo-with-hugh-hewitt-of-the-hugh-hewitt-show-3/. |
| 117. |
The White House, "Remarks by President Trump on Protecting America's Seniors," May 1, 2020, https://www.whitehouse.gov/briefings-statements/remarks-president-trump-protecting-americas-seniors/. |
| 118. |
Office of the Director of National Intelligence, "Intelligence Community Statement on Origins of COVID-19," April 30, 2020, https://www.dni.gov/index.php/newsroom/press-releases/item/2112-intelligence-community-statement-on-origins-of-covid-19. |
| 119. |
Tweet by Hua Chunying, "24 LIES & FACTS about #COVID19," May 10, 2020, https://twitter.com/SpokespersonCHN/status/1259376944400891904. "Reality Check of US Allegations Against China on COVID-19," Xinhua, May 10, 2020, http://www.xinhuanet.com/english/2020-05/10/c_139044103.htm. |
| 120. |
Tweet by Hua Chunying, May 8, 2020, https://twitter.com/SpokespersonCHN/status/1258780531707109377. |
| 121. |
Evan A. Feigenbaum, "Why the United States and China Forgot How to Cooperate," April 28, 2020, https://carnegieendowment.org/2020/04/28/why-united-states-and-china-forgot-how-to-cooperate-pub-81673. |
| 122. |
Thomas J. Christensen, "A Modern Tragedy? COVID-19 and U.S.-China Relations," May 2020, https://www.brookings.edu/research/a-modern-tragedy-covid-19-and-us-china-relations/. |
| 123. |
Cui Tiankai, "Chinese Ambassador: Ignoring the Facts to Blame China Will Only Make Things Worse," May 5, 2020, https://www.washingtonpost.com/opinions/chinese-ambassador-cui-tiankai-blaming-china-will-not-end-this-pandemic/2020/05/05/4e1d61dc-8f03-11ea-a9c0-73b93422d691_story.html. |
| 124. |
"Trump on China: 'We Could Cut Off the Whole Relationship," Fox Business, May 14, 2020, https://www.foxbusiness.com/politics/trump-on-china-we-could-cut-off-the-whole-relationship. |
| 125. |
Written by Ben Dolven, Specialist in Asian Affairs. |
| 126. |
Y. Rusmana and H. Suhartono, "Indonesia has Recent Rise in Covid Cases, Taking Total to 2,738," Bloomberg, April 7, 2020; John McBeth, "Why Indonesia has the World's Highest COVID-19 Death Rate," Asia Times. March 20, 2020. |
| 127. |
"Malaysia Reaches 131 New Coronavirus Case; 3,793 in Total with One New Death," The New York Times, April 6, 2020. |
| 128. |
UN News, "'Toxic Lockdown Culture' of Repressive Coronavirus Measures Hits Most Vulnerable," April 27, 2020. |
| 129. |
Human Rights Watch, "Cambodia: Emergency Bill Recipe for Dictatorship," April 2, 2020. |
| 130. |
International Institute for Strategic Studies, Update on the 2020 IISS Shangri-La Dialogue: Asia Security Summit, March 27, 2020. |
| 131. |
Written by Maria Blackwood, Analyst in Asian Policy. |
| 132. |
Maximillian Hess, "Central Asia's Force Majeure Fears: Impact of COVID-19 Outbreak on China's Natural Gas Supply Demands," Foreign Policy Research Institute, March 16, 2020; Bruce Pannier, "Analysis: Do Oil Price Cuts Signal Bad Economic Times Will Return to Central Asia?" Radio Free Europe/Radio Liberty, March 14, 2020. |
| 133. |
Human Rights Watch, "Central Asia: Respect Rights in Covid-19 Responses," April 23, 2020; Manshuk Asautai, "Podpiska o nerazglashenii dannykh sledstviia—sredstvo davleniia?" Radio Azattyq, May 4, 2020; Aida Dzhumashova, "Sredstvam massovoi informatsii razreshili rabotat' s 11 maia," 24.kg, April 29, 2020; Bakhmaner Nadirov, "V Tadzhikistane zablokiroali sait po sboru informatsii o pogibshikh COVID-19," ASIA-Plus, May 11, 2020. |
| 134. |
Written by K. Alan Kronstadt, Specialist in South Asian Affairs, and Bruce Vaughn, Specialist in Asian Affairs. |
| 135. |
For example, according to the WHO, India has 8 physicians per 10,000 residents and Pakistan has nearly 10, compared to 41 in Italy and 26 in the United States. |
| 136. |
Angel Martinez Cantera, "Can India Keep Up With COVID-19?," Diplomat (Tokyo), March 23, 2020. |
| 137. |
See the State Department release at https://go.usa.gov/xvHpH. |
| 138. |
Vikram Singh, "Can US-India Defense Progress Continue to Surge Through COVID-19?" (op-ed), Financial Express (Noida), May 8, 2020. |
| 139. |
"How India Will Play a Major Role in a Covid-19 Vaccine," BBC News, April 27, 2020. |
| 140. |
"India Allows Limited Exports of Anti-Malaria Drug After Trump Warns of Retaliation, Reuters, April 7, 2020. |
| 141. |
"In India, Coronavirus Fans Religious Hatred," New York Times, April 12, 2020; "India Uses Pandemic to Try to Muzzle Media, Press Freedom Advocates Say" (interview), NPR (online), April 30, 2020; Tariq Mir, "India is Using the Pandemic to Intensify Its Crackdown in Kashmir" (op-ed), Washington Post, April 30, 2020. |
| 142. |
"Pakistan's Imran Khan Sidelined by Military During Coronavirus Outbreak," Financial Times (London), April 24, 2020; Madiha Afzal, "Pakistan's Dangerous Capitulation to the Religious Right on Coronavirus," Washington Post, May 1, 2020. |
| 143. |
"Panic Grips Rohingya Refugee Camps in Bangladesh Over Coronavirus Concerns," Radio Free Asia, March 20, 2020; Bertil Lintner, "Rohingya Refugee Camps a Covid-19 Time Bomb," Asia Times, March 20, 2020. |
| 144. |
Ashley Westerman, "Bangladesh Sends 28 Rohingya Refugees to Cyclone Prone Island Over COVID-19 Fears," May 4, 2020. |
| 145. |
Written by Bruce Vaughn, Specialist in Asian Affairs. |
| 146. |
Karen DeYoung, "U.S., Australia Call for Global Probe of Early Response," The Washington Post, April 24, 2020. |
| 147. |
Rod McGuirk, "China Warns Australia it Could Face Boycotts Over Call for an Independent Inquiry Into Coronavirus," Time, May 1, 2020. |
| 148. |
Peter Hartcher, "China's Man in Canberra Has Unmasked the Regimes True Face," The Sydney Morning Herald, April 28, 2020. |
| 149. |
"China Berates New Zealand Over Support for Taiwan at WHO," The New York Times, May 11, 2020. |
| 150. |
"New Zealand Backs Taiwan Joining the WHO Despite China Rebuke," The Guardian, May 12, 2020. |
| 151. |
Written by Clayton Thomas, Analyst in Middle Eastern Affairs. |
| 152. |
Thomas Gibbons-Neff and Julian Barnes, "Coronavirus Disrupts Troop Withdrawal in Afghanistan," New York Times, March 18, 2020. |
| 153. |
Kylie Atwood and Ryan Browne, "US troop drawdown in Afghanistan running ahead of schedule," CNN, April 30, 2020; Carol E. Lee and Courtney Kube, "Trump tells advisors U.S. should pull troops as Afghanistan COVID-19 outbreak looms," NBC News, April 27, 2020. |
| 154. |
Sayed Salahuddin, "Skype call reconnects Taliban and Afghan officials," Arab News, March 24, 2020. |
| 155. |
Ruchi Kumar, "Taliban launches campaign to help Afghanistan fight coronavirus," Al Jazeera, April 6, 2020. |
| 156. |
Abdul Qadir Sediqi and Orooj Hakimi, "Coronavirus makes Taliban realise they need health workers alive not dead," Reuters, March 18, 2020. |
| 157. |
See Ashley Jackson, "For the Taliban, the Pandemic is a Ladder," Foreign Policy, May 6, 2020, and "The Taliban are joining Afghanistan's fight against covid-19," Economist, May 9, 2020. |
| 158. |
International Organization on Migration, Return of Undocumented Afghans Weekly Situation Report, May 3-9, 2020. See also, Jaffer Shah et al., "COVID-19: the current situation in Afghanistan," The Lancet, April 2, 2020. |
| 159. |
Written by Caitlin Campbell, Analyst in Asian Affairs. |
| 160. |
C. Jason Wang et al., "Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing," Journal of the American Medical Association, May 3, 2020. |
| 161. |
Taiwan Center for Disease Control, "Starting from February 6, 2020, China (including Hong Kong, Macau) to be listed as Level 2 Area or above; Chinese residents to be prohibited from entering Taiwan," February 5, 2020; Taiwan Centers for Disease Control, "CECC extends restrictions on direct cross-strait flights and ban on passenger transits," April 23, 2020. |
| 162. |
C. Jason Wang et al., "Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing," Journal of the American Medical Association, May 3, 2020. |
| 163. |
Other parts of the NHCCC include: the Biological Pathogen Disaster Command Center, the Counter-Bioterrorism Command Center, and the Central Medical Emergency Operations Center. |
| 164. |
C. Jason Wang et al., "Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing," Journal of the American Medical Association, May 3, 2020. |
| 165. |
Winston Wen-yi Chen, "Lessons on handling the COVID-19 outbreak from Taiwan," iPolitics, March 17, 2020. |
| 166. |
Taiwan Centers for Disease Control, "To strengthen community-based surveillance, groups with foreign travel or contact history or other groups of potential risks included in COVID-19 testing procedure," February 16, 2020; Kathrin Hille and Edward White, "Containing coronavirus: lessons from Asia," Financial Times, March 16, 2020. |
| 167. |
Laws and Regulations Database of the Republic of China, "Communicable Disease Control Act," June 19, 2019; Cindy Sui, "What Taiwan can teach the world on fighting the coronavirus," NBC News, March 10, 2020. |
| 168. |
Anders Fogh Rasmussen, "Taiwan Has Been Shut Out of Global Health Discussions. Its Participation Could Have Saved Lives," Time, March 18, 2020. |
| 169. |
Winston Wen-yi Chen, "Lessons on handling the COVID-19 outbreak from Taiwan," iPolitics, March 17, 2020. |
| 170. |
Executive Yuan, "Executive Yuan Approves Special Budget to Fund COVID-19 Response," Press Release, February 27, 2020; "CECC Announces Compensation for COVID-19 Quarantine," Taiwan Today, March 12, 2020. |
| 171. |
Written by Michael F. Martin, Specialist in Asian Affairs. |
| 172. |
"Coronavirus: Hong Kong hospital staff strike to demand closure of China border," BBC, February 3, 2020. |
| 173. |
Rachel Wong, "Closure of checkpoints with China a 'speedy' response to virus outbreak, says Hong Kong's Carrie Lam," Hong Kong Free Press, February 4, 2020; Rachel Wong and Jennifer Creery, "Coronavirus: 14-day quarantine for all arrivals to Hong Kong except from China, Macau, Taiwan," Hong Kong Free Press, March 17, 2020. |
| 174. |
Jennifer Creery, "Coronavirus: Hong Kong to ban all foreign visitors as 8,600 businesses barred from selling alcohol," Hong Kong Free Press, March 23, 2020; and The Government of the Hong Kong Special Administrative Region, "Entry restriction on non-Hong Kong residents coming from overseas extended," press release, April 6, 2020. |
| 175. |
For example, the HKSAR has created a dedicated web page, https://www.coronavirus.gov.hk/eng/index.html, to provide current COVID-19 information. |
| 176. |
These protocols include mandatory masking in patient contact areas and establishing "dirty teams" to treat riskier patients. According to a Hong Kong doctor contacted by CRS, medical professionals implemented these measures before the Hospital Authority issued instructions to do so. |
| 177. |
The Government of the Hong Kong Special Administrative Region, "Lifting of certain social distancing measures under Prevention and Control of Disease Ordinance," press release, May 5, 2020. |
| 178. |
The Government of the Hong Kong Special Administrative Region, "Gov't to distribute reusable masks," press release, May 5, 2020. |
| 179. |
Written by Ben Dolven, Specialist in Asian Affairs. |
| 180. |
Hannah Beech, "Tracking the Coronavirus: How Crowded Asian Cities Tackled an Epidemic," The New York Times, March 17, 2020. |
| 181. |
Sribala Subramanian, "How Singapore Connected the Dots on Coronavirus," The Diplomat. March 4, 2020. |
| 182. |
"Singapore Reports 287 New Coronavirus Cases in Biggest Daily Jump," U.S. News and World Report, April 9, 2020. |
| 183. |
Hilary Leung, "Singapore Was a Coronavirus Success Story – Until an Outbreak Showed How Vulnerable Workers Can Fall Through the Cracks," Time. April 29, 2020. |
| 184. |
Written by Emma Chanlett-Avery, Specialist in Asian Affairs. |
| 185. |
"Korea's Evolving Response to COVID-19," Republic of Korea Ministry of Foreign Affairs, May 11, 2020. |
| 186. |
"Korea's Fight Against COVID-19," South Korea Ministry of Foreign Affairs, March 30, 2020. |
| 187. |
"Korea's Fight Against COVID-19," South Korea Ministry of Foreign Affairs, March 30, 2020. |
| 188. |
"How South Korea Put Into Place the World's Most Aggressive Coronavirus Test Program," The Wall Street Journal, March 16, 2020. |
| 189. |
"Coronavirus: South Korea seeing a 'stabilising trend'" BBC News Video, March 15, 2020. |
| 190. |
"How South Korea Scaled Coronavirus Testing While the U.S. Fell Dangerously Behind," ProPublica, March 16, 2020. |
| 191. |
"Korea's Fight Against COVID-19," South Korea Ministry of Foreign Affairs, March 30, 2020. |
| 192. |
Written by Bruce Vaughn, Specialist in Asian Affairs. |
| 193. |
Rosie Perper, "Australia and New Zealand Have Been Able to Keep Their Number of Coronavirus Cases Low," Business Insider, April 17, 2020. |
| 194. |
"Australia's Virus Testing Rate Leads World," Financial Review, April 1, 2020. |
| 195. |
Josh Taylor, "COVID Safe App," The Guardian, April 27, 2020. |
| 196. |
O. Patrick, "Millions of Australians Get App to Track Virus," The Washington Post, April 30, 2020. |
| 197. |
Written by Bruce Vaughn, Specialist in Asian Affairs. |
| 198. |
Julia Hollingsworth, "How New Zealand 'Eliminated' COVID-19 After Weeks of Lockdown," CNN, April 28, 2020. |
| 199. |
Rt Hon. Jacinda Ardern, Major Steps Taken to Protect New Zealanders from COVID-19," March 14, 2020. Beehive.govt.nz. |
| 200. |
"Coronavirus Travel Restrictions Across the Globe," The New York Times, May 8, 2020. |
| 201. |
"PM Ardern's Full Lockdown Speech," www.newsroom.co.nz, and Anna Fifield, "New Zealand isn't Just Flattening the Curve its Squashing it," The Washington Post, April 7, 2020. |
| 202. |
"About the Tourism Industry," www.tourismnewzealand.com. |
| 203. |
"COVID-19 Key Updates," www.immigration.govt.nz. |
| 204. |
New Zealand has four COVID-19 Alert levels: Level 4 Lockdown: likely the disease is not contained; 3 Restrict: high risk the disease is not contained; 2 Reduce: the disease is contained but the risk of community transmission remains; and 1 Prepare: the disease is contained in New Zealand. "Alert Levels Summary," www.covid19.govt.nz/assets/resources/tables/COVID-19-aler-tlevels-summary |
| 205. |
Eleanor Roy, "NZ Plans to ease Coronavirus Lockdown in a Week," The Guardian, April 20, 2020. |
| 206. |
"Alert Level 2," www.covid19.govt.nz. |
| 207. |
Katherine Murphy, "Morrison and Ardern Agree on Travel 'Bubble' Between New Zealand and Australia," The Guardian, May 5, 2020. |
| 208. |
Written by Kristin Archick, Specialist in European Affairs, and Paul Belkin, Analyst in European Affairs. |
| 209. |
"Coronavirus: Europe Now Epicentre of the Pandemic, Says WHO," BBC, March 13, 2020. |
| 210. |
"Coronavirus in Europe – Live Data Tracker," Politico.eu, updated regularly at https://www.politico.eu/article/coronavirus-in-europe-by-the-numbers/. |
| 211. |
Liz Alderman and Jack Ewing, "Europe's Big Economies Brace for Sharpest Drop Since World War II," New York Times, April 8, 2020. |
| 212. |
"How European Economies Are Trying to Mitigate the Coronavirus Shock," Financial Times, March 17, 2020. |
| 213. |
Mehreen Khan, "Lagarde Bails Out Europe," Financial Times, March 19, 2020. |
| 214. |
European Council, Eurogroup Report on the Comprehensive Economic Policy Response to the COVID-19 Pandemic, April 9, 2020, at https://www.consilium.europa.eu/en/press/press-releases/2020/04/09/report-on-the-comprehensive-economic-policy-response-to-the-covid-19-pandemic/. |
| 215. |
For more information on the EU, including the Schengen Area, see CRS Report RS21372, The European Union: Questions and Answers, by Kristin Archick. |
| 216. |
David M. Herszenhorn, "Coronavirus Border Controls Imperil EU Freedoms," Politico Europe, March 16, 2020; Michael Peel, Sam Fleming, and Jim Brunsden, "EU Leaders Prepare to Close Bloc's Borders," Financial Times, March 16, 2020; Benjamin Novak and Melissa Eddy, "Closed Borders Within Europe Unleash Congestion and Chaos," New York Times, March 18, 2020. |
| 217. |
European Council, Statement by Presidents Charles Michel and Ursula von der Leyen with the Croatian Presidency on US Travel Ban Related to COVID-19, March 12, 2020. |
| 218. |
The White House, Proclamation – Suspension of Entry as Immigrants and Nonimmigrants of Certain Additional Persons Who Pose a Risk of Transmitting 2019 Novel Coronavirus, March 11, 2020; The White House, "Remarks by President Trump and Prime Minister Varadkar of Ireland Before Bilateral Meeting," March 12, 2020. |
| 219. |
James McAuley and Michael Birnbaum, "Europe Blindsided by Trump's Travel Restrictions, With Many Seeing Political Motive," Washington Post, March 12, 2020; Erik Brattberg, "Trump's Coronavirus Travel Ban Delivers a Blow to Transatlantic Relations," Carnegie Endowment for International Peace, March 13, 2020; Jeremy Shapiro, "A View from Washington: The America First Pandemic," European Council on Foreign Relations, March 19, 2020. |
| 220. |
Written by Nicolas Cook, Specialist in African Affairs. |
| 221. |
CRS Insight IN11285, Fostering Behavior Change During Disease Outbreaks: Insights from Ebola Response in Africa, among others. |
| 222. |
Katharine Houreld et al., "Virus exposes gaping holes in Africa's health systems," Reuters, May 7, 2020; and Johns Hopkins Center for Health Security, et al., 2019 Global Health Security Index, among others. |
| 223. |
AFP, "After head start on virus, Africa begins clampdown," March 17, 2020; and David Pilling, Joseph Cotterill, and Neil Munshi, "African countries move swiftly to head off coronavirus spread," Financial Times, March 18, 2020. |
| 224. |
BBC News, "Coronavirus in Africa: Whipping, shooting and snooping," April 9, 2020; Simon Allison, "The Covid-19 pandemic is a wildcard that will change politics as we know it," Mail & Guardian, March 25, 2020; and Freedom House, Heavy-Handed Pandemic Responses Could Fuel Unrest in Southern Africa, May 11, 2020, inter alia. |
| 225. |
Christopher Giles and Peter Mwai, "Coronavirus: Why are some African states easing lockdowns?," BBC News, May 4, 2020. |
| 226. |
Economist, "Africa is woefully ill-equipped to cope with covid-19," March 26, 2020; and Landry Signé and Ameenah Gurib-Fakim, "Africa is Bracing for a Head-On Collision with Coronavirus," ForeignPolicy.com, March 26, 2020. |
| 227. |
Baker McKenzie, The Impact of COVID-19 on African Trade, March 12, 2020, among others. |
| 228. |
Reuters, "Sub-Saharan Africa faces pressure from oil price shock, pandemic rout," April 3, 2020; Nikos Tsafos, "Who is Prepared for an Oil Price War?," CSIS, March 9, 2020; and Baker McKenzie, The Impact of COVID-19 on Key African Sectors, March 10, 2020. |
| 229. |
IMF, Policy Responses to COVID-19 and COVID-19 Emergency Financial Assistance; and World Bank, "Assessing the Economic Impact of COVID-19 and Policy Responses in Sub-Saharan Africa," Africa Pulse, April 2020. |
| 230. |
The Africa CDC was established in 2016, with U.S. and Chinese support. In February 2020, Trump Administration officials reportedly warned that U.S. assistance might end should the AU agency accept a Chinese offer to build its headquarters. An unnamed Administration official alleged that Chinese assistance would enable China to "steal … vast amounts of genomic data" held by the Africa CDC and its regional affiliates. China has rejected such claims. Katrina Manson and David Pilling, "US warns over Chinese 'spying' on African disease control centre," Financial Times, February 6, 2020; and China Ministry of Foreign Affairs, Daily Briefing, February 7, 2020, inter alia. |
| 231. |
Information in this paragraph drawn from Africa CDC, Outbreak Brief #17: Coronavirus Disease 2019 (COVID-19) Pandemic, May 12 2020, and prior regular Africa CDC 2020 COVID-19 outbreak briefs since January 2020. |
| 232. |
One of these reference labs, Senegal's Institute Pasteur, has partnered with Mologic, a British biotech firm, to produce a rapid mobile COVID-19 test. DiaTropix, a Senegalese diagnostic testing innovation and production entity, is to manufacture the test kits at cost, at roughly $1 per test. The effort is funded by the UK government and the Gates Foundation. Yomi Kazeem, "A Senegalese innovation lab is helping the UK develop a 10-minute coronavirus test kit," Quartz, March 11, 2020; and William Worley, "Why the UK wants a new coronavirus test to be made in Senegal," Devex, March 17, 2020. |
| 233. |
On February 22, 2020, AU Ministers of Health adopted a regional Africa Joint Continental Strategy for COVID-19 Outbreak. Africa CDC, Outbreak Brief #6: Novel Coronavirus (COVID-19) Global Epidemic, February 25, 2020. |
| 234. |
RCCs support disease surveillance, lab networks, emergency preparedness and responses, and other public health capacity building initiatives. Africa CDC, "Regional Collaborating Centres," 2020. |
| 235. |
Written by Carla Humud, Analyst in Middle Eastern Affairs and Kenneth Katzman, Specialist in Middle Eastern Affairs. |
| 236. |
For the purposes of this report, the Middle East and North Africa region (MENA), or what the State Department calls "Near East" Affairs (NEA), is defined as an area stretching from Morocco in the west to the Persian/Arabian Gulf in the east, excluding Turkey. It comprises Algeria, Bahrain, Egypt, Iraq, Israel, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Qatar, Saudi Arabia, Syria, Tunisia, United Arab Emirates, West Bank/Gaza, and Yemen. The World Health Organization refers to this area as the Eastern Mediterranean Region (EMR), which it defines as 21 countries plus the Gaza Strip and West Bank. MENA and EMR countries largely overlap. However, EMR includes some countries not covered by MENA (Afghanistan, Pakistan, Djibouti, Somalia, and Sudan). EMR does not include Israel, which the WHO classifies under its Europe regional office. |
| 237. |
Percentages based on official government figures as posted by the World Health Organization's EMR office. These figures are updated daily on Twitter @ WHOEMRO. |
| 238. |
"Pompeo says Iran must 'tell the truth' on coronavirus." AFP, February 25, 2020; "Egypt: rate of coronavirus cases 'likely to be higher than figures suggest,'" Guardian, March 15, 2020. |
| 239. |
"As covid-19 spreads, Arab states are clamping down," Economist, March 26, 2020. |
| 240. |
Human Rights Watch, "Egypt: Covid-19 Cover for New Repressive Powers," May 7, 2020. |
| 241. |
U.S. Embassy in Algeria, "COVID-19 Information: Country-Specific Information," updated as of May 11, 2020. A number of local activists had called for a temporary halt to protests prior to the new restrictions, citing public health concerns. |
| 242. |
IMF, "Press Remarks by Jihad Azour on the Economic Outlook for the Middle East and Central Asia," April 15, 2020. |
| 243. |
"Lebanon to enforce new lockdown after uptick in cases," Washington Post, May 12, 2020. |
| 244. |
Statement by WHO's Regional Director Dr. Ahmed Al-Mandhari, "Our collective fight against COVID-19," April 28, 2020. |
| 245. |
Ibid. |
| 246. |
Lewis Sanders IV, "Coronavirus: Gaza faces worst-case scenario," Deutsche Welle, March 18, 2020; Anna Ahronheim, "Concern of potential coronavirus outbreak in Gaza grows," jpost.com, March 15, 2020. |
| 247. |
CRS Report RS22967, U.S. Foreign Aid to the Palestinians, by Jim Zanotti; CRS Report R46274, The Palestinians and Amendments to the Anti-Terrorism Act: U.S. Aid and Personal Jurisdiction, by Jim Zanotti and Jennifer K. Elsea. |
| 248. |
http://www.cq.com/pdf/govdoc-5881691; https://davis.house.gov/statements/members-of-congress-call-on-un-ambassador-craft-to-restart-us-humanitarian-assistance-to-palestinians/; https://www.warren.senate.gov/imo/media/doc/2020.03.26%20Letter%20to%20State%20Dept%20re%20assistance%20to%20help%20combat%20coronavirus%20in%20Palestinian%20Territories.pdf. On April 16, the Administration announced that it would provide $5 million in International Disaster Assistance for the West Bank. To date, the Administration has not announced funding for Gaza. |
| 249. |
U.S. Department of State, "Briefing with Assistant Secretary of State David Schenker on Updates on Developments in the Middle East and North Africa," Special Briefing, March 20, 2020. |
| 250. |
For more information, see CRS Insight IN11279, COVID-19 and U.S. Iran Policy, by Kenneth Katzman. |
| 251. |
"UK presses US to ease Iran sanctions to help fight coronavirus," The Guardian, March 18, 2020. |
| 252. |
Department of the Treasury, Issuance of Iran-related Frequently Asked Question Related to Humanitarian Assistance with Regard to the Coronavirus Disease 2019 (COVID-19) outbreak in Iran. March 6, 2020. |
| 253. |
State Department. Fact Sheet. Iran's Sanctions Relief Scam. April 6, 2020. |
| 254. |
See: CRS Report R46342, COVID-19: Role of the International Financial Institutions, by Rebecca M. Nelson and Martin A. Weiss. |
| 255. |
Press release by Senator Bob Menendez and Rep. Eliot Engel, "Menendez and Engel Propose Policies for Addressing COVID19 in Iran," April 3, 2020. |
| 256. |
Written by June Beittel, Analyst in Latin American Affairs and Peter Meyer, Specialist in Latin American Affairs. |
| 257. |
Mia Rabson, "Trudeau Promises Stockpile Policies to get Overhaul to Prevent Waste," Canadian Press, April 20, 2020; and Marieke Walsh, "Trudeau Concedes Stockpile of Protective Gear Fell Short," Globe and Mail, May 2, 2020. |
| 258. |
Office of the Parliamentary Budget Officer, Scenario Analysis Update: COVID-19 Pandemic and Oil Price Shocks, April 30, 2020, p. 10. |
| 259. |
Government of Canada, "Canada's COVID-19 Economic Response Plan," May 11, 2020. |
| 260. |
Economist Intelligence Unit, "Canada Economy: Quick View - Central Bank Cuts Rates for Third Time in One Month," March 30, 2020. |
| 261. |
Office of the Parliamentary Budget Officer, Scenario Analysis Update: COVID-19 Pandemic and Oil Price Shocks, April 30, 2020, p. 6. |
| 262. |
Robert Fife, "Canada-U.S. Border Expected to Stay Closed until June 21," Globe and Mail, May 13, 2020. |
| 263. |
Andy Blatchford, "Trump's Moves to Hold Medical Supplies Tip Trudeau to China," Politico Pro, April 4, 2020; and Department of Homeland Security, Federal Emergency Management Agency, "Prioritization and Allocation of Certain Scarce or Threatened Health and Medical Resources for Domestic Use; Exemptions," 85 Federal Register 22021-22024, April 21, 2020. |
| 264. |
Johns Hopkins Center for Health Security, Economist Intelligence Unit, and the Nuclear Threat Initiative, 2019 Global Health Security Index, at https://www.ghsindex.org/. |
| 265. |
Brian Winter, "Coronavirus and Latin America: 4 Possible Outcomes," Americas Quarterly, March 9, 2020. |
| 266. |
In Nicaragua, the government has rejected the need to impose social distancing and as of mid-May claimed only a few COVID-19 related deaths. See Alfredo Zuniga, "Quick Burials in Nicaragua Hint at a Coronavirus Crisis that Officials Say Doesn't Exist," Associated Press, May 12, 2020. |
| 267. |
Anatoly Kurmanaev, Manuela Andreoni, Letícia Casado and Mitra Taj, "Latin America's Outbreaks Now Rival Europe's. But Its Options are Worse," New York Times, May 13, 2020. |
| 268. |
U.N. Economic Commission for Latin America and the Caribbean (ECLAC), 2018 Statistical Yearbook for Latin America and the Caribbean, March 2019, p. 13. |
| 269. |
Anthony Faiola, Ana Vanessa Herrero, "In Ecuador's Epicenter, Bodies in the Streets," Washington Post, April 5, 2020. |
| 270. |
See, Ana Vanessa Herrero, "Locked-down Colombians Fly Red Flags to Call for Help," Washington Post, May 11, 2020; "The Lockdown Conundrum," Economist, May 2, 2020. |
| 271. |
Human Rights Watch, "El Salvador: Inhumane Prison Lockdown Treatment," April 29, 2020. |
| 272. |
CRS Insight IN11198, Bolivia Postpones May Elections Amidst COVID-19 Outbreak, by Clare Ribando Seelke. |
| 273. |
International Monetary Fund, World Economic Outlook Database, April 2020. |
| 274. |
Written by James K. Jackson, Specialist in International Trade and Finance; Rebecca M. Nelson, Specialist in International Trade and Finance; Andres Schwarzenberg, Analyst in International Trade and Finance; Michael Sutherland, Analyst in International Trade and Finance; Karen Sutter, Specialist in Asian Trade and Finance; and Martin Weiss, Specialist in International Trade and Finance. Also see CRS In Focus IF11434, COVID-19: U.S.-China Economic Considerations. |
| 275. |
Reuters, "China's cabinet to extend Lunar New Year holidays: state broadcaster," January 26, 2020. |
| 276. |
Tian Chen and Livia Yap, "China Adds Market Support With More Cash, Strong Yuan Fix," Bloomberg, February 3, 2020, l; Don Weinland, "China steps in to support financial system as coronavirus spreads," Financial Times, February 2, 2020; and Reuters, "China pumps $79 billion into economy with bank cash reserve cut," March 13, 2020. |
| 277. |
National Bureau of Statistics of China, "Preliminary Accounting Results of GDP for the First Quarter of 2020," April 20, 2020, http://www.stats.gov.cn/english/PressRelease/202004/t20200420_1739811.html. |
| 278. |
Echo Xie, "As coronavirus epidemic eases in China, life is slowly returning to normal," South China Morning Post, March 15, 2020. |
| 279. |
Office of the United States Trade Representative, Economic and Trade Agreement Between the United States of America and the Government of the People's Republic of China, January 2020, Article 7.6.2; William Mauldin and Alex Leary, "Virus Clouds China's Prospects to Meet U.S. Trade Commitments," The Wall Street Journal, March 9, 2020. |
| 280. |
Scott Kennedy, "China's Poor Purchasing Performance: How Should the United States Respond?" Center for Strategic and International Studies, May 8, 2020, https://www.csis.org/analysis/chinas-poor-purchasing-performance-how-should-united-states-respond; Dion Rabouin, "China is nowhere near meeting the 'phase 1' trade agreement," Axios, May 7, 2020, https://www.axios.com/china-phase-1-trade-agreement-coronavirus-trump-84c1486e-0e12-4f86-b317-248c8ead3e0e.html. |
| 281. |
Wang Cong, "US president's threat to terminate phase one deal risks resurface of tit-for-tat tussle," Global Times, May 10, 2020, https://www.globaltimes.cn/content/1187923.shtml. Note: The Global Times is published by The People's Daily, an arm of China's official state media. |
| 282. |
See CRS Report R46270, Global Economic Effects of COVID-19, coordinated by James K. Jackson. |
| 283. |
International Monetary Fund, World Economic Outlook, April 14, 2020, p. v. |
| 284. |
Ibid., p. 9. |
| 285. |
Samson, Adam and Hudson Lockett, "Stocks Fall Again in Worst Week Since 2008 Crisis," The Financial Times, February 28, 2020. |
| 286. |
Foroohar, Rana, How Coronavirus Became a Corporate Credit Run, The Financial Times, March 15, 2020. |
| 287. |
For further information, see CRS Report R46304, COVID-19: China Medical Supply Chains and Broader Trade Issues, coordinated by Karen M. Sutter. |
| 288. |
Trinh Nguyen, "The Economic Fallout of the Coronavirus in Southeast Asia," Carnegie Endowment for International Peace, February 13, 2020. |
| 289. |
Finbarr Bermingham and Su-Lin Tan, "Coronavirus: China's mask-making juggernaut cranks into gear, sparking fears of over-reliance on world's workshop," South China Morning Post, March 12, 2020, https://www.scmp.com/economy/global-economy/article/3074821/coronavirus-chinas-mask-making-juggernaut-cranks-gear; U.S. Food and Drug Administration, "Coronavirus (COVID-19) Supply Chain Update," Press release, February 27, 2020, https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-supply-chain-update. |
| 290. |
For a detailed breakdown of U.S. and Chinese trade of medical supplies related to the treatment and prevention of COVID-19, see CRS Report R46304, COVID-19: China Medical Supply Chains and Broader Trade Issues, coordinated by Karen M. Sutter. |
| 291. |
Zhang Pinghui and Zhou Xin, "Coronavirus: China Shifts Responsibility Over Medical Supplies Amid Mask Shortage, Rising Death Toll," South China Morning Post, February 3, 2020, updated on February 14, 2020, https://www.scmp.com/economy/china-economy/article/3048744/coronavirus-mask-shortage-prompts-beijing-tweak-authority; Finbarr Bermingham and Su-Lin Tan, "Coronavirus: China's Mask Making Juggernaut Cranks Into Gear, Sparking Fears of Overreliance on World's Workshop," South China Morning Post, March 12, 2020, https://www.scmp.com/economy/global-economy/article/3074821/coronavirus-chinas-mask-making-juggernaut-cranks-gear; Engen Tham, Cheng Leng, and Zhang Yan, "Exclusive: Unilever, 3M on List of Firms Eligible for China Loans to Ease Coronavirus Crisis—Sources," Reuters, February 19, 2020, https://www.reuters.com/article/us-china-health-lending-exclusive-idUSKBN20D0SQ; Yang Jian, "GM, Wuling Venture Begins Output of Machines to Make Face Masks, Automotive News, February 20, 2020, https://www.autonews.com/china/gm-wuling-venture-begins-output-machines-make-face-masks; and Luffy Liu, "700 Tech Companies in China Have Begun Making Masks," EE Times, February 13, 2020, https://www.eetimes.com/700-tech-companies-in-china-have-begun-making-masks/. |
| 292. |
"Circular on Further Facilitating the Import and Export of Technology During the Period of Epidemic Prevention and Control," PRC Ministry of Commerce, February 4, 2020, http://english.mofcom.gov.cn/article/newsrelease/significantnews/202002/20200202934774.shtml; and "Circular on Actively Expanding Imports to Combat Against Novel Coronavirus Epidemic," PRC Ministry of Commerce, February 6, 2020, http://english.mofcom.gov.cn/article/newsrelease/significantnews/202002/20200202. |
| 293. |
Keith Bradsher and Liz Alderman, "The World Needs Masks. China Makes Them—But Has Been Hoarding Them," The New York Times, March 16, 2020, https://www.nytimes.com/2020/03/13/business/masks-china-coronavirus.html. |
| 294. |
Li Yan, "Xi Says China to Send More Medical Experts to Italy," Xinhua, March 17, 2020, http://www.ecns.cn/m/news/politics/2020-03-17/detail-ifzunmih1236562.shtml934157.shtml, and "Mask Diplomacy' From Beijing to Change Narrative About COVID-19," SupChina, March 23, 2020, https://supchina.com/2020/03/23/mask-diplomacy-from-beijing-to-change-narrative-about-covid-19/. |
| 295. |
Written by June Beittel, Analyst in Latin American Affairs, Tiaji Salaam-Blyther, Specialist in Global Health; Nicolas Cook, Specialist in African Affairs; Emily Morgenstern, Analyst in Foreign Assistance and Foreign Policy; and Maureen Taft-Morales, Specialist in Latin American Affairs. |
| 296. |
USAID, "U.S. Provides Personal Protective Equipment to the Royal Thai Government to Assist COVID-19 Response," Press Release, March 9, 2020; U.S. Representative Mo Brooks et al. letter to Vice President Michael Pence regarding the use of the USAID stockpile, April 2, 2020. |
| 297. |
For more information on ICE's Enforcement and Removal Operations in response to COVID-19, see ICE, Enforcement and Removal Operations: COVID-19 Pandemic Response Requirements, April 10, 2020. Also see "ICE Guidance on COVID-19," web page, accessed on April 13, 2020. Senator Bob Menendez et al., "Threat of Deportation May Discourage Undocumented Immigrants from Seeking Medical Care for COVID-19," Press Release, March 5, 2020. Andre Paultre and Robenson Sanon, "United States deports Haitians despite coronavirus fears," Reuters, April 7, 2020. Sonia Pérez, "Guatemala: U.S. deportations driving up COVID-19 cases," Associated Press, April 15, 2020. |
| 298. |
U.S. Representative Doug Collins, "Collins Statement on SCOTUS Decision to Uphold Trump Administration's Migrant Protection Protocols," Press Release, March 11, 2020. |
| 299. |
See H.Res. 917, Expressing the sense of the House of Representatives that the United States should withhold the contribution of Federal funds to the World Health Organization until Director-General Tedros Ghebreyesus resigns and an international commission to investigate the World Health Organization is established. Senator Robert Menendez letter to Secretary of State Mike Pompeo urging the Trump Administration to provide outstanding 2019 assessments to the World Health Organization, March 26, 2020. |
| 300. |
Written by Hannah Fischer, Information Research Specialist, on May 11, 2020. |