Introduction
In December 2019, a new disease later called COVID-19 emerged in China and has quickly become a global pandemic. The disease presents major consequences for global health, foreign relations, the global economy, and global security. International institutions and country governments are taking a variety of responses to address these challenges. In the 116th Congress, Members have introduced legislation to respond to COVID-19 in particular and to address global pandemic preparedness in general that are now occurring on a global scale. This report focuses on global implications of and responses to the COVID-19 pandemic, and is organized into four broad parts that answer common questions regarding: (1) the disease and its global prevalence, (2) country and regional responses, (3) global economic and trade implications, and (4) issues that Congress might consider. For information on domestic COVID-19 cases and related responses, see CRS Insight IN11253, Domestic Public Health Response to COVID-19: Current Status and Resources Guide, by Kavya Sekar and Ada S. Cornell.
What are coronaviruses and what is COVID-19?1
Coronaviruses that typically infect humans are common pathogens, which can cause mild illnesses with symptoms similar to the common cold, or severe illness, potentially resulting in death of the victim. Prior to COVID-19, two "novel" coronaviruses (i.e., coronaviruses newly recognized to infect humans) have caused serious illness and death in large populations, namely severe acute respiratory syndrome (SARS) in 2002-2003 and Middle East Respiratory Syndrome (MERS), which was first identified in 2012 and continues to have sporadic transmission from animals to people with limited human-to-human spread.2
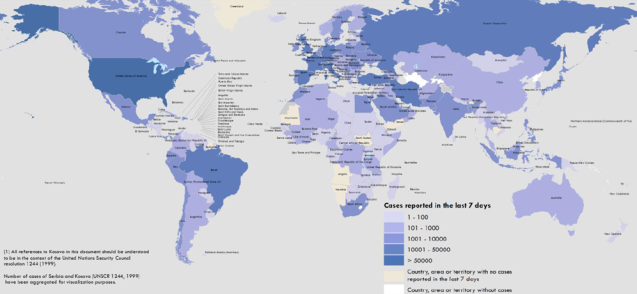
The origin of COVID-19 is unknown, although genetic analysis suggests an animal source.3 On December 31, 2019, China's government notified the World Health Organization (WHO) of pneumonia cases from unknown causes in Wuhan, China. On January 7, 2020, Chinese scientists isolated a previously unknown coronavirus in the patients, and on January 12, the scientists made its genetic sequence available to WHO and international partners. The virus is now in much of the world (Figure 1). For the purposes of this report, CRS refers to COVID-19 as the virus and the syndrome people often develop when infected.4
|
Figure 1. Confirmed COVID-19 Cases Globally, as of April 19, 2020 |
 |
|
Source: World Health Organization, COVID-19 Situation Report 90, April 19, 2020. |
How is COVID-19 transmitted?5
Health officials and researchers are still learning about COVID-19. According to the U.S. Centers for Disease Control and Prevention (CDC), the virus is thought to spread mainly from person-to-person between individuals who are in close contact with each other (less than six feet), through respiratory droplets produced when an infected person coughs or sneezes.6 Health officials and researchers are still determining the virus's incubation period, or time between infection and onset of symptoms. CDC is using 14 days as the outer bound for the incubation period, meaning that the agency expects someone who has been infected to show symptoms within that period.
The CDC has confirmed that asymptomatic cases (infected individuals who do not have symptoms) can transmit the virus, though "their role in transmission is not yet known."7 A study of the 3,711 passengers on the Diamond Princess cruise ship found that 712 people (19.2% of the cruise ship passengers) tested positive for COVID-19. Almost half (331) of the positive cases were asymptomatic at the time of testing.8
What are global COVID-19 case fatality and hospitalization rates?9
The COVID-19 case fatality rate is difficult to determine; milder cases are not being diagnosed, death is delayed, and wide disparities exist in case detection worldwide. In addition, the case fatality rate in any given context may depend on a number of factors including the demographics of the population, density of the area, and the quality and availability of healthcare services. Scientists are using different methods to estimate case fatality and estimates range. One study of those diagnosed with COVID-19 estimated case fatality rates for Wuhan, China and other parts of China at 1.4% and 0.85%, respectively.10 Another estimated 3.6% within China and 1.5% outside the country,11 with a third recommending using a range of 0.2%-3.0%.12
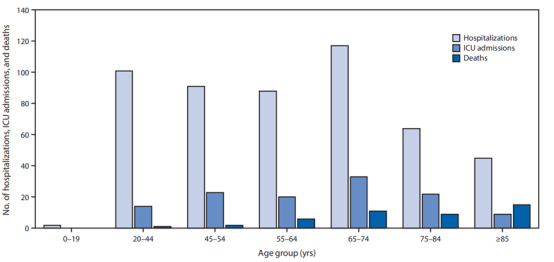
Current data suggest the elderly and those with preexisting medical conditions (including asthma, high blood pressure, heart disease, cancer, and diabetes) are more likely to become severely sickened by COVID-19. One study in China showed that 80% of those killed by the virus were older than 60 years and 81% of surveyed COVID-19 cases were mild.13 Another study showed that 87% of all hospitalized COVID-19 patients in China were aged between 30 and 79 years, though the study did not further disaggregate the data by age.14 Whereas the CDC found that the elderly had higher death rates, more than half (55%) of reported COVID-19 hospitalizations between February 12 and March 16, 2020, were younger than 65 years (Figure 2).15
Where are COVID-19 cases concentrated?16
As of April 19, 2020, national governments reported to the WHO more than 2 million cases of COVID-19 and more than 150,000 related deaths worldwide. Ten countries accounted for nearly 80% of all reported cases and almost 90% of all reported deaths (Table 1). The pandemic epicenter has shifted from China and Asia to the United States and Europe. More than half of all reported cases are now found in the WHO Europe region and less than 5% are in China (Table 2).17 In most countries, the number of reported COVID-19 deaths have not exceeded 1,000. The virus has reportedly killed more than 1,000 people in 14 countries (the ten in Table 1, Switzerland, Sweden, Brazil, and Canada).
|
Country |
Cases |
Deaths |
% of All Cases |
% of All Deaths |
|
United States |
695,353 |
32,427 |
31.0 |
21.3 |
|
Spain |
191,726 |
20,043 |
8.6 |
13.1 |
|
Italy |
175,925 |
23,227 |
7.8 |
15.2 |
|
Germany |
139,897 |
4,294 |
6.2 |
2.8 |
|
France |
110,721 |
19,294 |
4.9 |
12.6 |
|
United Kingdom |
114,221 |
15,464 |
5.1 |
10.1 |
|
China |
84,201 |
4,642 |
3.8 |
3.0 |
|
Iran |
80,868 |
5,031 |
3.6 |
3.3 |
|
Turkey |
82,329 |
1,890 |
3.7 |
1.2 |
|
Belgium |
37,183 |
5,453 |
1.7 |
3.6 |
|
Top Ten Total |
1,712,424 |
131,765 |
76.4 |
86.4 |
|
Grand Total |
2,241,778 |
152,551 |
100.0 |
100.0 |
Source: WHO, Coronavirus Disease 2019 (COVID-19) Situation Report 90, April 19, 2020.
Notes: Numbers include domestic and repatriated cases. WHO's China case count includes cases reported in Hong Kong and Macao, both Special Administrative Regions of the People's Republic of China. Because WHO treats self-governing Taiwan as a province of China, WHO also includes Taiwan cases in its China case count. Taiwan, which also calls itself the Republic of China, has protested this practice, and has sought international support for its efforts to participate in WHO in its own right. The Taiwan Centers for Disease Control reports that as of April 15, 2020 it had identified a total of 395 COVID-19 cases, including 6 deaths.
|
WHO Region |
Cases |
Deaths |
% of All Cases |
% of All Deaths |
|
Europe |
1,112,189 |
100,938 |
50.1 |
66.2 |
|
Americas |
821,860 |
38,258 |
36.7 |
25.1 |
|
Western Pacific |
131,115 |
5,621 |
5.8 |
3.7 |
|
Eastern Mediterranean |
124,691 |
5,908 |
5.6 |
3.9 |
|
Southeast Asia |
27,319 |
1,185 |
1.2 |
0.8 |
|
Africa |
13,892 |
628 |
0.6 |
0.4 |
|
Diamond Princess |
712 |
13 |
0.0 |
0.0 |
|
Total |
2,241,778 |
152,551 |
100.0 |
100.0 |
Source: WHO, Coronavirus Disease 2019 (COVID-19) Situation Report 90, April 19, 2020..
Note: WHO regions at https://www.who.int/chp/about/regions/en/, accessed on April 6, 2020.
COVID-19 Responses of International Institutions
Individual countries carry out both domestic and international efforts to control the COVID-19 pandemic, with the WHO issuing guidance, coordinating some international research and related findings, and coordinating health aid in low-resource settings. Countries follow (to varying degrees) WHO policy guidance on COVID-19 response and leverage information shared by WHO to refine national COVID-19 plans. The United Nations (U.N.) Office for the Coordination of Humanitarian Affairs (UNOCHA) is requesting $2.01 billion to support COVID-19 efforts by several U.N. entities (see "Multilateral Technical Assistance" section).18
International Health Regulations19
What rules guide COVID-19 responses worldwide?
WHO is the U.N. agency responsible for setting norms and rules on global health matters, including on pandemic response. The organization also develops and provides tools, guidance and training protocols. In 1969, the World Health Assembly (WHA)—the governing body of WHO—adopted the International Health Regulations (IHR) to stop the spread of six diseases through quarantine and other infectious disease control measures. The WHA has amended the IHR several times, most recently in 2005.20 The 2005 edition, known as IHR (2005), provided expanded means for controlling infectious disease outbreaks beyond quarantine. The regulations include a code of conduct for notification of and responses to disease outbreaks with pandemic potential, and carry the expectation that countries (and their territories) will build the capacity, where lacking, to comply with IHR (2005). The regulations mandate that WHO Member States:
- build and maintain public health capacities for disease surveillance and response;
- provide or facilitate technical assistance to help low-resource countries develop and maintain public health capacities;
- notify WHO of any event that may constitute a Public Health Emergency of International Concern (PHEIC) and respond to requests for verification of information regarding such event; and
- follow WHO recommendations concerning public health responses to the relevant PHEIC.
Per reporting requirements of the IHR (2005), China and other countries are monitoring and reporting COVID-19 cases to WHO. Observers are debating the extent to which China is fully complying with IHR (2005) reporting rules (see "Asia").
How does WHO respond to countries that do not comply with IHR (2005)?
IHR (2005) does not have an enforcement mechanism. WHO asserts that "peer pressure and public knowledge" are the "best incentives for compliance."21 Consequences that WHO purports non-compliant countries might face include a tarnished international image, increased morbidity and mortality of affected populations, travel and trade restrictions imposed by other countries, economic and social disruption, and public outrage.
China's response to the COVID-19 outbreak may deepen debates about the need for an IHR enforcement mechanism. On one hand, questions about the timeliness of China's reporting of the COVID-19 outbreak and questions about China's transparency thereafter might bolster arguments in favor of an enforcement mechanism. On the other hand, critics of an enforcement mechanism might point to assertions by the WHO Director-General Tedros Adhanom Ghebreyesus that some actions by China's government, despite contravening IHR (2005), have appeared to delay the global spread of COVID-19.
What does the Global Health Security Agenda (GHSA) have to do with IHR (2005) and pandemic preparedness?
IHR (2005) came into force in 2007, with signatory countries committing to comply by 2012. In 2012, only 20% of countries reported to the WHO that they had developed IHR (2005) core capacities, and many observers asserted the regulations needed a funding mechanism to help resource-constrained countries with compliance. In 2014, the WHO launched the Global Health Security Agenda (GHSA) as a five-year (2014-2018) multilateral effort to accelerate IHR (2005) implementation, particularly in resource-poor countries lacking the capacity to adhere to the regulations. The GHSA appeared to advance global pandemic preparedness capacity with more than 70% of surveyed countries reporting in 2017 being prepared to address a global pandemic.22 Regional disparities persisted, however; about 55% of surveyed countries in the WHO Africa region reported being prepared for a pandemic, compared to almost 90% of countries surveyed in the WHO Western Pacific region. In 2017, participating countries agreed to extend the GHSA through 2024. For more information on the GHSA, see CRS In Focus IF11461, The Global Health Security Agenda (GHSA): 2020-2024, by Tiaji Salaam-Blyther.
Multilateral Technical Assistance
What is WHO doing to respond to the COVID-19 pandemic?23
In February 2020, WHO released a $675 million Strategic Preparedness and Response Plan for February through April 2020. WHO aims to provide international coordination and operational support, bolster country readiness and response capacity—particularly in low-resource countries—and accelerate research and innovation. As of April 17, private donors and 17 countries had contributed $368.4 million towards the plan, including $14.7 million from the United States.24 Countries have pledged an additional $157.9 million towards the plan. As of April 7, the funds have been used to
- purchase and ship personal protective equipment (PPE) to 133countries, including
- 974,000 surgical masks and masks,
- 1,000,000 boxes of gloves,
- 115,000 gowns,
- 18,000 goggles, and
- 34,000 face shields;
- supply 1,500,000 diagnostic kits to 126 countries;
- develop online COVID-19 training courses in 13 languages and one simulation exercise reaching 176,000 COVID-19 responders;
- enrolled more than 74 countries in WHO-coordinated trials to accelerate treatment research; and
- publish more than 40 technical guidance and public advice statements.25
In April 2020, WHO issued an updated plan that provided guidance for countries preparing for a phased transition from widespread transmission to a steady state of low-level or no transmission, among other things.26 The update did not include a request for additional funds.
How are international financial institutions responding to COVID-19?27
The international financial institutions (IFIs), including the International Monetary Fund (IMF), the World Bank, and the regional development banks, are mobilizing their financial resources to support countries grappling with the COVID-19 pandemic.28 The IMF has announced it is ready to tap its total lending capacity, about $1 trillion, to support governments responding to COVID-19. The World Bank can mobilize about $150 billion over the next 15 months, and the regional development banks are also preparing new programs and redirecting existing programs to help countries respond to the economic ramifications of COVID-19. According to the World Bank, its support will cover a wide range of activities, including strengthening health services and primary health care, bolstering disease monitoring and reporting, training front line health workers, encouraging community engagement to maintain public trust, and improving access to treatment for the poorest patients. Through the stimulus legislation (P.L. 116-136), Congress is accelerating increased U.S. contributions to several IFIs. Many policy experts are discussing additional resources and policies that the IFIs could pursue to help address the crisis, including the creation of new IFI lending facilities and large-scale debt relief. Some of these policy initiatives would require congressional approval to go forward.
What is the U.N. humanitarian response to the COVID-19 pandemic?29
Outside of the WHO, other U.N. entities and their implementing partners are considering how to maintain ongoing humanitarian operations while preparing for COVID-19 cases should they arise.30 On March 17, 2020, the International Organization for Migration (IOM) and the U.N. High Commissioner for Refugees (UNHCR) announced they were suspending global resettlement travel for refugees due to the COVID-19 travel bans.31 Cessation of resettlement may reinforce population density in refugee camps and other settlements, which might further complicate efforts to address COVID-19 outbreaks in such settings.
Many experts agree that even prior to the COVID-19 pandemic, the scope of current global humanitarian crises was unprecedented. The U.N. Office for the Coordination of Humanitarian Affairs (UNOCHA) estimated that in 2020, nearly 168 million people in 53 countries would require humanitarian assistance and protection due to armed conflict, widespread or indiscriminate violence, and/or human rights violations.32 The 2020 U.N. global humanitarian annual appeal totaled an all-time high of more than $28.8 billion, excluding COVID-19 responses.33 The appeal also focused on the needs of displaced populations, which numbered more than 70 million people, including 25.9 million refugees, 41.3 million internally displaced persons (IDPs) and 3.5 million asylum seekers.34 In addition, natural disasters are also key drivers of displacement each year.35
Humanitarian experts agree that the conditions in which vulnerable, displaced populations live make them particularly susceptible to COVID-19 spread and present significant challenges to response and containment.36 Overcrowded living spaces and insufficient hygiene and sanitation facilities make conditions conducive to contagion.37 In many situations, disease control recommendations are not practical. Space is not available to create isolation and "social-distancing," for example, and limited access to clean water and sanitation make regular and sustained handwashing difficult.38 In addition, low or middle-income countries that are likely to struggle to respond effectively to the pandemic host 85% of refugees worldwide.39 So far, relatively few COVID-19 cases have been reported among the displaced and those affected by conflict or natural disasters, although there is a widespread lack of testing.40
On March 25, 2020, the United Nations launched a $2.01 billion global appeal for the COVID-19 pandemic response to "fight the virus in the world's poorest countries, and address the needs of the most vulnerable people" through the end of the year.41 The appeal includes support for several U.N. entities (see Table 3).
UNOCHA will coordinate the U.N.-wide response, but most of the activities will be carried out by specific U.N. entities and their implementing partners. U.N. guidance for scaling up responses in refugee and IDP settings include addressing mental health and psychological aspects, adjusting food distribution, and developing prevention and control mechanisms in schools.42 Some experts recommend incorporating COVID-19 responses within existing humanitarian programs to ensure continuity of operations and to protect aid personnel while facilitating their access in areas where travel has been restricted.43
|
U.N. Agency |
Amount |
U.N. Agency |
Amount |
|
World Health Organization (WHO) |
450.0 |
U.N. Population Fund (UNFPA) |
120.0 |
|
U.N. Children's Fund (UNICEF) |
405.0 |
Food and Agriculture Organization (FAO) |
110.0 |
|
World Food Program (WFP) |
350.0 |
International Organization for Migration (IOM) |
100.0 |
|
U.N. High Commissioner for Refugees (UNHCR) |
255.0 |
Country-specific NGO response |
100.0 |
|
U.N. Development Program (UNDP) |
120.0 |
U.N.-Habitat |
2.0 |
|
Total |
$2.01 billion |
||
Source: UNOCHA, Global Humanitarian Response Plan COVID-19: United Nations Coordinated Appeal April – December 2020, March 25, 2020.
Notes: Each U.N. agency's role in implementing the plan is described briefly on pp. 40-43 of the above cited report.
U.S. Support for International Responses
On January 29, 2020, President Donald Trump announced the formation of the President's Coronavirus Task Force, led by the Department of Health and Human Services (HHS) and coordinated by the White House National Security Council (NSC).44 On February 27, the President appointed Vice President Michael Pence as the Administration's COVID-19 task force leader, and the Vice President subsequently appointed the head of the President's Emergency Plan for AIDS Relief (PEPFAR), Ambassador Deborah Birx, as the White House Coronavirus Response Coordinator.45 International COVID-19 response efforts carried out by U.S. federal government departments and agencies, including those in the Task Force, are described below.46
Emergency Appropriations for International Responses47
On March 6, 2020, the President signed into law P.L. 116-123, Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020, which provides $8.3 billion for domestic and international COVID-19 response.48 The Act includes $300 million to continue the CDC's global health security programs and a total of $1.25 billion for the U.S. Agency for International Development (USAID) and Department of State. USAID- and Department of State-administered aid includes the following:
- Global Health Programs (GHP). $435 million for global health responses (see "U.S. Agency for International Development (USAID)"), including $200 million for USAID's Emergency Reserve Fund (ERF).49
- International Disaster Assistance (IDA). $300 million for relief and recovery efforts in the wake of the COVID-19 pandemic.
- Economic Support Fund (ESF). $250 million to address COVID-19-related "economic, security, and stabilization requirements."
The Act also provides $1 million to the USAID Office of Inspector General to support oversight of COVID-19-related aid programming.
On March 27, 2020, President Trump signed P.L. 116-136, Coronavirus Aid, Relief, and Economic Security Act, which contains emergency funding for U.S. international COVID-19 responses, including the following:
- International Disaster Assistance (IDA). $258 million to "prevent, prepare for, and respond" to COVID-19.
- Migration and Refugee Assistance (MRA). $350 million to the State Department-administered MRA account to "prevent, prepare for, and respond" to COVID-19.
U.S. Department of State50
How does the State Department help American citizens abroad?
Section 43 of the State Department Basic Authorities Act of 1956 (P.L. 84-885; hereafter, the Basic Authorities Act) requires the State Department to serve as a clearinghouse of information on any major disaster or incident that affects the health and safety of U.S. citizens abroad.51 The department implements this statutory responsibility through its Consular Information Program (CIP), which provides a range of products, including but not limited to country-specific information web pages, Travel Advisories, Alerts, and Worldwide Cautions. Travel Advisories range from Level 1 (Exercise Normal Precautions) to Level 4 (Do Not Travel).
On March 19, 2020, the State Department issued a Level 4 Global Health Advisory advising U.S. citizens to avoid international travel due to the COVID-19 pandemic.52 Level 4 Travel Advisories do not constitute a travel ban. Instead, they advise U.S. citizens not to travel because of life threatening risks and, in some cases, limited U.S. government capability to provide assistance to U.S. citizens.53 The State Department's Level 4 Global Health Advisory notes that because the State Department has authorized the departure of U.S. personnel abroad who are "at higher risk of a poor outcome if exposed to COVID-19," U.S. embassies and consulates may have more limited capacity to provide services to U.S. citizens abroad.54
CIP products are posted online and disseminated to U.S. citizens who have registered to receive such communications through the Smart Traveler Enrollment Program (STEP). The Assistant Secretary for Consular Affairs is responsible for supervising and managing the CIP. 55 State Department regulations provide that when health concerns rise to the level of posing a significant threat to U.S. citizens, the State Department will publish a web page describing the health-related threat and resources.56 The Bureau of Consular Affairs has developed such a web page for the COVID-19 pandemic.57 Additionally, the State Department has created a website providing COVID-19-related information and resources for every country in the world.58 Furthermore, on March 24, 2020, the State Department began publishing a daily COVID-19 newsletter, developed for Members of Congress and congressional staff, intended to "dispel rumor, combat misinformation, and answer any outstanding questions regarding the Department's overseas crisis response efforts."59
What are the authorities and funding for the State Department to carry out overseas evacuations?
The Omnibus Diplomatic Security and Antiterrorism Act of 1986 (P.L. 99-399) authorizes the Secretary of State to carry out overseas evacuations. Section 103 of this law requires the Secretary to "develop and implement policies and programs to provide for the safe and efficient evacuation of United States Government personnel, dependents, and private United States citizens when their lives are endangered."60 In addition, the Basic Authorities Act authorizes the Secretary to make expenditures for overseas evacuations. Section 4 of this law authorizes both expenditures for the evacuation of "United States Government employees and their dependents" and "private United States citizens or third-country nationals, on a reimbursable basis to the maximum extent practicable," leaving American citizens or third-country nationals generally responsible for the cost of evacuation, although emergency financial assistance may be available for destitute evacuees and the scope of potential repayment is limited.61
In practice, even when the State Department advises private U.S. citizens to leave a country, it will advise them to evacuate using existing commercial transportation options whenever possible. This is reflected in the State Department's current Level 4 Global Health Advisory, which states that "[i]n countries where commercial departure options remain available, U.S. citizens who live in the United States should arrange for immediate return."62 In more rare circumstances, when the local transportation infrastructure is compromised, the State Department will arrange chartered or non-commercial transportation for U.S. citizens to evacuate to a safe location determined by the department. Following the outbreak of COVID-19, the State Department has made such arrangements for thousands of U.S. citizens throughout the world, initially those in Wuhan, China and, shortly thereafter, U.S. citizen passengers who were quarantined on the Diamond Princess cruise ship in Yokohama, Japan.
Congress authorizes funding for the evacuation-related activities through the Emergencies in the Diplomatic and Consular Service (EDCS) account, which is part of the annual Department of State, Foreign Operations, and Related Programs (SFOPS) appropriation. For FY2020, Congress appropriated $7.9 million for this account.63 Congress typically funds this account through no-year appropriations, thereby authorizing the State Department to indefinitely retain funds.64 The State Department is able to further fund emergency evacuations using transfer authorities provided by Congress. In recent SFOPS appropriations, for example, Congress has authorized the State Department to transfer and merge funds appropriated to the Diplomatic Programs, Embassy Security, Construction, and Maintenance, and EDCS accounts for emergency P.L. 116-123, evacuations.65 Congress also appropriated an additional $264 million to the Diplomatic Programs account, to remain available until the end of FY2022, for purposes including the "reimbursement of evacuation expenses" (P.L. 116-123).
Congress has appropriated new funds to the Department of State's Diplomatic Programs account, on an emergency basis, to remain available through FY2022, to "prevent, prepare for, and respond to coronavirus," including through maintaining consular operations and carrying out emergency evacuations. These funds support Department of State operations and are not considered foreign assistance. They include $264 million appropriated under P.L. 116-123 and $324 million under P.L. 116-136.
How many evacuations have been carried out due to the COVID-19 pandemic?
The State Department began arranging evacuations of U.S. government personnel and private U.S. citizens in response to the COVID-19 pandemic on January 28, 2020, when the department started evacuating over 800 American citizens from Wuhan, China. An additional 300 American citizens who were passengers aboard the Diamond Princess cruise ship were subsequently evacuated in February. When COVID-19 continued to spread and was declared a global pandemic by WHO, the State Department accelerated its efforts to evacuate Americans amid actions by countries to close their borders and implement mandatory travel restrictions. On March 19, 2020, the State Department established a repatriation task force to coordinate and support these efforts. By April 8, the State Department had repatriated over 50,000 U.S. citizens on 400 flights.66 The State Department's current Level 4 Global Health Advisory warns that while the department is currently "making every effort to assist U.S. citizens overseas who wish to return to the United States, funds "may become more limited or even unavailable."67 Some Members of Congress and others have expressed concern that the State Department moved too slowly in facilitating the evacuation of Americans overseas as global COVID-19 transmission accelerated and, even after the number of evacuations ramped up, did not adequately communicate with Americans seeking the department's assistance.68
U.S. Agency for International Development (USAID)69
Where is USAID providing COVID-19 assistance?
USAID is providing assistance to more than 64 affected and at-risk developing countries facing the threat of COVID-19.70 USAID identified these countries through a combination of the following criteria:
- trend of increasing confirmed cases of COVID-19, especially with evidence of local transmission;
- imported cases with high risk for local transmission due to connectivity to a hotspot;
- low scores on the Global Health Security Index71 classification of health systems and on the Global Health Security Agenda Joint External Evaluation, which measures compliance with IHR (2005);
- other vulnerabilities (unstable political situation, displaced populations); and
- the existence of other U.S. global health programs that could be leveraged.
USAID is also providing funding to multilateral organizations, including the WHO, UNICEF, and the International Federation of the Red Cross and Red Crescent Societies for COVID-19 assistance, and to facilitate coordination with other donors.
What type of assistance does USAID provide for COVID-19 control?
On February 7, 2020, USAID committed $100 million from the Emergency Reserve Fund for Contagious Infectious Diseases. USAID received $986 million from the first emergency supplemental appropriation and an additional $353 million from the second. Examples of activities to which USAID resources will be programed include
- assisting target countries to prepare their laboratories for COVID-19 testing,
- implementing a public-health emergency plan for points of entry,
- activating case-finding and event-based surveillance for influenza-like illnesses,
- training and equipping rapid-response teams,
- investigating cases and tracing the contacts of infected persons, and
- adapting health worker training materials for COVID-19.
How do USAID COVID-19 responses relate to regular pandemic preparedness activities?
Congress appropriates funds for USAID global health security and pandemic preparedness activities through annual State, Foreign Operations, and Related Programs appropriations (Table 4). Implemented through the Emerging Pandemic Threats (EPT) program, these efforts comprise USAID's contribution towards advancing the Global Health Security Agenda (see "International Health Regulations") and will be leveraged in several countries for COVID-19 responses worldwide. Key related activities include
- strengthening surveillance systems to detect and report disease transmission;
- upgrading veterinary and other national laboratories;
- strengthening programs to combat antimicrobial resistance (AMR) in the public health and animal-health sectors;
- training community health volunteers in epidemic control and designing community-preparedness plans;
- conducting simulation exercises to prepare for future outbreaks; and
- establishing or strengthening emergency supply-chain programs specially designed to deliver critically needed commodities (e.g., personal protective equipment) to affected communities during outbreaks.
The PREDICT project, launched in 2009, is a key part of EPT. The second phase of the project, PREDICT-2 (2015-2019), reportedly helped nearly 30 countries detect and discover viruses with pandemic potential. According to USAID, the project has
- detected more than 1,100 unique viruses, 931 of which were novel viruses (such as Ebola and coronaviruses);
- sampled over 163,000 animals and people; and
- provided $207 million from 2009 through 2019.
USAID has responded to 42 outbreaks through PREDICT-2, which ended in March 2020 (following a three-month extension). The agency has not issued any formal announcements regarding the continuation of the project, though the University of California, Davis—one of the implementing organizations—has reportedly received additional funding from USAID to extend PREDICT (to a certain extent), implement the "One Health Workforce—Next Generation" project, and to facilitate USAID COVID-19 responses.72
Table 4. USAID Global Pandemic Preparedness Funding: FY2017-FY2021 Request
(current U.S. $ millions)
|
Fiscal Year |
Amount |
|
FY2017 Enacted |
72.5 |
|
FY2018 Enacted |
72.5 |
|
FY2019 Enacted |
100.0 |
|
FY2020 Enacted |
100.0 |
|
FY2021 Requested |
115.0 |
Source: Congressional budget justifications and appropriations legislation.
Notes: Excludes emergency appropriations for controlling the 2014-2016 Ebola outbreak in West Africa.
U.S. Centers for Disease Control and Prevention (CDC)73
What role is CDC playing in international COVID-19 responses?
CDC has staff stationed in more than 60 countries who have been providing technical support, where relevant, and is receptive to bilateral requests for assistance or requests for assistance through the Global Outbreak Alert and Response Network (GOARN). CDC is working with WHO and other partners, including USAID and the Department of State, to assess needs and accelerate COVID-19 control, particularly by helping countries to implement WHO recommendations related to the diagnosis and care of patients, tracking the epidemic, and identifying people who might have COVID-19.
Through supplemental appropriations (P.L. 116-123), Congress provided CDC $300 million for global disease detection and emergency response. CDC plans to obligate $150 million of the funds by the end of FY2020. Related efforts will focus on
- disease surveillance,
- laboratory diagnostics,
- infection prevention and control,
- border health and community mitigation, and
- vaccine preparedness and disease prevention.
CDC is reportedly working closely with USAID and Department of State to ensure a coordinated U.S. government approach to the COVID-19 pandemic. CDC is prioritizing countries based on
- the current status of COVID-19 in country and future trajectory of its spread;
- the ability to effectively implement activities given CDC presence, capacity and partnerships in the country; and
- the capacity to provide support to other countries in the region.
CDC staff are working with colleagues in partner countries to conduct investigations that will help inform COVID-19 response efforts.
How do CDC COVID-19 responses relate to regular pandemic preparedness activities?
Through the Global Health Protection line item of annual Labor-HHS appropriations, CDC works to enhance public health capacity abroad and improve global health security, particularly through GHSA (Table 5). CDC works to bolster global health security and pandemic preparedness in 19 countries by focusing on enhancing the core foundations of what CDC views as strong public health systems—comprehensive disease surveillance and integrated laboratory systems, a strong public health workforce, and capable emergency management structures.
Programs within CDC's global health security portfolio include the following:
- The Field Epidemiology Training Program (FETP) trains a global workforce of field epidemiologists to increase countries' ability to detect and respond to disease threats, address the global shortage of skilled epidemiologists, and deepen relationships between CDC and other countries. Over 70 countries have participated in FETP with more than 10,000 graduates.
- National Public Health Institutes (NPHI) help more than 26 partner countries carry out essential public health functions and ensure accountability for public health resources. The program focuses on improving the collection and use of public health data, as well as the development, implementation, and monitoring of public health programs.
- Global Rapid Response Team (GRRT) is a team of public health experts who remain ready to deploy for supporting emergency response and helping partner countries achieve core global health capabilities. The GRRT focuses on field-based logistics, communications, and management operations. Since the GRRT's inception, more than 500 CDC staff have provided over 30,000 person-days of response support. From January through March 2020 CDC staff has completed more than 100 deployments for COVID-19 response. Core and surge members support domestic deployments to quarantine stations and repatriation sites, international deployments, WHO and country office operations, and the Emergency Operations Center in Atlanta.
The Public Health Emergency Management (PHEM) program trains public health professionals affiliated with international ministries of health on emergency management and exposes them to the CDC Public Health Emergency Operations Center. To date, the program has graduated 142 fellows from 37 countries (plus the African Union).
|
Fiscal Year |
Amount |
|
FY2017 Enacted |
58.2 |
|
FY2018 Enacted |
108.2 |
|
FY2019 Enacted |
108.2 |
|
FY2020 Enacted |
183.2 |
Source: Correspondence with CDC, March 27, 2020.
Notes: In the Labor, HHS Appropriations, these activities are described as Global Public Health Protection. For the purposes of this report, these activities are referred to as pandemic preparedness.
U.S. Department of Defense (DOD)
What is the DOD global COVID-19 response?74
DOD is conducting medical surveillance for COVID-19 worldwide.75 Related activities entail daily monitoring of reported cases, including persons under investigation (PUI), confirmed cases, and locations of such individuals,76 as well as surveillance for COVID-19 at China's southern border.77 DOD is supporting the U.S. CDC with additional laboratory capabilities. The DOD Laboratory Network, which includes military facilities in the United States and in certain overseas locations, has made available to interagency network laboratories its "detection and characterization capabilities…to support COVID-19-related activities across the globe."78 The Secretary of Defense also has directed geographic combatant commanders79 to "execute their pandemic plans in response to the [COVID-19] outbreak."80
Emergency Appropriations for DOD Responses81
The Families First Coronavirus Response Act (P.L. 116-127) became law on March 18, 2020. Title II of Division A of the act included $82 million for the Defense Health Program to waive all TRICARE cost-sharing requirements related to COVID-19.82
The Coronavirus Aid, Relief, and Economic Security Act (CARES Act; P.L. 116-136) became law on March 27, 2020. Title III of Division B of the act included $10.5 billion in emergency funding for DOD. Of the $10.5 billion, $4.9 billion (47%) is for the Defense Health Program (DHP), according to the bill text. The DHP funding included $1.8 billion for patient care and procurement of medical and protective equipment; $1.6 billion to increase capacity in military treatment facilities; $1.1 billion for private-sector care; and $415 million to develop vaccines and to procure diagnostic tests, according to a summary released by the Senate Appropriations Committee.83 H.R. 748 also provided
- $2.5 billion for the defense industrial base, including $1.5 billion in defense working capital funds and $1 billion in Defense Production Act purchases;
- $1.9 billion in operations and maintenance (O&M) funding for the Services, in part to support deployment of the hospital ships USNS COMFORT and USNS MERCY to ease civilian hospital demand by caring for non-COVID patients; and
- $1.2 billion in military personnel (MILPERS) funding for Army and Air National Guard personnel deployments.
DOD has not detailed how much of the emergency funding may be used to support international activities related to COVID-19, though the Department has stated it is working with the Department of Health and Human Services and the Department of State to provide support in dealing with the pandemic.84 As part of missions that began in March, Air National Guard C-17 cargo aircraft have transported hundreds of thousands of coronavirus testing swabs from Italy to the United States.85 The swabs have been distributed to medical facilities around the country at the direction of the Department of Health and Human Services.86
To what extent is COVID-19 affecting United States security personnel?87
The degree to which U.S. security operations around the world may be affected due to personnel becoming infected has yet to be determined.88 Numerous media reports suggest that various parts of the U.S. military has seen a significant number of service members contract or die from COVID-19 related symptoms. Citing operational security concerns, on March 30, 2020 the Department of Defense (DoD) directed military service commanders not to share the number of personnel affected by the COVID-19. In justifying this policy the DoD stated, "We will not report the aggregate number of individual service member cases at individual unit, base or Combatant Commands. We will continue to do our best to balance transparency in this crisis with operational security."89 Also, as of April 1, 2020, reportedly the Department of Homeland Security has nearly 9,000 employees that have been exposed to COVID-19 that has taken them out of the workforce90 and deployed U.S. Naval vessels, such as the USS Theodore Roosevelt, have had their operational effectiveness called into question.91
Regional Implications of and Responses to the COVID-19 Pandemic
Asia
What are the implications for U.S.-China relations?92
U.S.-China relations were fraught well before the outbreak of COVID-19, with the two governments engaged in a bitter trade war, competing for influence around the globe, and clashing over such issues as their activities in the South China Sea, China's human rights record, and China's Belt and Road Initiative. The pandemic appears to have increased the acrimony, although since late March, the two countries have taken some efforts to rein in their more heated rhetoric. On February 3, when the COVID-19 outbreak was at its peak in China, a spokesperson for China's Foreign Ministry blasted the United States for its response to the crisis there. "The U.S. government hasn't provided any substantive assistance to us, but it was the first to evacuate personnel from its consulate in Wuhan, the first to suggest partial withdrawal of its embassy staff, and the first to impose a travel ban on Chinese travelers," the spokesperson charged. "What it has done could only create and spread fear."93 Days later, Secretary of State Michael R. Pompeo announced the United States would make available up to $100 million in existing funds "to assist China and other impacted countries," and that the State Department had facilitated the delivery to China of 17.8 tons of personal protection equipment and medical supplies donated by the private sector.94
As COVID-19 transmission accelerated in the United States, the Trump Administration stepped up criticism of China's early response to the outbreak. Secretary Pompeo told an interviewer on March 24, "unfortunately, the Chinese Communist Party covered this up and delayed its response in a way that has truly put thousands of lives at risk."95 Spokespeople for the State Department and China's Foreign Ministry have traded COVID-19-related accusations on Twitter. On March 12, a Chinese spokesperson tweeted, "It might be US army who brought the epidemic to Wuhan."96 Secretary Pompeo accused China of waging a disinformation campaign "designed to shift responsibility," and President Trump for several days referred to COVID-19 as "the Chinese virus."97 That nomenclature has drawn criticism from Asian-American groups, who argue that such language is stigmatizing.98 With a March 27 phone call, the U.S. and Chinese Presidents appeared to seek a truce of sorts. President Trump tweeted, "China has been through much & has developed a strong understanding of the Virus. We are working closely together. Much respect!"99 On the same day, the coordinator of the State Department's Global Engagement Center credited Chinese officials for recent "messaging refinement away from disinformation" related to the pandemic on social media.100 On April 8, Secretary Pompeo stated, "we're all about finding cooperation and places to move forward, but it requires truthful, candid information and sharing of data sets so that the professionals can get their arms around this virus." China, he implied, has not provided such information.101
As COVID-19 transmission in China continues to slow, China's government is making high-profile donations and deliveries of medical equipment (such as personal protective equipment, ventilators, and COVID-19 test kits) around the world, as well as supplying loans and medical teams to dozens of countries.102 President Trump has stated that he welcomes the role China is playing. "I view that as a positive, if they're helping other countries," he said on April 1, adding, "I would love China and other countries, if they have additional supplies, medical supplies, to give to other countries."103 Two critics of the Trump Administration's approach warn, "Beijing understands that if it is seen as leading, and Washington is seen as unable or unwilling to do so, this perception could fundamentally alter the United States' position in global politics and the contest for leadership in the twenty-first century."104 Several Members of Congress have introduced legislation criticizing China's response to the COVID-19 pandemic (see the Appendix).
What are the implications in Southeast Asia?105
Southeast Asia was one of the first regions to experience COVID-19 infections and the outbreak could have broad social, political, and economic implications in the months ahead. The region's countries are deeply tied together through trade and the movement of labor, links that could be reshaped if the outbreak leads to broad policy changes. As an example, Malaysia banned overseas travel on March 18, affecting approximately 300,000 Malaysians who work in neighboring Singapore, before changing tack and allowing individuals to travel to Singapore if they remain there until the end of May. Other regional issues include the following:
- Indonesia appears to be experiencing a widening outbreak, and may have a significantly larger COVID-19 case count than its public health system is able to detect.106
- The new Prime Minister of Malaysia, Muhyiddin Yassin, already faces legitimacy questions because he was not elected, and may now face greater criticism as the country's COVID-outbreak grows.107
- Burma and Laos have reported only a handful of COVID-19 cases, highlighting questions about transparency in the region's poorest nations, which may be particularly vulnerable given their underdeveloped health systems.
Much of the Southeast Asian diplomatic calendar, which drives regional cooperation on a wide range of issues including trade and public health, has been cancelled or has moved to virtual meetings. Plans by the Trump Administration to host leaders from the 10 members of the Association of Southeast Asian Nations (ASEAN) in Las Vegas on March 15 were cancelled, and Vietnam postponed the ASEAN Leaders Meeting, originally scheduled for April 6-9 until late June. The International Institute for Strategic Studies (IISS) has cancelled this year's iteration of its annual Shangri-la Dialogue, slated for June 5-7, after consultations with the government of Singapore.108
What are the implications in Central Asia?109
In Central Asia, the economic impacts of the pandemic may affect the roles of Russia and China in the region. Given disruptions to trade and cross-border movement, the pandemic could reverse recent progress on regional connectivity, a U.S. policy priority in Central Asia. The COVID-19 pandemic is placing significant economic pressure on Central Asian countries both directly, due to economic disruptions in China and Russia, and indirectly, through the fall in hydrocarbon prices. China has cut the volume of natural gas imports from Central Asia due to falling demand, and analysts speculate that Chinese investment in the region may also shrink. Turkmenistan sends almost all of its gas exports to China and is particularly vulnerable, as the Turkmen government uses gas exports to service billions of dollars of Chinese loans. The economic impact of the pandemic will likely interrupt the flow of remittances from Russia, where millions of Kyrgyz, Tajik, and Uzbek citizens work as labor migrants, accounting for significant percentages of their countries' GDPs.110
Some measures implemented to combat the spread of COVID-19 could provide governments in the region with the means to suppress political and media freedoms. The states of emergency currently in effect in Kazakhstan, the Kyrgyz Republic, and Uzbekistan grant authorities a range of powers, including the ability to suspend telecommunications networks and seize control of media outlets as well as radio and television equipment. In Kazakhstan and the Kyrgyz Republic, authorities may also suspend the activities of political parties, public associations, and independent organizations.111
What are the implications in South Asia?112
The seven countries of South Asia are home to about 1.8 billion people, nearly one-quarter of the world's population. In most South Asian countries, per capita spending on health care is relatively low and medical resources and capacities are limited.113 Dense populations and lack of hygiene are facilitating factors for pandemics, and with medical equipment needed to address the crisis in short supply, South Asia nations are likely to face serious risk.114
The COVID-19 crisis has led to more acute questioning of the political leadership in India, where since last year Prime Minister Narendra Modi has faced mass protests over new citizenship laws and persecution of Muslims; and in Pakistan, where Prime Minister Imran Khan was already dealing with widespread disaffection related to his government's performance and legitimacy. The COVID-19 crisis is likely to put a broad hold on activities related to U.S.-India and regional multilateral security cooperation, as well as delay sensitive negotiations on U.S.-India trade disputes. Moreover, with India and Pakistan still engaged in a deep-rooted militarized rivalry, any generalized South Asian crisis, especially in the disputed region of Kashmir, could lead to societal breakdowns and/or open interstate conflict between these two nuclear-armed countries.
India is the world's leading manufacturer of hydrocholoquine, an anti-malarial drug President Trump has touted as a potential treatment for COVID-19. In early April the U.S. President suggested that the United States might retaliate against India if New Delhi bans export of the drug and fails to fulfill an existing large-scale U.S. purchase order. India has agreed to allow limited exports.115
In Bangladesh, over one million displaced Rohingya reside in overcrowded and unsanitary camps along Bangladesh's border with Burma. Of these Rohingya, approximately 630,000 live in the Kutupalong camp, which may be the world's largest refugee camp. The population density in the camps—104,000 people per square mile in Kutupalong—poses challenges for social distancing, quarantine, and isolation. Any COVID-19 transmission in the camps would likely quickly overwhelm medical facilities and services, and because of the camps' porous perimeters, risk spreading into neighboring Bangladeshi towns and villages.116
What are the implications for U.S. withdrawal from Afghanistan?117
The presence and spread of COVID-19 in Afghanistan is adding new confusion to the Afghan peace process, already complicated by an extended political crisis in Kabul. The February 29, 2020 agreement signed by U.S. and Taliban negotiators commits the United States to withdraw about 3,500 of the 12,000 troops it has in Afghanistan by mid-June 2020 (with commensurate drawdowns of international forces). The United States announced on March 18, however, that it is pausing the movement of personnel into and out of theater due to concerns about COVID-19, leading some to question whether withdrawal plans will take place as envisioned by the agreement.118 The U.S.-Taliban agreement also called for negotiations between the Taliban and Afghan government representatives to begin by March 10, but thus far no formal negotiations have taken place or been scheduled.
Further spread of COVID-19 in Afghanistan could cause additional disruptions to the nascent peace process, or could present opportunities for compromise and intra-Afghan cooperation. For example, Afghan government representatives have expressed support for Taliban efforts to combat the virus in areas they control.119 Additionally, while the Taliban have reportedly targeted health workers in the past, a Taliban spokesman announced that the group "assures all international health organizations and WHO of its readiness to cooperate and coordinate with them in combatting" COVID-19.120 Afghanistan may be at particularly high risk of a widespread outbreak, due in part to its weak public health infrastructure and its porous border with Iran, where up to three million Afghan refugees live. Over 150,000 Afghans have reportedly returned from Iran in March alone.121
What COVID-19 containment lessons could be learned from Asia?
Asian governments outside mainland China were the first to deal with COVID-19. Four jurisdictions, in particular, have received wide praise for their COVID-19 control approaches: Taiwan, Hong Kong, Singapore, and South Korea. All have drawn on experiences in addressing previous public health emergencies, including outbreaks caused by SARS, swine and avian flu, and MERS. Those experiences fostered bureaucratic and public attentiveness to public health challenges and prompted governments to develop active protocols for screening, testing, isolating infected individuals, and tracing their contacts. Prior experience may also have conditioned people in those places to follow standard infection control measures (frequent hand-washing, mask-wearing, and social distancing) and to more readily accept quarantines and movement restrictions.
Taiwan.122 Taiwan (which officially calls itself the Republic of China, or ROC), is located just 81 miles off the coast of mainland China. On December 31, the same day China notified the WHO China Office of pneumonia cases of unknown origin, Taiwan officials had begun to board planes arriving from Wuhan to evaluate passengers who had fever or pneumonia symptoms.123 Travel alerts, routine passenger screenings, and directives to self-quarantine soon followed, and by early February, Taiwan barred residents of mainland China from entry.124 On January 20, Taiwan both confirmed its first COVID-19 case and activated a Central Epidemic Command Center (CECC) to lead and coordinate the government's response to the COVID-19 crisis.125 The CECC is part of the National Health Command Center (NHCC), a 24/7 central command headquarters created in 2004 following SARS.126 The government also integrated its national health insurance, customs, and immigration databases to facilitate case identification and tracking.127 The concentration of public health expertise among Taiwan's top leaders likely contributed to the government's attentive response. Taiwan's vice president, vice president-elect, vice premier, and minister of health are all public health experts.128
The government has also issued strict and transparent guidance to contain the spread of the virus, which its citizens largely appear to have followed. Taiwan has tested widely for the virus, including mandatory tests for certain groups and tests for patients with respiratory illnesses that tested negative for the flu.129 Directives to conduct "self-health management" or self-quarantine have been enforced by harnessing cellphone location data and punishing violators with steep fines.130 The government's daily press conferences and frequent broadcasts of public service announcements have heightened public awareness and facilitated compliance with best practices.131 Taiwan also created informational apps, to help citizens track the spread of the virus and locate supplies of masks.132 In February and March, the government announced economic relief and stabilization measures, including approximately USD$2 billion to assist Taiwan industries affected by the outbreak, and payments totaling $465 to individuals who were quarantined or providing care for the quarantined.133
Hong Kong.134 Initially, the government of Hong Kong, a Special Administrative Region (HKSAR) of the People's Republic of China, resisted taking aggressive measures to prevent a COVID-19 outbreak. Public criticism of what many considered an insufficient and inconsistent initial response appears to have contributed to the government's subsequent decision to act. A newly formed union of doctors and nurses working for the Hong Kong Hospital Authority held a strike on February 3, 2020, demanding the HKSAR government close the city's border with mainland China, for example.135 The HKSAR government closed all but two of the land crossings with mainland China the next day. The government implemented a mandatory 14-day quarantine for all arrivals to Hong Kong on March 17, 2020.136 Recent, more aggressive government measures to contain the spread of COVID-19 include closing Hong Kong's borders to all non-resident arrivals (except from Macau and Taiwan) as of March 25, 2020.137 The government has also developed an extensive range of public service announcements, webpages, and other modes of informing the public about COVID-19.138
Although the HKSAR government may have hesitated, Hong Kong's public quickly adopted social distancing and anti-contamination behaviors developed during previous viral outbreaks. Similarly, medical professionals quickly implemented anti-viral protocols.139 Many businesses acted on their own initiative to adopt measures to reduce the risk of exposure, including facilitating telework, taking people's temperature when they entered buildings, and refusing entry to anyone with a fever.
Singapore.140 Singapore, a Southeast Asian city-state of 5.7 million people, was one of the first nations outside China to report COVID-19 cases, with its first infection reported on January 23. Public health experts have praised Singapore's rapid early actions, including extensive monitoring of cases and their contacts, temperature checks at building entrances, and clear public messaging. Singapore has experienced a significant "second wave" of cases after initial success at curbing the spread, however, leading authorities to close schools and most businesses, steps that they had avoided earlier.141 Singapore's approach continues to evolve and become more restrictive, including employing the armed forces to make up to 2,000 visits per day to search for carriers.142 Many of the new cases have come from crowded quarters where migrant workers live.
Singapore began screening individuals who had traveled to Hubei Province three days after China first reported the outbreak, and halted incoming flights from Wuhan on January 23, the day of Singapore's first confirmed case.143 As new cases were reported, Singapore health officials conducted detailed interviews of affected individuals, requiring those who had come into contact with them to quarantine themselves. The Health Ministry developed the capacity to test more than 2,000 individuals a day.144 Individuals who come within two meters of an infected individual or spend 30 minutes with one are required to undergo testing and to quarantine or be placed under observation. Individuals found to have misled health officials are subject to criminal penalties including fines and the threat of imprisonment.145 The Health Ministry issues daily updates on individual cases and the numbers of people under care or protective quarantine, including details of where each individual who has tested positive lives.
South Korea.146 After cases were confirmed in South Korea in late January, authorities pursued an aggressive testing regimen and public communication strategy. South Korea describes its strategy as the three "T"s: tracking, testing, and treatment. As of March 30, nearly 400,000 citizens had been tested for the virus—the highest rate of testing per capita in the world—at over 600 sites, including pop-up facilities and drive-through sites.147 Results are generally provided within 24 hours.148 The case fatality ratio (1.64% as of March 30) has also been low, which health officials attribute to early detection and treatment, as well as universal health care.149 As of mid-April, South Korea has been able to stabilize the outbreak without lockdowns or wholesale travel bans, in part, experts argue, by being transparent and disseminating information about the virus' spread, including possible infections at the neighborhood level. President Moon Jae-in has stepped aside to allow national health officials to take the lead in delivering twice-daily messages to the public. After MERS killed 38 people in 2015, South Korea reformed its health policy by granting the government greater powers to monitor and track individual patients and to allow private companies to rapidly produce tests. Shortly after the COVID-19 outbreak hit, authorities were able to test 10,000 patients daily.150 By the end of March, authorities were testing over 20,000 patients per day.151
Europe152
How are European governments and the European Union (EU) responding?
On March 13, 2020, WHO officials described Europe as the new global epicenter of the COVID-19 pandemic, noting that more cases were being reported each day in Europe than were reported in China at the height of its epidemic.153 Italy has been hit hardest thus far, having become on March 19 the country with the world's highest COVID-19 death toll at that time. Infections have been rising elsewhere on the continent as well. As of April 16, more than 800,000 infections and nearly 90,000 deaths had been reported across the EU and United Kingdom.154 Although fewer than elsewhere in Europe, Ukraine, Russia, and other parts of the former Soviet Union also report a growing number of new COVID-19 cases.
European leaders have characterized the pandemic as Europe's biggest challenge since the Second World War, with potentially severe economic consequences and far-reaching social and political implications beyond the public health impact.155 European governments and the 27-member European Union (EU) are enacting an array of policy responses. Authorities in most European countries have imposed limitations on the movement of people and are undertaking significant fiscal and monetary measures. Key measures taken in Europe to combat the pandemic include:
- "Lockdowns" and restrictions on medical equipment exports. On March 9, Italy became the first country to impose a nationwide quarantine, prohibiting "non-essential" movement within the country and closing all non-essential businesses; France, Germany, the United Kingdom (UK), and others followed with similar restrictions. Almost all European countries closed schools and some types of businesses and have restricted public gatherings to varying degrees. Numerous European governments mobilized their military forces to assist response efforts, including constructing makeshift hospitals. In some countries, government authorities scaled back public transportation and introduced curfews. In mid-April, some European countries began announcing plans for a gradual re-opening of their societies and economies in the coming months, but leaders in these countries cautioned that measures would be contingent on a clear reduction in infection rates.
On March 15, the EU restricted the export of some protective medical equipment outside the bloc to preserve stocks and encourage the sharing of such supplies with member states facing shortfalls, such as Italy.156 Some governments, including France and Germany, initially faced criticism for imposing national restrictions on medical supply exports.
- Economic stimulus. Many analysts predict that the COVID-19 pandemic could cause a financial crisis in Europe that might be several times worse than the 2008 global recession. European governments and the EU have announced an array of measures to mitigate a severe economic downturn. Measures include loan programs and credit guarantees for companies, income subsidies for affected workers, tax deferrals, and debt repayment deferments. Italian officials estimate COVID-19 responses could cost the government €25 billion ($27 billion). In France, President Emmanuel Macron has pledged to provide unlimited budgetary support to companies and workers, which the government says could cost upward of €45 billion ($48 billion). Germany has announced a €500 billion ($536 billion) loan program and income support measures.157 Other countries have announced similar relief measures.
On March 18, the European Central Bank, which manages the EU's common currency (the euro), announced a Pandemic Emergency Purchase Program (PEPP) of about €750 billion ($803 billion) aimed at calming markets and stemming a debt crisis in the Eurozone (the 19 EU member states that use the euro as their currency).158 On April 9, Eurozone leaders agreed to a new financial assistance package for member states of at least €540 billion (roughly $590 billion). This package includes access to credit lines through the European Stability Mechanism (ESM, the Eurozone's "bail-out" fund) worth approximately €240 billion ($261 billion) for health-related costs, establishment of a European Investment Bank fund to back up to €200 billion ($219 billion) in loans for businesses, and a €100 billion ($110 billion) unemployment benefit support plan. Reaching consensus on this financial package was contentious and exposed divisions among EU member states. The package does not include establishing common EU debt instruments (or "corona bonds")—one of the most controversial proposals supported by hardest-hit countries such as Italy, Spain, and France—but EU leaders will likely continue to discuss this option and other potential economic measures.159
- Border closures. Numerous European governments have enacted national border controls and some have restricted entry only to national citizens. These measures have complicated efforts to maintain the free movement of goods, services, and people (key elements of the EU's single market) on which the EU's highly integrated economy depends. National border controls and closures within the EU's internal border-free Schengen Area160—in which individuals may travel without passport checks among 22 EU member states and four non-EU countries—resulted in long delays at several borders. On March 16, 2020, the EU implemented a temporary ban on "non-essential travel" into the Schengen Area for non-residents from outside countries (including the United States), partly in an effort to preserve freedom of movement within the EU. Many analysts contend that the disparate national reactions to the COVID-19 pandemic are endangering the EU's single market and Schengen system, with possible long-term implications for the EU's future.161
How is the pandemic affecting U.S.-European relations?
Managing the spread of COVID-19 has added new tensions to already strained U.S.-European relations. The EU—a frequent target of criticism from President Trump—expressed dismay with the announcement from the Trump Administration on March 11, 2020 of a travel ban on foreign nationals arriving in the United States from the Schengen Area. In a joint statement on March 12, EU leaders noted that COVID-19 was a global crisis that "requires cooperation rather than unilateral action" and expressed disapproval that the U.S. travel ban was imposed "without consultation."162 U.S. officials countered that the travel ban decision had to be taken quickly and was based on the WHO's assessment of sustained transmission in the Schengen Area.163 The Trump Administration subsequently extended the travel ban beyond the Schengen Area to the UK and Ireland. Nevertheless, some analysts on both sides of the Atlantic asserted that the U.S. travel ban was scapegoating the EU, threatened future U.S.-EU relations, and imperiled broader U.S.-European political and security alliances. Some critics have also bemoaned the lack of coordinated U.S.-European leadership in mobilizing a global response to control the pandemic and address its wider societal and economic consequences.164
Africa165
How are African governments responding?
Nearly all countries in sub-Saharan Africa had confirmed COVID-19-cases as of April 7, 2020, and 12 had more than 100 cases. South Africa had the most, with nearly 1,700. Most early cases in the region were detected through screening of international air passengers, which many African governments began carrying out in early 2020. Most early identified cases were detected among travelers arriving from Europe. Several countries have reported chains of infection tied to initial imported cases, but a growing number of infections are of unknown origin, suggesting that local community transmission is occurring in some countries.166
The foreign origin of most initial COVID-19 cases has spurred a growing number of African governments to suspend several international links, including with China.167 Some also banned the entry of visitors from other high prevalence countries.168 Prevention and mitigation strategies vary considerably across the region. Some countries, for instance, have banned large gatherings, (e.g., religious, political, sporting, and/or cultural events), closed schools and universities, and encouraged work from home where feasible. Others have declared national disasters and/or national emergencies.169 In addition to increasing COVID-19 testing capacity (see below) and providing for the isolation of infected persons and potential cases, most African governments have launched public outreach campaigns centered on personal hygiene (e.g., handwashing) and social/physical distancing.
Some African countries are leveraging community health networks to detect and prevent the spread of COVID-19 in rural areas, in some cases based on lessons learned in responding to past Ebola virus outbreaks.170 African health systems overall, however, have very low capacity to prepare for and respond to COVID-19, and governments have few domestic tools to address the economic fallout. As in other developing regions, many people live in close quarters and lack access to clean water or adequate sanitation facilities. In some countries, mistrust of government authorities (rooted in part in political differences, corruption, health system inefficacies, and traditional beliefs) may spur noncompliance with official public health recommendations, as was the case during the Ebola outbreak. The pandemic may also have an impact on political conditions in Africa, as authoritarian-leaning governments wield emergency powers to break up protests and limit opposition activism.171 Many of the region's heads of state are over 70 years old, placing them in a high risk profile for COVID-19. In Burkina Faso, at least four cabinet members have tested positive for the disease.
Experts have expressed concern that the full extent of the pandemic's impact on public health and economies could be devastating in Africa, where many countries rely on tourism and/or commodity exports, notably to China.172 Both have declined sharply due to COVID-19-linked interruptions and declines in world economic activity, trade, and travel. Africa's heavy reliance on imports of consumer and industrial goods from China may also suffer, alongside business sectors tied to these imports (e.g., digital technology activity and local retail). African airlines are also suffering steep losses. Natural resource-linked exports, which comprise roughly 75% of African exports by value, may be particularly hard-hit as foreign industrial demand declines. Africa's many oil export-dependent countries may face a double threat: a concurrent oil price collapse linked to a Saudi-Russian oil price war and a projected global COVID-19-linked slump in global oil demand. Multiple central banks have acted to increase economy-wide liquidity and many governments are planning substantial resource reallocations or are slated to receive international assistance to finance COVID-19 responses.173
How is the Africa CDC responding?
The WHO and the African Union (AU) Africa Centres for Disease Control and Prevention (Africa CDC) are partnering with African governments to enhance the capacity of public health systems in the region to detect and respond to COVID-19.174 Their support centers on training personnel on disease detection and surveillance at laboratories and ports of entry, providing COVID-19 test kits and other health commodities (e.g., personal protection equipment or PPE), and other health response capacity-building. The Africa CDC has provided COVID-19 detection training in 40 countries, most of which are now able to independently test for the disease. These labs are supported by a regional COVID-19 specimen referral and verification system comprising expert labs in Senegal and South Africa, with ten more planned region-wide. The Africa CDC has created a regional COVID-19 task force to facilitate priority COVID-19 control measures and activated its Emergency Operations Center and Incident Management System to aid intra-AU COVID-19 information sharing.175 The Africa CDC also is training epidemiologists in disease event tracking and risk analysis, at its headquarters and regionally,176 and is providing COVID-19 medical and technical advice and pandemic briefings to AU member states.177 Senegal's Institute Pasteur, an African CDC reference lab, has partnered with Mologic, a British biotech firm, to produce a rapid mobile COVID-19 test that it plans to produce within months.178
Middle East and North Africa179
How are Middle Eastern and North African governments responding?
As of April 9, WHO announced that countries in the "Eastern Mediterranean Region," or EMR (which includes some but not all countries in the Middle East, North and East Africa, and Central Asia),180 had reported 87,882 confirmed COVID-19 cases spanning 20 countries and the Palestinian territories.181 Unofficial estimates are considerably higher.
- Iran has been the epicenter of the crisis within the region, reporting more than 66,220 confirmed cases as of April 9.182 U.S. officials are "deeply concerned" that Iran may be covering up data relating to the spread of the virus.183
- Egypt is in the early stages of what could become a nationwide outbreak. Officially, the government has reported 1,560 cases as of April 9, but foreign reporters noted that a Canadian study estimated that Egypt had roughly 19,000 cases as of mid-March.184
Government responses to the crisis have varied. On March 18, WHO Regional Director for EMR stated, "Frankly, we are seeing uneven approaches across the region. While we have observed impressive progress in several countries, not all are yet applying the whole-of-government and whole-of-society approach that are absolutely needed to effectively prepare and respond."185 Many countries have suspended international and/or domestic passenger flights, closed land and sea crossings with neighboring states, imposed curfews, and closed commercial, educational, and religious sites. In Jordan, the King invoked a war-time defense law and ordered the army to deploy and establish checkpoints around the capital Amman. In Algeria, the government of recently elected President Abdelmadjid Tebboune announced a ban on protest rallies, which have been held weekly for political reforms since February 2019. In Israel, the government approved temporary emergency regulations for security officials to monitor COVID-19 patients and potential victims via their mobile phones.
WHO has stated that the EMR region has among the worst health indicators in the world, noting, "There is armed conflict in 12 of the region's 22 countries. The region's 680 million people represent 9% of the global population, yet the EMR is home to 43% of those who need humanitarian assistance and is the source of 64% of the world's refugees."186 Several countries in the region have weak water and energy infrastructure, underinvestment in hospitals, internal displacement, and overcrowding in urban areas, leaving them vulnerable to potentially severe effects. In Syria, which has undergone 10 years of civil conflict, a significant portion of the country's healthcare infrastructure has been damaged or destroyed. In Lebanon, an economic crisis that escalated in late 2019 has severely limited the government's ability to import food, fuel, and medicine. In Yemen, where conflict has contributed to what officials already have called the worst humanitarian crisis in the world, health care capacity is severely limited.
As in other regions, government efforts to contain the spread of the virus have required the suspension of most public commerce and trade, resulting in a severe blow to economic activity that is expected to generate increased unemployment. The tourism and hospitality industries, which employ a large share of people in the region, have been significantly affected by travel restrictions. Rising unemployment, particularly concentrated among the youth, could have implications for political stability in the region. A prolonged global economic slowdown associated with COVID-19 also could dampen global demand for oil and natural gas resources exported from countries in the Middle East with corresponding diminishing effects on export revenues and the fiscal health of some regional governments.
- The Gaza Strip. The Hamas-controlled Gaza Strip has reported 13 COVID-19 cases as of April 9, and officials from international organizations have voiced concerns about a possible outbreak given the acute humanitarian challenges in Gaza. The densely populated territory of nearly 2 million Palestinians has a weak health infrastructure and many other challenges related to sanitation and hygiene.187 On March 17, the U.N. Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) launched an emergency flash appeal for $14 million to prepare and respond to COVID-19-related needs for Palestinian refugees in Gaza, the West Bank, Jordan, Lebanon, and Syria through May 2020. The Trump Administration stopped U.S. contributions to UNRWA in 2018 and all bilateral aid to the West Bank and Gaza in 2019.188 For FY2020, Congress appropriated $75 million from the Economic Support Fund for humanitarian and development purposes in the West Bank and Gaza.
- Syria. Approximately 6.2 million Syrians remain internally displaced, with many living in overcrowded IDP camps or informal settlements where they are unable to access clean water, sanitation, or medical care. In northwest Syria, nearly one million people were internally displaced between December 2019 and February 2020, and more than 70 health facilities ceased to function. Conditions are also dire at Al Hol IDP camp in northeast Syria, which houses nearly 70,000 family members of captured Islamic State fighters, 96 percent of whom are women and children.189 According to the Kurdish Red Crescent, at least 517 people, mostly children, died inside the Al Hol camp in 2019, due to malnutrition, inadequate healthcare for newborns, and hypothermia.190
- The Hajj (Saudi Arabia). Each year, millions of Muslims travel to Saudi Arabia for a religious pilgrimage to Mecca. This journey, known as the Hajj, is a pillar of the Islamic faith. Saudi authorities have invested considerable attention and resources to averting infectious disease outbreaks during the Hajj, having faced 2009 HIN1 Pandemic, SARS, and MERS. In February 2020, Saudi leaders suspended umrah pilgrimage visits to the kingdom (which can be done at any time of year in contrast to the Hajj) and limited access to holy sites in Mecca and Medina. It remains to be seen whether the Hajj pilgrimage will go forward as scheduled in August 2020.
- U.S. Military Facilities. The United States maintains a significant military presence in the region, and has partnered closely with local forces. U.S. forces remain in Iraq and are consolidating base locations. U.S. training has been suspended due to COVID-19 risks, and U.S. officials say future training will use "fewer bases with fewer people."191
What are the implications for U.S.-Iran policy?
The spread of COVID-19 in Iran has raised questions about the possible effects of U.S. sanctions on Iran's response capacity.192 The Trump Administration has articulated a policy of "maximum pressure" on Iran, which imposes economic sanctions on every sector of Iran's economy. Iranian officials and some global health officials assert that the U.S. sanctions are weakening Iran's ability to contain the virus by reducing the availability of medical equipment.193 Sales to Iran of humanitarian items, including medicine and medical equipment, are generally exempt from U.S. sanctions. The reluctance of banks worldwide, however, to finance any transactions involving Iran, fearing penalties by the United States for sanctions violations, has reportedly affected Iran's ability to import all types of goods, including those that are exempt from sanctions. The United States has offered Iran an unspecified amount of assistance through WHO to help it deal with the outbreak, which the government has reportedly refused. In early March 2020, U.S. officials issued guidance indicating that transactions involving Iran's foreign exchange assets held abroad, when used to buy humanitarian items, would not face U.S. sanctions.194 Iran has requested a $5 billion loan from the International Monetary Fund (IMF) that Iran says it needs to cope with the COVID-19 crisis. Administration officials have reportedly told journalists that the United States plans to work with its allies to deny the loan, asserting that Iran will likely use the funds for its regional activities such as supporting armed factions in various countries, rather than on medical equipment.195 Yet, some Members of Congress have called on the Administration to relax sanctions on Iran, at least for a temporary period, to help Iran deal with the COVID-19 pandemic.196
Canada, Latin America, and the Caribbean197
How is the Canadian government responding?
Canada's federal, provincial, and territorial governments have taken a variety of steps to respond to the COVID-19 pandemic. To slow the spread of the virus, each provincial and territorial government has implemented social distancing measures, though restrictions vary by location. Prime Minister Justin Trudeau also announced on March 11, 2020, the establishment of a C$1.0 billion ($715 million) fund to prepare for and mitigate the effects of COVID-19. The federal government provided half of the funds directly to provinces and territories to enhance testing and surveillance, and purchase additional medical equipment. It allocated the remainder to the research and development of vaccines and antiviral treatments, acquisition of personal protective equipment, and other federal health measures.198
Additionally, the Canadian government has begun to respond to the economic impact of the pandemic. The Trudeau government has announced an assistance package worth C$105 billion ($75 billion), equivalent to about 5% of Canada's gross domestic product, to provide direct support to Canadian individuals and businesses. The Canadian Parliament has approved several of the measures, including a new Canada Emergency Response Benefit that is to provide C$2,000 ($1,430) per month for up to four months for workers who lose their incomes due to COVID-19. The Parliament also approved a new Canada Emergency Wage Subsidy that is to help employers cover 75% of employees' wages, up to C$847 ($610) per week, for up to 12 weeks.199 In addition, the Bank of Canada cut its benchmark interest rate from 1.75% to 0.25%, and launched its first-ever quantitative easing program to purchase government and commercial debt.200
Provincial health services, which administer the Canadian health system, have reported shortages of and intense competition for needed supplies.201 The federal government worked with the Trump Administration to close the U.S.-Canada border to all non-essential travel. Although both the Canadian and U.S. governments initially prioritized keeping their border open to trade, Canadian officials are concerned that export restrictions in the United States could exacerbate shortages of medical supplies and personnel.202 Canadian officials have warned the United States against interrupting the flow of essential goods and services, noting that Canadian medical professionals and supplies cross the border daily.203
How are Latin American and Caribbean governments responding?
The ability of countries in Latin American and the Caribbean to mitigate a COVID-19 outbreak varies across the region. The pandemic appears to have arrived in Latin American and the Caribbean later than many other regions and has yet to peak. A 2019 Global Health Security Index included Brazil, Argentina, Chile, and Mexico among countries most prepared for a pandemic, and considered Venezuela, Honduras, Jamaica, the Bahamas, Haiti, Guyana, Belize, and Guatemala to be among the least prepared.204 Although all countries in the region have identified universal health coverage as a priority, many lack sufficient doctors, hospitals, medical supplies and other infrastructure, and are overlaid with challenges of inequality and economic fragility.205 As the most urbanized region in the world (with approximately 80% of the region's 650 million people concentrated in urban areas), several countries in Latin American and the Caribbean face challenges in treating COVID-19 cases, and enforcing social distancing by quarantine and curfew.206 In some cities, such as Guayaquil, Ecuador, outbreaks have already overwhelmed medical systems.207In rural areas, access to clean water and treated sewage is limited, and meager health infrastructure poses additional challenges. Indigenous communities, Afro-descendants, and other marginalized populations often face additional barriers to healthcare.
Political conditions could further hinder the region's pandemic response. Venezuela is of particular concern since protracted political and economic crises had already weakened the health system. An estimated 4.8 million Venezuelans have fled the country, and recent immigration controls implemented by neighboring countries are unlikely to stop many more Venezuelans from crossing the region's porous borders. The presidents of Brazil and Mexico, downplayed the COVID-19 pandemic, delaying a coordinated and timely response and raising concerns that individuals might ignore public health advice.208 On the other hand, leaders who have taken more sweeping control measures frequently have been applauded.
Many governments have taken extraordinary measures to respond to the pandemic, including delaying elections. Chile was scheduled to hold a referendum on drafting a new constitution that has been delayed until October, and Bolivia was scheduled to hold a new presidential election on May 3 that was postposed without a fixed new date for the vote.209 Analysts warn that election delays and other emergency measures could be used to curb civil liberties and allow for abuses of power and corruption.
International Economic and Supply Chain Issues210
What are the implications of the pandemic in China's economy?
COVID-19 emerged amidst an economic downturn in China with officials negotiating U.S.-China bilateral tariffs, working to curb consumer inflation (due in part to domestic pork shortages resulting from African swine fever) and moving to rein in government spending and shadow lending. COVID-19 containment measures significantly slowed economic activity in China, and halted production almost entirely in some areas of the country, particularly Hubei province.211 In early February, China's central bank pumped $57 billion into the banking system, capped banks' interest rates on loans for major firms, and extended deadlines for banks to curb shadow lending. China's central bank is seeking to stabilize China's currency and shore up liquidity in China's banking system, which remains the primary channel through which the government is providing business relief. 212 Despite these measures, China has experienced a contraction in GDP growth in its first quarter, the first contraction since 1992.213
Many firms in China are still struggling to return to full capacity as some restrictions on travel and distribution of goods and workers remain.214 Some Chinese firms are facing reduced domestic and global demand for goods and services. U.S. companies in the technology and auto sectors might be affected significantly, as exports of intermediate inputs (e.g., auto parts, microelectronics) from China continue to be delayed. Service sectors exposed to China's tourism might also be significantly impacted by ongoing travel restrictions and a slump in Chinese demand.215 Economic constraints raise questions about the capacity of the United States and China to implement the Phase One Trade Agreement signed in January 2020, which commits China to purchasing $200 billion in additional exports over the next two years.216
How is COVID-19 affecting the global economy and financial markets?
The COVID-19 pandemic is having a noticeable impact on global economic growth.217 The pandemic is affecting a broad swath of international economic and trade activities, from tourism, medical supplies and other global value chains, consumer electronics, and financial markets to energy, food, and a range of social activities. The economic situation, however, remains highly fluid. Labeling the projected decline in global economic activity as the Great Lockdown, the IMF forecasted on April 14, 2020 that the global economy could decline by 3.0% in 2020, before growing by 5.8% in 2021, constituting the "worst recession since the Great Depression, surpassing that seen during the global financial crisis a decade ago."218 The U.S. economy is projected to contract by 5.9%, about twice the rate of decline experienced in 2009 during the financial crisis. The forecast assumes that the pandemic fades in the second half of 2020 and that the containment measures can be reversed. The IMF also argues that recovery of the global economy could be weaker than projected as a result of: lingering uncertainty about possible contagion, lack of confidence, and permanent closure of businesses and shifts in the behavior of firms and households.219
Global trade, measured by trade volumes, slowed in the last quarter of 2019 and was expected to decline further in 2020, as a result of weaker global economic activity associated with the pandemic. As of March 2, the Organization for Economic Cooperation and Development (OECD) projected a 0.5% reduction in global economic growth, from 2.9% to 2.4%, if the economic effects of COVID-19 peaked in the first quarter of 2020.220 If the effects of the virus extended into the second quarter, OECD estimated a more sluggish economic growth rate of 1.5%. The OECD also estimates that increased direct and indirect economic costs through global supply chains, reduced demand for goods and services, and declines in tourism and business travel mean that, "the adverse consequences of these developments for other countries (non-OECD) are significant."221
Uncertainty about the length and depth of pandemic-related economic effects and the effectiveness of pandemic control measures are shaping perceptions of risk and volatility in financial markets and corporations. Financial markets worldwide, particularly in the United States, Asia, and Europe, are volatile as investors are concerned that the virus is creating a global crisis that could be prolonged and expansive.222 Similar to the 2008-2009 global financial crisis, central banks are rapidly becoming the lender of last resort and are attempting to address financial market volatility. Developments continue to evolve rapidly and the market dynamics have led some observers to question if these events mark the beginning of a full-scale global financial crisis.223
Financial market dislocation can potentially increase liquidity constraints and credit market tightening, as firms hoard cash, with negative effects on economic growth. In some financial markets, fund managers have started selling government securities to increase their cash reserves, pushing down government bond prices. Financial markets are also responding to increased government bond issuances in the United States and Europe to fund COVID-19-related spending, further increasing government debt.
How are policymakers responding to the economic crisis?
The challenge for policymakers is to implement targeted policies that address what are expected to be short-term problems without creating distortions in economies that can outlast the impact of the virus itself. Policymakers are being overwhelmed by the quickly changing nature of the global health crisis, which appears to be turning into a global trade and economic crisis whose potential effects on the global economy are rapidly growing. In addition, many policymakers are constrained in their response to the crisis, with limited flexibility for monetary and fiscal support, given the broad-based synchronized slowdown in global economic growth, especially in manufacturing and trade, which was occurring prior to the viral outbreak. In their policy response, many governments are taking unilateral measures, particularly in closing borders and imposing export restrictions on medical equipment. The G-7 have pledged to do "whatever is necessary" to respond to the crisis, and an emergency G-20 summit is expected to be held soon.
On March 3, 2020, a meeting of the G-7 finance ministers issued a statement claiming that the G-7 economies224 would use "all appropriate policy tools" to sustain economic growth.225 Since that statement, the European Central Bank and the Bank of Japan have taken steps to expand liquidity, but both the EU and Japan already have low interest rates, potentially limiting the effectiveness of any further monetary policy responses.226 On March 10, Italy announced €10 billion ($28 billion) in stimulus measures to cushion the economic impact of the nationwide lockdown.227
How will China's production slowdowns affect U.S. supply chains?
COVID-19 has revealed U.S. and global supply chain vulnerabilities across a range of sectors, many of which rely directly and indirectly on China-based manufacturing. During the 2002-2003 SARS outbreak, China accounted for 8% of global manufacturing exports; in 2018, China was the source of approximately 19% of global manufacturing exports, including intermediate goods vital to global manufacturing supply chains.228
The measures taken by the Chinese government to contain the COVID-19 outbreak significantly curtailed domestic and global transportation of a wide range of products and manufacturing inputs, including microelectronics, auto parts, and other intermediate inputs that ship by air.229 Production has not returned to full capacity in China, with sharp slowdowns continuing in sectors concentrated in Hubei Province, the outbreak's epicenter and an important production and transport hub for goods, including auto parts, LCD panels, and pharmaceuticals.230 Disruptions in Chinese supply chains were initially expected to have a limited, short-term macroeconomic effect on developed markets, but Chinese firms and logistics operations are struggling to return to full capacity. Some observers expect these challenges might cause shortages in a range of goods produced in China, including raw materials, intermediate industrial inputs, and consumer products. Before the pandemic, U.S.-China tariffs had prompted a number of U.S. firms with operations in China or with a heavy dependence on China to move some operations out of the country. Observers question whether companies might further diversify away from China and establish new supply chains.231
China plays a considerable role in U.S. healthcare and pharmaceutical supply chains as an exporter of both intermediate products, such as active pharmaceutical ingredients (APIs) used for producing drugs and antibiotics, as well as finished goods, including personal protective equipment (PPE) and medical devices. In early February, the Chinese government redirected all medical-related production for domestic use, centralized the production and distribution of key PPE and other medical supplies in China, and transferred related authorities from China's Ministry of Industry and Information Technology (MIIT) to the National Development and Reform Commission (NDRC), China's central economic planning agency.232 In response to government directives, firms with significant production capacity in China, including 3M, Foxconn, and General Motors, shifted significant elements of their operations to manufacturing medical PPE.233
Reduced production and export of pharmaceuticals and PPE from China is exacerbating shortages in the United States of critical medical supplies. Minnesota-based 3M, a large-scale manufacturer of N95 masks, for example, told the New York Times that all masks manufactured at its Shanghai factory were sold to meet China's domestic demand. Other mask manufacturers, such as Canada's Medicom, have also stated that the Chinese government has prohibited the export of PPE.234 A longer-term disruption of China's pharmaceutical and medical exports could increase the cost of drugs and routine medical procedures in the United States. A slowdown in API exports from China, for example, could increase cost pressures faced by U.S. drug manufacturers.235 The U.S. Food and Drug Administration (FDA) has not reported a precise volume of APIs manufactured by China,236 but estimated that China was the second largest exporter of drugs and biologics to the United States in 2018.237 Similarly, China is a leading supplier of APIs in global supply chains for painkillers, diabetes medicines, and antibiotics.
On March 6, the Office of the U.S. Trade Representative (USTR) removed tariffs on 100 health-related supplies and equipment. It remains to be seen whether this incentive will increase imports. While some analysts and industry groups have pointed to existing tariffs as an obstacle to U.S. imports of health and medical products, global supply shortages due to the sharp spike in demand and the continued nationalization of domestic supply in China appear to be stronger drivers of reduced imports of medical products in the United States.238
Issues for Congress239
The COVID-19 pandemic has raised questions about domestic and international preparedness and the appropriate responses to pandemic control. Although the United States has long-supported the delivery of PPE through its international pandemic preparedness programs, this practice has come into question while the numbers of COVID-19 cases and deaths climb in the United States. As of April 15, 2020, the United States had the highest number of COVID-19 cases and deaths worldwide, accounting for roughly 30% of all COVID-19 cases globally. In March, some Members of Congress began questioning the delivery of PPE by USAID to foreign countries while some governors and mayors reported shortages of the commodities.240
The United States provides annual funding for foreign assistance, approximately $20 billion of which is administered by USAID each year. USAID programs operate in more than 120 countries worldwide and are intended to meet specific development objectives. In many of these countries, widespread poverty, weak public institutions, and diverse pre-existing governance challenges are likely to be exacerbated by the pandemic. To preserve these investments and past policy progress, protect U.S. foreign policy interests in the region, save lives, and help combat the negative socioeconomic effects of the pandemic in the region, Congress may seek to address additional help aid recipients might request to control the pandemic and its effects.
Congress might also consider how the pandemic may affect partner governments' absorption capacities, and the manner and degree to which U.S. assistance may complement or coincide with nationally-determined pandemic responses. Congress may also wish to consider how responding to the challenges created by the pandemic may reshape pre-existing U.S. aid priorities—and how it may affect the ability of US personnel to implement and oversee programs in the field. Relatedly, Congress may wish to ensure that U.S. responses are robustly coordinated with those of other donor governments and multilateral functional agencies—and to ensure that such efforts are transparent and cost-effective, and that donor assistance is complementary and non-duplicative.
The pandemic is also having other effects on foreign affairs that Congress might consider. Some have questioned, for example, how U.S. immigration policy might impact COVID-pandemic control efforts. Some Members of Congress and officials representing Latin American and Caribbean governments have expressed concern that COVID-19-related screening procedures for deportations are not sufficient to prevent the importation of COVID-19 cases from the United States and have asked the U.S. Immigration and Customs Enforcement (ICE) to suspend deportations.241 A number of people deported from the United States to Latin America have reportedly tested positive with COVID-19 or have reportedly been exposed to someone with COVID-19. Other Members of Congress continue to support the Administration's border policies, which the Administration maintains are conducted in a manner that accounts for the dangers of COVID-19.242
Congress has also debated the extent to which the United States should contribute to multilateral organizations for COVID-19 control. Some Members, for example, are arguing for withholding contributions to the WHO, while others are urging the Administration to pay outstanding assessments to the organization and support ongoing WHO COVID-19 efforts.243
Appendix. Selected Legislation Introduced or Enacted in the 116th Congress Related to International COVID-19 Incidence or International Pandemic Preparedness244
H.R. 6504, To direct the Secretary of Health and Human Services, acting through the Director of the Centers for Disease Control and Prevention, to develop a plan to improve surveillance with respect to diseases that are viral pandemic threats, and for other purposes. Referred to the House Committee on Energy and Commerce on April 14, 2020.
H.Res. 922, Expressing the sense of the House of Representatives that all nations should permanently close live wildlife markets and that the People's Republic of China should cease spreading disinformation regarding the origins of coronavirus. Referred to the House Committee on Foreign Affairs, and in addition to the House Committees on Natural Resources, Agriculture, and Energy and Commerce on April 14, 2020.
H.R. 6500, To reduce Federal spending and fund the acquisition of unexpired personal protective equipment (including face masks) for the strategic national stockpile by terminating taxpayer financing of Presidential election campaigns. Referred to the House Committee on Ways and Means, and in addition to the Committee on House Administration, on April 14, 2020.
H.R. 6481, To rescind the appropriation made for migration and refugee assistance in the Coronavirus Aid, Relief, and Economic Security Act and redirect the funds to U.S. Customs and Border Protection and U.S. Immigration and Customs Enforcement. Referred to the House Committee on Appropriations on April 10, 2020.
H.R. 6480, To require the President, after the World Health Organization declares a global pandemic, to report to the Congress on the status of Federal planning to respond to the pandemic. Referred to the House Committee on Energy and Commerce, and in addition to the Committee on Financial Services on April 10, 2020.
H.Res. 919, Condemning the United Nations' decision to appoint China a seat on its Human Rights Council. Referred to the House Committee on Foreign Affairs on April 10, 2020.
H.R. 2166, Global Health Security Act of 2019. Directs the President to create the Global Health Security Agenda Interagency Review Council to implement the Global Health Security Agenda, an initiative launched by nearly 30 nations to address global infectious disease threats. Ordered to be reported on March 4, 2020, and introduced in the House on April 9, 2020.
H.Res. 917, Expressing the sense of the House of Representatives that the United States should withhold the contribution of Federal funds to the World Health Organization until Director-General Tedros Ghebreyesus resigns and an international commission to investigate the World Health Organization is established. Referred to the House Committee on Foreign Affairs on April 7, 2020.
H.R. 6471, To posthumously award a Congressional Gold Medal to Dr. Li Wenliang, in recognition of his efforts to save lives by drawing awareness to COVID-19 and his call for transparency in China. Referred to the House Committee on Financial Services, and in addition to the Committee on House Administration on April 7, 2020.
H.R. 6429, To establish in the Legislative Branch a National Commission on the Coronavirus Disease 2019 Pandemic in the United States. Referred to the House Subcommittee on Economic Development, Public Buildings, and Emergency Management on April 6, 2020.
H.R. 6440, To establish the National Commission on the COVID-19 Pandemic. Referred to the House Committee on Energy and Commerce on April 3, 2020.
P.L. 116-136, Coronavirus Aid, Relief, and Economic Security Act or the CARES Act. Enacted H.R. 748 on March 27, 2020.
H.R. 6410, To direct the President to use authority under the Defense Production Act of 1950 to ensure an adequate supply of equipment necessary for limiting the spread of COVID-19. Referred to the House Committee on Financial Services on March 27, 2020.
H.R. 6398, To provide for the expedited procurement of equipment needed to combat COVID-19 under the Defense Production Act of 1950. Referred to the House Subcommittee on Economic Development, Public Buildings, and Emergency Management on March 27, 2020.
H.R. 6406, To require personal protective equipment to be included in the strategic national stockpile, and to require the Federal Government to procure such equipment from United States sources, and for other purposes. Referred to the Subcommittee on Economic Development, Public Buildings, and Emergency Management on March 27, 2020.
H.R. 6405, To direct the President, in consultation with the Secretary of the Treasury, to develop and carry out a strategy to seek reimbursement from the People's Republic of China of funds made available by the United States Government to address the Coronavirus Disease 2019 (COVID-19). Referred to the House Committee on Foreign Affairs on March 26, 2020.
S. 3586, Eliminating Leftover Expenses for Campaigns from Taxpayers (ELECT) Act of 2020. Referred to the Senate Committee on Finance on March 25, 2020.
H.R. 6390, To require the President to use authorities under the Defense Production Act of 1950 to require emergency production of medical equipment to address the COVID-19 outbreak. Referred to the House Committee on Financial Services on March 25, 2020.
H.R. 6393, To require the Secretary of Defense to submit to Congress a report on the reliance by the Department of Defense on imports of certain pharmaceutical products made in part or in whole in certain countries, to establish postmarket reporting requirements for pharmaceuticals, and for other purposes. Referred to the House Committee on Ways and Means, and in addition to the House Committees on Armed Services, Oversight and Reform, and Energy and Commerce on March 25, 2020. As of April 15, 2020, no text of the bill was available.
S.Res. 552, A resolution supporting an international investigation into the handling by the Government of the People's Republic of China of COVID-19 and the impact of handling COVID-19 in that manner on the people of the United States and other nations. Referred to the Senate Committee on Foreign Relations on March 24, 2020.
H.Res. 907 and S.Res. 553, Expressing the sense of the House of Representatives that the Government of the People's Republic of China made multiple, serious mistakes in the early stages of the COVID-19 outbreak that heightened the severity and spread of the ongoing COVID-19 pandemic, which include the Chinese Government's intentional spread of misinformation to downplay the risks of the virus, a refusal to cooperate with international health authorities, internal censorship of doctors and journalists, and malicious disregard for the health of ethnic minorities. Referred to the House Committee on Foreign Affairs on March 24, 2020.
S. 3573, American-Made Protection for Healthcare Workers and First Responders Act. Referred to the Senate Committee on Health, Education, Labor, and Pensions on March 24, 2020.
S. 3570, A bill to provide for the expedited procurement of equipment needed to combat COVID-19 under the Defense Production Act of 1950. Referred to the Senate Committee on Banking, Housing, and Urban Affairs on March 23, 2020.
S. 3568, Medical Supply Chain Emergency Act of 2020. Referred to the Senate Committee on Banking, Housing, and Urban Affairs on March 23, 2020.
H.R. 6379, Take Responsibility for Workers and Families Act, Referred to the House Committee on Appropriations, and in addition to the House Committees on the Budget, and Ways and Means on March 23, 2020.
H.R. 6373, To increase the amount available under the Defense Production Act of 1950 to respond to the coronavirus epidemic, and for other purposes. Referred to the House Committee on Financial Services on March 23, 2020.
H.R. 6371, To amend the Securities Exchange Act of 1934 to require issuers to disclose risks related to global pandemics, and for other purposes. Referred to the House Committee on Financial Services on March 23, 2020.
H.R. 6319, To establish a Congressional COVID-19 Aid Oversight Panel, to authorize the Special Inspector General for the Troubled Asset Relief Program to coordinate audits and investigations in connection with the receipt of Federal aid related to COVID-19, and for other purposes. Referred to the House Committee on Financial Services on March 23, 2020.
H.Res. 906, Calling on the President to invoke the Defense Production Act to respond to COVID-19. Referred to the House Committee on Financial Services on March 23, 2020.
S. 3548, Coronavirus Aid, Relief, and Economic Security Act or the CARES Act. Referred to the Senate Committee on Finance on March 21, 2020.
H.R. 6310, To require the Secretary of Defense to make testing for the coronavirus disease 19 available to all members of the Armed Forces deployed to an area in which the United States Central Command has responsibility. Referred to the House Committee on Armed Services, March 19, 2020.
H.R. 6482, A bill to require the Secretary of Health and Human Services to maintain a list of the country of origin of all drugs marketed in the United States, to ban the use of Federal funds for the purchase of drugs manufactured in China, and for other purposes. Referred to the Senate Committee on Finance on March 19, 2020.
S. 3538, Strengthening America's Supply Chain and National Security Act. Referred to the Senate Committee on Finance, March 19, 2020.
S. 3537, Protecting Our Pharmaceutical Supply Chain from China Act of 2020. Referred to the Senate Committee on Finance, March 19, 2020.
S.Res. 547, A resolution encouraging the President to use authorities provided by the Defense Production Act of 1950 to scale up the national response to the coronavirus crisis. Referred to the Senate Committee on Banking, Housing, and Urban Affairs, March 18, 2020.
S. 3530, A bill to amend the National Security Act of 1947 to require the President to designate an employee of the National Security Council to be responsible for pandemic prevention and response, and for other purposes. Referred to the Senate Committee on Homeland Security and Governmental Affairs on March 18, 2020.
S. 3507, A bill to require the Secretary of Defense to make testing for the coronavirus disease 19 available to all members of the Armed Forces deployed to an area in which the United States Central Command has responsibility. Referred to the Senate Committee on Armed Services on March 17, 2020.
S. 3510, A bill to transfer all border wall funding to the Department of Health and Human Services and USAID to combat coronavirus. Referred to the Committee on Homeland Security and Government Affairs on March 17, 2020.
H.R. 6288, Responsibly Responding to Pandemics Act. Referred to the House Subcommittee on Economic Development, Public Buildings, and Emergency Management, March 16, 2016.
H.R. 6205, Assistance for Workers Harmed by COVID-19 Act. Amends the Trade Act of 1974 to provide adjustment assistance to certain workers adversely affected by disruptions in global supply chains from COVID–19, and for other purposes. Referred to the House Committee on Ways and Means on March 11, 2020.
P.L. 116-123, Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020. Provides $7.8 billion in supplemental appropriations to aid in domestic and global COVID-19 preparedness and response activities, including $6.5 billion for the Department of Health and Human Services (HHS), $0.02 billion for the Small Business Administration and $1.3 billion for foreign operations activities provided across several agencies and funding mechanisms. Parts of the HHS amounts are to be made available for international activities. Enacted H.R. 6074 on March 6, 2020.
S.Amdt. 1506, To rescind unobligated balances for certain international programs to offset the amounts appropriated in this bill to respond to the coronavirus outbreak. Motion to table the amendment was agreed to in the Senate on March 5, 2020.
S.Res. 497, A resolution commemorating the life of Dr. Li Wenliang and calling for transparency and cooperation from the Government of the People's Republic of China and the Communist Party. Agreed to in the Senate on March 3, 2020 without amendment and an amended preamble by unanimous consent.
H.R. 6070, Border Health Security Act of 2020. To establish grant programs to improve the health of border area residents and for all hazards preparedness in the border area including bioterrorism, infectious disease, and noncommunicable emerging threats, and for other purposes. Referred to the House Committee on Energy and Commerce and Committee on Foreign Affairs on March 3, 2020.
S.Res. 511, A resolution supporting the role of the United States in helping save the lives of children and protecting the health of people in developing countries with vaccines and immunization through GAVI, the Vaccine Alliance. Referred to the Senate Committee on Foreign Relations, February 27, 2020.
S.Res. 505, A resolution expressing the sense of the Senate that the United States will continue to provide support to international partners to help prevent and stop the spread of coronavirus. Referred to the Senate Committee on Foreign Relations on February 13, 2020.
H.R. 2166 and S. 3302, Global Health Security Act of 2020. Establishes a Special Advisor for Global Health Security within the Executive Office of the President to coordinate U.S. government global health security activities, convene and chair a Global Health Security Interagency Review Council, and submit a biannual report to Congress on related activities, among other things. Referred to the Senate Committee on Foreign Relations on February 13, 2020.
H.R. 5730, National Strategy for Pandemic Influenza Update Act. To direct the Homeland Security Council and the National Security Council, in consultation with Federal departments and agencies responsible for biodefense, to update the National Strategy for Pandemic Influenza, and for other purposes. Referred to the House Committees on Energy and Commerce, Armed Services, Foreign Affairs, Intelligence, and Agriculture on January 30, 2020.
P.L. 116-22, Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. To advance research and development of innovative tools to improve pandemic preparedness, including directing the Secretary of Health and Human Services to submit a report to the Senate Committee on Health, Education, Labor, and Pensions and the House Committee on Energy and Commerce on U.S. efforts to coordinate with other countries and international partners during recent public health emergencies with respect to the research and advanced research on, and development of, qualified pandemic or epidemic products. Enacted S. 1379 on June 24, 2019.
H.R. 269, Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. Related to S. 1379, which became P.L. 116-22. Placed on Senate Legislative Calendar under General Orders, January 10, 2019.