Health Resources and Services Administration (HRSA) FY2020 President’s Budget Request and Agency Funding History: In Brief
The Health Resources and Services Administration (HRSA) within the Department of Health and Human Services (HHS) provides health care to individuals who are geographically isolated and/or economically or medically vulnerable. The agency’s programs target specific populations, including pregnant women and their children and individuals with HIV/AIDs.
HRSA is organized into five bureaus: (1) Primary Care; (2) Health Workforce; (3) Maternal and Child Health; (4) HIV/AIDS; and (5) Healthcare Systems. In addition to these bureaus, HRSA has 11 offices. Some offices focus on specific populations or health care issues (e.g., Office of Women’s Health, Federal Office of Rural Health Policy), while others provide agency-wide support or technical assistance to HRSA’s regional offices (e.g., Office of Planning, Analysis and Evaluation; Office of Regional Operations).
This fact sheet focuses on the agency’s funding; a number of specific HRSA programs are described in more detail in other CRS products.
HRSA’s funding sources include—in order of magnitude—discretionary appropriations, mandatory funding, the Vaccine Injury Compensation Program Trust Fund, and user fees. For FY2019, the agency’s program funding level was $11.99 billion. Of that amount, $6.85 was from the agency’s discretionary appropriation. For FY2020, the President’s budget requests $5.85 billion in discretionary appropriations, an amount that would be approximately $1.0 million less than in the FY2019 appropriation. The FY2020 budget request proposed reducing funding for programs in most HRSA bureaus, with the largest reductions for programs administered by the Health Workforce Bureau. The President’s FY2020 budget request includes proposals to continue the agency’s mandatory funding sources at their current funding levels; under the President’s budget, the FY2020 program funding level would be $11.02 billion.
Health Resources and Services Administration (HRSA) FY2020 President's Budget Request and Agency Funding History: In Brief
Jump to Main Text of Report
Contents
Summary
The Health Resources and Services Administration (HRSA) within the Department of Health and Human Services (HHS) provides health care to individuals who are geographically isolated and/or economically or medically vulnerable. The agency's programs target specific populations, including pregnant women and their children and individuals with HIV/AIDs.
HRSA is organized into five bureaus: (1) Primary Care; (2) Health Workforce; (3) Maternal and Child Health; (4) HIV/AIDS; and (5) Healthcare Systems. In addition to these bureaus, HRSA has 11 offices. Some offices focus on specific populations or health care issues (e.g., Office of Women's Health, Federal Office of Rural Health Policy), while others provide agency-wide support or technical assistance to HRSA's regional offices (e.g., Office of Planning, Analysis and Evaluation; Office of Regional Operations).
This fact sheet focuses on the agency's funding; a number of specific HRSA programs are described in more detail in other CRS products.
HRSA's funding sources include—in order of magnitude—discretionary appropriations, mandatory funding, the Vaccine Injury Compensation Program Trust Fund, and user fees. For FY2019, the agency's program funding level was $11.99 billion. Of that amount, $6.85 was from the agency's discretionary appropriation. For FY2020, the President's budget requests $5.85 billion in discretionary appropriations, an amount that would be approximately $1.0 million less than in the FY2019 appropriation. The FY2020 budget request proposed reducing funding for programs in most HRSA bureaus, with the largest reductions for programs administered by the Health Workforce Bureau. The President's FY2020 budget request includes proposals to continue the agency's mandatory funding sources at their current funding levels; under the President's budget, the FY2020 program funding level would be $11.02 billion.
Agency Overview
The Health Resources and Services Administration (HRSA) within the Department of Health and Human Services (HHS) provides health care to individuals who are geographically isolated and/or economically or medically vulnerable. The agency's programs target specific populations, including pregnant women and children and individuals with Human Immunodeficiency Virus/Acquired Immunity Deficiency Syndrome (HIV/AIDS). HRSA also supports the health care workforce; oversees organ, bone marrow, and umbilical cord blood donation; and compensates individuals harmed by vaccination. HRSA currently awards funding to more than 3,000 grantees, including community-based organizations; colleges and universities; hospitals; state, local, and tribal governments; and private entities. These funds support health services projects, such as training health care workers and providing specific health services.1
HRSA is organized into five bureaus: (1) Primary Care; (2) Health Workforce; (3) Maternal and Child Health; (4) HIV/AIDS; and (5) Healthcare Systems. In addition to these bureaus, HRSA has 11 offices. Some offices focus on specific populations or health care issues (e.g., Office of Women's Health, Federal Office of Rural Health Policy), while others provide agency-wide support or technical assistance to HRSA's regional offices (e.g., Office of Planning, Analysis and Evaluation; Office of Regional Operations).
This fact sheet focuses on the agency's funding; a number of specific HRSA programs are described in more detail in other CRS reports.2
Funding Sources
For the time period discussed in this fact sheet—FY2015 through the FY2020 President's budget request—HRSA has four major sources of funding, described in order of magnitude: (1) discretionary appropriations, (2) mandatory funds directly appropriated in the Patient Protection and Affordable Care Act (ACA, P.L. 111-148, as amended), (3) the Vaccine Injury Compensation Program Trust Fund; and (4) user fees.
HRSA receives its discretionary appropriations through the Labor, HHS, and Education and Related Agencies (LHHS) Appropriations Act.3 HRSA began receiving mandatory appropriations from the ACA to support specific programs in FY2010.4 For example, the ACA established the Maternal, Infant, and Early Childhood Home Visiting Program.5 HRSA also receives mandatory appropriations through the LHHS Appropriations Act from the Vaccine Injury Compensation Program Trust Fund to pay claims associated with vaccine-related injury or death.6 Finally, HRSA has the authority to collect user fees for specified activities; the authority to expend these fees is provided in annual LHHS appropriations acts. In prior years, some HRSA programs have received funds from the Public Health Service (PHS) Program Evaluation Set-Aside.7
Funding for a number of HRSA's mandatory ACA programs was extended through November 21, 2019, by the Continuing Appropriations Act, 2020, and the Health Extenders Act of 2019 (P.L. 116-59). The FY2020 President's budget request proposes to continue mandatory funding for these programs at current levels. Previously, these programs had been extended in the Bipartisan Budget Act of 2018 (BBA 2018, P.L. 115-123), which generally included funding for FY2018 and FY2019.8 Many of these programs received funding extensions for FY2016 and FY2017 in the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA, P.L. 114-10).9 Legislation has been introduced that would extend some of these funding sources for a longer duration, but no further extension legislation has been enacted as of the date of this report's publication.
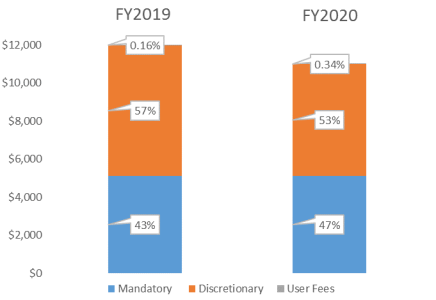
The figures below show the agency's funding distribution in FY2019 and the FY2020 President's request. The President's budget proposes a new user fee that would increase user fees as a percentage of total funding that the agency would receive in FY2020. It also requests smaller levels of discretionary funding. Amounts of mandatory funding provided would generally remain the same. As such, mandatory funding as a percentage of the agency's total funding would increase under the President's FY2020 budget.
|
Figure 1. Composition of HRSA Funding Sources, FY2019 Enacted and FY2020 Proposed |
 |
|
Source: CRS analysis of HRSA Budget Justification data. The mandatory share of HRSA funding includes mandatory amounts from the Vaccine Injury Compensation Trust Fund. (These amounts are typically excluded, by convention, from totals in the HRSA budget justification, but have been included here in order to match totals in Table 1.) |
The FY2020 President's Budget Request
Table 1 presents enacted funding for HRSA in FY2015-FY2019, along with the FY2020 President's budget request. Although appropriations for HRSA have increased over time, the FY2018 funding levels represented a larger increase over the preceding year than funding levels provided in prior years. The FY2018 increases were generally sustained or further expanded in FY2019. In particular, the FY2019 appropriations bill included increases for a number of Bureau of Health Workforce Programs, including increased discretionary funds for the National Health Service Corps and funding for a new Graduate Medical Education program to support medical schools in states with predicted primary care shortages. In addition, the FY2019 appropriations act sustained funding increases that began in FY2018 for Rural Health programs and included a funding increase from $100 million to $120 million for the Rural Communities Opioids Response program, which began in FY2018. The program supports activities that aim to increase access to opioid treatment and prevention services in rural areas.10
They FY2020 President's budget request represents a decrease from FY2019 funding for a number of HRSA programs and activities. Specifically, it would eliminate funding for a number of Bureau of Health Workforce Programs, such as those that support training in primary care and oral health. It would also eliminate funding for a number of Maternal and Child Health Bureau Programs, such as those that focus on pediatric mental health and screening for maternal depression and programs related autism and developmental disorders. The FY2020 budget request would maintain funding for behavioral health workforce development, but it proposes reductions in funding for Maternal Child Health Block Grants. The President's budget request also calls for decreased or no funding for a number of Rural Health Programs—for example, it requests less funding for telehealth programs and for rural health outreach grants, and no funding for Rural Flexibility Grants, State Offices of Rural Health, and Rural Residency Training. The budget request would maintain funding for Radiation Exposure Screening and Education Programs, Black Lung Programs, and for the Rural Communities Opioid Response program.
The President's budget requests $70 million for the HIV/AIDS Bureau as part of the Administration's larger Ending the HIV Epidemic Initiative. These funds would be used to provide areas with high HIV rates with additional expertise, technology, and resources.11 These funds would be for the HIV/AIDs Bureau, in addition to funding amounts requested to support the Ryan White HIV/AIDS program.
Table 1 presents funding levels for selected programs and totals for each of HRSA's bureaus. The table presents enacted funding levels for FY2015-FY2019. FY2020 appropriations have not yet been enacted, but the table displays amounts requested in the FY2020 President's budget.
Table 1. Health Resources and Services Administration (HRSA)
(Budget Authority in Millions, by Fiscal Year)
|
Bureau or Activity |
FY2015 |
FY2016 |
FY2017 |
FY2018 |
FY2019 |
FY2020 President's Request |
|
Primary Care |
||||||
|
Health Centers |
5,001 |
5,091 |
4,998 |
5,447 |
5,506 |
5,506 |
|
Discretionarya (non-add) |
(1,392) |
(1,392) |
(1,387) |
(1,507) |
(1,506) |
(1,506) |
|
CHCF Transfer (non-add) |
(3,509) |
(3,600)b |
(3,511)b |
(3,800)c |
(4,000)c |
(4,000)d |
|
Precision Medicine Initiativee (non-add) |
— |
— |
— |
(25)c |
— |
|
|
Health Center Tort Claims (non-add) |
(100) |
(100) |
(100) |
(115) |
(120) |
(120) |
|
Free Clinics |
0.1 |
0.1 |
1.0 |
1.0 |
1.0 |
1.0 |
|
Subtotal, Primary Care |
5,001 |
5,092 |
4,999 |
5,448 |
5,627 |
5,627 |
|
Health Workforce |
||||||
|
National Health Service Corps (NHSC) |
287 |
310 |
289 |
415 |
430 |
415 |
|
Discretionary (non-add) |
— |
— |
— |
(105) |
(120) |
(105) |
|
CHCF Transfer (non-add) |
(287) |
(310)b |
(289)b |
(310)c |
(310)c |
(310)d |
|
Training for Diversityf |
83 |
83 |
83 |
88 |
88 |
0 |
|
Primary Care Training and Enhancement |
39 |
39 |
39 |
49 |
49 |
0 |
|
Oral Health |
34 |
36 |
37 |
41 |
41 |
0 |
|
Interdisciplinary, Community-Based Linkagesg |
108 |
79 |
129 |
191 |
192 |
112 |
|
Health Care Workforce Assessment |
5 |
5 |
5 |
6 |
6 |
5 |
|
Public Health Workforce Development |
21 |
21 |
17 |
17 |
17 |
0 |
|
Nursing Workforce Developmenth |
232 |
229 |
229 |
249 |
234 |
83i |
|
Children's Hospital GME Payments |
265 |
295 |
299 |
314 |
325 |
0 |
|
Teaching Health Center GME Payments (ACA Sec. 5508(c)) |
—j |
60b |
56b |
127c |
127c |
127d |
|
Graduate Medical Education |
— |
— |
— |
— |
25 |
0 |
|
National Practitioner Data Bank (User Fees) |
19 |
21 |
19 |
19 |
19 |
19 |
|
Subtotal, Health Workforce |
1,093 |
1,178 |
1,200 |
1,514 |
1,552 |
760 |
|
Maternal and Child Health |
||||||
|
Maternal and Child Health Block Grant |
637 |
638 |
640 |
650 |
678 |
661 |
|
Healthy Start |
102 |
104 |
118k |
110 |
123 |
123 |
|
Home Visiting (ACA Sec. 2951) |
400l |
400b |
372b |
400c |
400c |
400c |
|
Family-to-Family Health Centers (ACA Sec. 5507) |
5m |
5b |
5b |
6c |
6c |
6d |
|
Other Maternal and Child Health Programsn |
103 |
103 |
103 |
124 |
127 |
0 |
|
Subtotal, Maternal and Child Health |
1,247 |
1,250 |
1,239 |
1,291 |
1,333 |
1,189 |
|
Ryan White HIV/AIDS |
||||||
|
Ryan White HIV/AIDS |
2,319 |
2,323 |
2,313 |
2,313 |
2,319 |
2,389o |
|
Ending the HIV Epidemic Initiative |
— |
— |
— |
— |
— |
(70) |
|
Subtotal, Ryan White HIV/AIDS |
2,319 |
2,323 |
2,313 |
2,313 |
2,319 |
2,389o |
|
Health Care Systems |
||||||
|
Other Health Care Systems Programsp |
76 |
76 |
77 |
86 |
89 |
87 |
|
Hansen's Disease Programsq |
17 |
17 |
17 |
16 |
16 |
14 |
|
340B Drug Pricing Programs/Office of Pharmacy Affairs |
10 |
10 |
10 |
10 |
10 |
10 |
|
340B Drug Pricing Program (User Fees) |
— |
— |
— |
— |
— |
19 |
|
Subtotal, Health Care Systems |
103 |
103 |
104 |
111 |
115 |
130 |
|
Rural Health |
||||||
|
Rural Communities Opioid Response |
— |
— |
— |
100 |
120 |
120 |
|
Rural Residency |
— |
— |
— |
15 |
10 |
— |
|
Other Rural Healthr |
147 |
150 |
156 |
175 |
188 |
69 |
|
Subtotal, Rural Health |
147 |
150 |
156 |
290 |
318 |
189 |
|
Other Activities |
||||||
|
Family Planning |
286 |
286 |
286 |
286 |
286 |
286 |
|
Program Management |
154 |
154 |
154 |
155 |
155 |
152 |
|
Vaccine Injury Compensation (Program Operations) |
8 |
8 |
8 |
9 |
9 |
11 |
|
Vaccine Injury Compensation Program (HRSA Claims)s |
235s |
253s |
282s |
227s |
280s |
286s |
|
Subtotal, Other Activities |
683 |
701 |
730 |
677 |
731 |
735 |
|
Total, Program Level |
10,593 |
10,796 |
10,740 |
11,643 |
11,994 |
11,018 |
|
Less Funds From Sources Other than the Discretionary Appropriation |
||||||
|
User Fees |
19 |
21 |
19 |
19 |
19 |
38 |
|
Vaccine Injury Compensation Claims (Mandatory)s |
235 |
253 |
282 |
268 |
280 |
286 |
|
ACA Mandatory Funds |
4,201 |
4,375 |
4,232 |
4,668t |
4,843 |
4,843 |
|
Total, Discretionary Budget Authority |
6,138 |
6,147 |
6,207 |
6,730 |
6,853 |
5,853 |
Sources: The funding amounts are from HRSA congressional budget justifications. Amounts for FY2015 are drawn from the FY2017 justification, amounts for FY2016 are drawn from the FY2018 justification, amounts for FY2017 are drawn from the FY2019 justification, and amounts for FY2018-FY2020 are drawn from the FY2020 justification. Congressional budget justifications are available at http://www.hhs.gov/budget/.
Notes: Bolded rows indicate total bureau funding. Individual amounts may not add to subtotals or totals due to rounding. The FY2020 President's request level reflects amounts as requested by the President.
a. Includes funding for Native Hawaiian Programs.
b. These funds were appropriated in Medicare Access and CHIP Reauthorization Act of 2015 (P.L. 114-10). Amounts appropriated were reduced in FY2017 because of budget sequestration. CRS Report R45941, The Annual Sequester of Mandatory Spending through FY2029.
c. These funds were appropriated in the Bipartisan Budget Act of 2018 (BBA 2018, P.L. 115-123).
d. The President's request proposes FY2020 mandatory funding for this program.
e. BBA 2018, Section 50901(b), appropriated $25 million to HRSA for FY2018 to support the participation of health centers in the All of Us Research Program, part of the National Institutes of Health Precision Medicine Initiative.
f. Training for Diversity includes Centers for Excellence, Scholarships for Disadvantaged Students, Faculty Loan Repayment, and the Health Careers Opportunity Program.
g. Interdisciplinary, Community-Based Linkages includes Area Health Education Centers, Geriatric Programs, and Mental and Behavioral Health Education and Training. FY2015 and FY2016 amounts reflect the Behavioral Health Workforce Education and Training Program (a component of the Mental and Behavioral Health Education and Training).
h. Nursing Workforce Development includes NURSE Corps; Advanced Nursing Education; Nursing Workforce Diversity; Nurse Education, Practice, Quality and Retention; Nurse Faculty Loan Program; and Comprehensive Geriatric Education.
i. The FY2020 budget proposes funding for the NURSE Corps program but does not propose funding for other Nursing Workforce Development programs.
j. ACA Section 5508(c) appropriated $230 million to support graduate medical education payments to teaching health centers to be used from FY2011 through FY2015.
k. Includes $15 million appropriated in the Water Infrastructure Improvements for the Nation Act (P.L. 114-322). See CRS Report R44723, Overview of Further Continuing Appropriations for FY2017 (H.R. 2028).
l. P.L. 113-93 provided $400 million for this program for the first half of FY2015. P.L. 114-10 extended the availability of these funds through all of FY2015.
m. P.L. 113-93 provided $2.5 million for this program for FY2015, which was superseded by the full-year funding ($5 million) for this program for FY2015 enacted in P.L. 114-10.
n. Other Maternal and Child Health Programs includes Autism and Other Developmental Disorders, Sickle Cell Services Demonstration, Universal Newborn Hearing Screening, Emergency Medical Services for Children, and Heritable Disorders, Screening and Treatment for Maternal Depression and Pediatric Mental Health Access. The latter two programs were new in FY2018. In FY2015, this account also included $9 million for the Traumatic Brain Injury program, but this program was transferred to the Administration for Community Living in FY2016 and, therefore, was not funded under HRSA. Per source materials, the $9 million in FY2015 funding for this program is not included above.
o. Includes $70 million for the Administration's Ending the HIV Epidemic Initiative.
p. Other Health Care Systems Programs includes Organ Transplantation, National Cord Blood Inventory, C.W. Bill Young Cell Transplantation Program, and Poison Control Centers.
q. Hansen's Disease Programs includes Hansen's Disease Center, Payments to Hawaii (for Hansen's Disease) and National Hansen's Disease Program—Buildings and Facilities. The FY2020 President's budget does not propose funding for the National Hansen's Disease Program—Buildings and Facilities program.
r. Other Rural Health includes Rural Health Policy Development, Rural Hospital Outreach Grants, Rural Hospital Flexibility Grants, State Offices of Rural Health, Radiation Exposure Screening and Education Program, Black Lung Clinics, and Telehealth grant programs.
s. By convention, mandatory funding for claims under the Vaccine Injury Compensation Trust Fund are not counted toward agency totals displayed in the HRSA's congressional budget justification. However, they have been included in the overall agency program level totals shown in this fact sheet.
t. Includes the $25 million appropriated in BBA 2018 to support health center participation in the All of Us Research Program, part of the National Institutes of Health Precision Medicine Initiative.
Author Contact Information
Footnotes
| 1. |
See HRSA's website at http://www.hrsa.gov. |
| 2. |
See CRS Report R43911, The Community Health Center Fund: In Brief; CRS Report R43937, Federal Health Centers: An Overview; CRS Report R44970, The National Health Service Corps; CRS Report R43930, Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program: Background and Funding; CRS In Focus IF10595, Maternal, Infant, and Early Childhood Home Visiting Program; CRS Report R44970, The National Health Service Corps; CRS Report R44282, The Ryan White HIV/AIDS Program: Overview and Impact of the Affordable Care Act; CRS Report R44929, Maternal and Child Health Services Block Grant: Background and Funding; CRS In Focus IF10777, Maternal and Child Health (MCH) Services Block Grant; CRS Report R45181, Family Planning Program Under Title X of the Public Health Service Act; and CRS Report R44282, The Ryan White HIV/AIDS Program: Overview and Impact of the Affordable Care Act. |
| 3. |
For more information, see CRS Report R45083, Labor, Health and Human Services, and Education: FY2018 Appropriations. |
| 4. |
These programs are described in CRS Report R41278, Public Health, Workforce, Quality, and Related Provisions in ACA: Summary and Timeline. |
| 5. |
CRS Report R43930, Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program: Background and Funding; CRS In Focus IF10595, Maternal, Infant, and Early Childhood Home Visiting Program. |
| 6. |
The LHHS Appropriations Act also provides HRSA with a smaller discretionary appropriation from the Vaccine Injury Compensation Program Trust Fund to support administrative expenses associated with this program. |
| 7. |
For more information, see CRS Report R43304, Public Health Service Agencies: Overview and Funding (FY2010-FY2016). |
| 8. |
CRS Report R45136, Bipartisan Budget Act of 2018 (P.L. 115-123): CHIP, Public Health, Home Visiting, and Medicaid Provisions in Division E. While the BBA 2018 generally extended mandatory ACA funding streams through FY2019, mandatory appropriations for the Maternal, Infant, and Early Childhood Home Visiting program were extended through FY2022. |
| 9. |
Medicare Access and CHIP Reauthorization Act of 2015; see CRS Report R43962, The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA; P.L. 114-10). |
| 10. |
P.L. 115-141 U.S. Congress, House Committee on Appropriations, Department of Defense for the Fiscal Year Ending September 30, 2019 and for Other Purposes, Conference Report to Accompany H.R. 6157, 115th Cong., 2nd sess., September 13, 2018, H.Rept. 115-952, p. 521. |
| 11. |
FY2020 HRSA congressional budget justification, p. 263. |