National Institutes of Health (NIH) Funding: FY1996-FY2026
Changes from May 12, 2020 to June 29, 2021
This page shows textual changes in the document between the two versions indicated in the dates above. Textual matter removed in the later version is indicated with red strikethrough and textual matter added in the later version is indicated with blue.
Summary
This report details the National Institutes of Health (NIH) budget and appropriations process with a focus on FY2020 and FY2021, and on coronavirus supplemental funding for NIHNational Institutes of Health (NIH) Funding:
June 29, 2021
FY1996-FY2022
Kavya Sekar
This report details the National Institutes of Health (NIH) budget and appropriations
Analyst in Health Policy
process with a focus on FY2020, FY2021, and FY2022. Coronavirus supplemental
funding for NIH is discussed in a dedicated section of the report but is general y not included in the budgetary figures elsewhere in the report. The report also provides an
. The report also provides an overview of funding trends in regular appropriations to the agency from FY1995 to FY2021FY1996 to FY2022. Appendix A includes funding tables by account and program-specific funding levels for FY2020, FY2021, and FY2022. Appendix B provides a list of acronyms and abbreviations used in the report.
and FY2021.
The NIH is the primary federal agency charged with conducting and supporting medical, health, and behavioral research, and it is made up of 27 Institutes and Centers and the Office of the Director (OD). About 80% of the NIH budget funds extramural research through grants, contracts, and other awards. About 10% of NIH funding goes to intramural researchers at NIH-operated facilities. Almost all al of NIH'’s funding is provided in the annual
Departments of Labor, Health and Human Services, and Education, and Related Agencies (LHHS) Appropriations Act. NIH also receives smallersmal er amounts of funding from Interior/Environmental (INT) appropriations and a mandatory budget authority for type 1 diabetes research.
NIH has an FY2020 program level of $41.685 billion and has received emergency supplemental appropriations in three coronavirus supplemental appropriations acts, totaling over $3.59 billion—an 8.6% funding increase over regular enacted FY2020 appropriations. The administration's FY2021 budget request, as amended by a March 2020 letter, proposes an FY2021 program level of $39.133 billion—a 6.1% decrease from the FY2020 program level (regular appropriations).
The FY2021 NIH program level of $42.936 bil ion represents a $1.251 bil ion increase (+3.0%) above the FY2020-enacted program level. The FY2021-enacted total for NIH is also $3.802 bil ion (+9.7%) above the FY2021 budget request and $715 mil ion (+1.7%) above the program level proposed by the House-passed LHHS
and INT bil s. In FY2021, al Institute and Center (IC) accounts received an increase above FY2020 funding levels, except for the Buildings and Facilities account (see Table A-1). The Biden Administration’s FY2022 budget request proposes an FY2022 program level of $51.953 bil ion—a $9.017 bil ion increase (+21.0%) from the FY2021 program level. It also proposes the creation of a new Advanced Research Projects Agency for Health (ARPA-H) within NIH.
NIH has seen periods of high and low funding growth during the period covered by this report, as illustratedil ustrated in Figure 1. Between FY1994FY1996 and FY1998, funding for NIH grew from $11.0 billion to $13.7 billion928 bil ion to $13.675 bil ion (nominal dollars). Over the next five years, Congress and the President doubled the NIH budget to $27.2 billion167 bil ion in FY2003. In each of FY1999 through FY2003, NIH received annual funding increases of 14% to 16%. From FY2003 to FY2015, NIH funding increased more graduallygradual y in nominal dollars. In some years (FY2006, FY2011,
and FY2013), funding for the agency decreased in nominal dollars. From FY2016 through FY2020, NIH has seen funding increases of over 5% each year. The largest increase was from FY2017 to FY2018, where the program level increased by $3.0 billion (+8.7010 bil ion (+8.8%), making this the largest single-year nominal dollar increase since FY2003.
The proposed funding increase in the FY2022 budget request would be over twice this amount.
When looking at NIH funding adjusted for inflation (in projected constant FY2021FY2022 dollars using the Biomedical
Research and Development Price Index; BRDPI), the purchasing power of NIH funding peaked in FY2003—the last year of the five-year doubling period—and then declined fairly steadily for more than a decade until back-to-back funding increases were provided in each of FY2016 through FY2020FY2021. The FY2021 program level is 3.3% below the peak FY2003 program level. The FY2022. The FY2021 budget request would provide a program level that is 13.0% below14.4% above the peak FY2003 program level.
NIH Funding: FY1995-FY2021
Congressional Research Service
link to page 4 link to page 5 link to page 6 link to page 8 link to page 10 link to page 11 link to page 13 link to page 14 link to page 16 link to page 18 link to page 20 link to page 16 link to page 21 link to page 22 National Institutes of Health (NIH) Funding: FY1996-FY2022
Contents
NIH Funding: FY1996-FY2022 ........................................................................................ 1
Funding Sources........................................................................................................ 2
Coronavirus Supplemental Appropriations (FY2020 and FY2021) .................................... 3 FY2021 Proposed and Enacted Funding ........................................................................ 5 FY2022 Budget and Appropriations.............................................................................. 7 Trends ..................................................................................................................... 8
Figures Figure 1. National Institutes of Health (NIH) Funding, FY1996-FY2022 ............................... 10
Tables
Table 1. NIH Funding, FY1996-FY2022........................................................................... 11
Table A-1. National Institutes of Health Funding................................................................ 13 Table A-2. Specified NIH Funding Levels in FY2021 Explanatory Statement ......................... 15 Table A-3. Specified NIH Funding Levels in FY2022 Budget Request .................................. 17
Appendixes Appendix A. NIH Funding Details ................................................................................... 13 Appendix B. Acronyms and Abbreviations ........................................................................ 18
Contacts
Author Information ....................................................................................................... 19
Congressional Research Service
link to page 6 link to page 6 National Institutes of Health (NIH) Funding: FY1996-FY2022
NIH Funding: FY1996-FY2022 This report provides a historical overview of federal funding provided to the National Institutes of Health (NIH) between FY1995 and FY2021FY1996 and FY2022. It also provides a brief explanation of the discretionary spending funding sources for NIH associated with the annual appropriations process (via the Labor, HHS, and Education and Interior/Environment Appropriations Acts) and the
mandatory funding for special program on type 1 diabetes research.1
1
NIH is the primary federal agency for medical, health, and behavioral research. It is the largest of the eight health-related agencies that make up the Public Health Service (PHS) within the Department of Health and Human Services (HHS).22 NIH consists of the Office of the Director
(OD) and 27 Institutes and Centers (ICs) that focus on aspects of health, human development, and biomedical science. The OD sets overall overal policy for NIH and coordinates the programs and
activities of all al NIH components, particularly in areas of research that involve multiple institutes.
Supplemental Funding for NIH
|
NIH activities cover a wide range of basic, clinical, and translational research, focused on particular diseases, areas of human health and development, or more fundamental aspects of biology and behavior. Its mission also includes research training and health information collection and dissemination.3 More than 80% of the NIH budget funds extramural research (i.e., external) through grants, contracts, and other awards. This funding supports research performed by more than 300,000 individuals who work at over 2,500 hospitals, medical schools, universities, and other research institutions around the country.4 About 10% of the agency's budget supports intramural research (i.e., internal) conducted by nearly 6,000 NIH physicians and scientists, most of whom are located on the NIH campus in Bethesda, Maryland.5
Funding Sources
Funding for NIH of the
the agency’s budget supports intramural
FY2020 and FY2021 amounts for the COVID-19
research (i.e., internal) conducted by nearly
pandemic is provided in “Coronavirus Supplemental
6,000 NIH physicians and scientists, most of
Appropriations.”
whom are located on the NIH campus in
Bethesda, Maryland.5
1 “Mandatory spending” is controlled by authorization acts; “discretionary spending” is controlled by appropriations acts. For further information, see CRS Report R44582, Overview of Funding Mechanism s in the Federal Budget Process, and Selected Exam ples.
2 T he Public Health Service also includes the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality (AHRQ), the Health Resources and Services Administration (HRSA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Indian Health Service (IHS), and the Agency for T oxic Substances and Disease Registry (AT SDR). 3 For further information on T he National Institutes of Health (NIH), see CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues.
4 NIH, “What We Do- Budget,” March 3, 2020, at https://www.nih.gov/about-nih/what-we-do/budget. 5 Ibid.
Congressional Research Service
1
link to page 16 National Institutes of Health (NIH) Funding: FY1996-FY2022
Funding Sources The vast majority of NIH funding comes from annual discretionary appropriations bil s. NIH
additional y receives some mandatory funding and some funding due to unique transfer or budgetary rules, as explained below. The total funding available for NIH activities, taking account
of add-ons and PHS tap transfers, is referred to as the NIH “program level.”
Discretionary budget authority: NIH’s discretionary budget authority comes primarily from annual Labor, HHS, and Education (LHHS) Appropriations Acts, with an additional smaller smal er amount for the Superfund Research Program and related activities from the Interior/Environment Appropriations Act.6 Those two bills provide NIH discretionary budget authority.
(INT) Appropriations Act.6
PHS Evaluation Set-Aside: Through LHHS appropriations, some funding is also transferred to NIH pursuantsubject to the PHS Evaluation Set-Aside or the "“PHS Evaluation Tap"” transfer authority.77 Authorized by Section 241 of the Public Health Service Act, the evaluation tap allowsal ows the Secretary of HHS, with the approval of appropriators, to redistribute a portion of eligible PHS agency appropriations across
HHS for program evaluation and implementation purposes. The PHSA section limits the set-aside to not less than 0.2% and not more than 1% of eligible program appropriations. However, LHHS Appropriations Acts have commonly established a higher maximum percentage for the set-aside and have distributedappropriated specific amounts of "tap"“tap” funding to selected HHS programs.—in the context of NIH, these appropriations have been made to National Institute of General Medical
Sciences in recent years.8 Since FY2010, and including in FY2020FY2021, this higher maximum set-aside level has been 2.5% of eligible appropriations.89 Readers should note that totals in this report and NIH source documents include amounts "“transferred in"” pursuant to PHS tap but do not
include any amounts "“transferred out"” under this same authority.
Nonrecurring expenses fund (NEF): The NEF permits HHS to transfer unobligated balances of expired discretionary funds from FY2008 and subsequent years into the NEF account. Statute authorizes use of the funds for capital acquisitions, including information technology (IT) and facilities infrastructure (42 U.S.C. §3514a), and can direct the funds to certain accounts through
appropriations acts. As shown in Table A-1, Congress directed specific amounts from the NEF to
the NIH Building and Facilities account in FY2020 and FY2021.
6 T he Hazardous Substance Basic Research and T raining Program (Superfund Research Program ) funds research on the health effects of exposures to hazardous substances and related solutions at the National Institute of Environmental Health Sciences. It is authorized by 311(a) of the Comprehensive Environmental Response, Compensation, and Liability Act of 1980 (42 U.S.C. §9660(a)) and Section 126(g) of the Superfund Amendments and Reauthorization Act of 1986.
7 For more information on the PHS Evaluation T ap, or PHS Evaluation Set -Aside, see discussion in CRS Report R44916, Public Health Service Agencies: Overview and Funding (FY2016 -FY2018). 8 Prior to FY2015, NIH had traditionally been by far the largest net donor of tap funds, rather than a net recipient. T he joint explanatory statement accompanying the FY2015 omnibus explained this shift as being intended to ensure that tap transfers are a “ net benefit to NIH rather than a liability” and noted that this change was in response to a growing concern at the loss of NIH funds to the tap. Joint Explanatory Statement, Proceedings and Debates of the 113th Congress, Second Session, Congressional Record, vol. 160, no. 151, Book II, December 11, 2014, p. H9832.
9 See Section 204 of Division H, T itle II of P.L. 116-260 for the FY2021 maximum set-aside level. T he last time that an appropriations act set the PHS tap percentage at a level other than 2.5% was in FY2009, when it was 2.4% (see P.L. 111-8). T he FY2020 omnibus also retained a change to this provision, first included in the FY2014 omnibus, allowing tap transfers to be used for the “evaluation and the implementation” of programs funded in the HHS title of the LHHS Appropriations Act. Prior to FY2014, such provisions had restricted tap funds to the “ evaluation of the implementation” of programs authorized under the Public Health Service Act.
Congressional Research Service
2
National Institutes of Health (NIH) Funding: FY1996-FY2022
21st Century Cures Act Innovation Account: NIH also receives funding through LHHS appropriations, subject to different budget enforcement rules than the rest of the NIH funding in the act—appropriations to the NIH Innovation Account created by The 21st21st Century Cures Act ("(“the Cures Act," ” P.L. 114-255) to fund programs authorized by the act.910 For appropriated amounts to the account—up the limit authorized for each fiscal year—the amounts are subtracted from any cost estimate for enforcing discretionary spending limits (i.e., the budget caps). In
effect, appropriations to the NIH Innovation Account as authorized by the Cures Act are not subject to discretionary spending limits.1011 The NIH Director may transfer these amounts from the NIH Innovation Account to other NIH accounts, but only for the purposes specified in the Cures Act. If the NIH Director determines that the funds for any of the four Innovation Projects are not necessary, the amounts may be transferred back to the NIH Innovation Account. All amounts Al amounts
authorized by the Cures Act have been fully appropriated to the Innovation Account from FY2017 to FY2021to FY2020, including $492 million for FY2020. For FY2021, $404 million is authorized to be appropriated.11
404 mil ion for FY2021. Under the FY2022 budget request, the full
amount authorized by the Cures Act ($496 mil ion) would be appropriated.
Mandatory Type I Diabetes Funding: In addition, NIH has received mandatory funding of $150 million annuallymil ion annual y that is provided in Public Health Service Act (PHSA) Section 330B, for a special program on type 1 diabetes research, most recently extended through FY2020FY2023 by the CARES Act (P.L. 116-136), with additional partial-year FY2021 funding of $25,068,493 for October 1, 2020, through November 30, 2020.
The total funding available for NIH activities, taking account of add-ons and PHS tap transfers, is referred to as the NIH "program level."
FY2020-Enacted Funding
The enacted FY2020 NIH program level is made up of the following:12
- $40.228 billion in discretionary LHHS appropriations, including the $492 million authorized for the Cures Act Innovation Account;
- $1.231 billion pursuant to the PHS program evaluation transfer and a $225 million transfer from the HHS non-recurring expenses fund (NEF);13
- $81 million for the Superfund research program in Interior/Environment appropriations; and
- $150 million in annual funding for the mandatory type 1 diabetes research program.
Accounting for transfers and other adjustments, cited FY2021 budget documents from the Administration show the NIH FY2020 program level as $41.685 billion.14
Coronavirus Supplemental Appropriations
NIH has also received emergency supplemental appropriations to several IC accounts as provided by the first and third, coronavirus supplemental appropriations acts, shown in Table 1, totaling $1.8 billion. In addition to these appropriations, the fourth coronavirus supplemental required that a total of not less than $1.8 billion of $25 billion appropriated to the Public Health and Social Services Emergency Fund be transferred to two NIH institutes and the Office of the Director. When accounting for these transfers, total funding directed to the NIH would come to not less than $3.6 billion across the three acts—an 8.6% funding increase over regular enacted FY2020 appropriations.
These acts also include various other transfer authorities that would allow for additional transfers to and from NIH accounts (explained in the table notes).
Table 1. NIH Funding in Coronavirus Supplemental Appropriations Acts
(budget authority, in millions of dollars)
Source: Supplemental appropriations acts, as cited.
Notes: All funding is designated as being provided as an emergency requirement. All funding in the first and third supplemental appropriations acts is available until September 30, 2024. Funding in the fourth appropriations act is available until expended. The three acts include HHS transfer authorities. Per the first supplemental, HHS may transfer funds between the Centers for Disease Control and Prevention (CDC), Public Health and Social Services Emergency Fund (PHSSEF), and NIH accounts, as specified. Pursuant to the third supplemental, HHS may transfer funds between the Administration for Children and Families (ACF), Administration for Community Living (ACL), CDC, NIH, and PHSSEF accounts, as specified. In addition, the CDC Director may transfer funds appropriated to the Infectious Disease Rapid Response Fund (IRRRDF) to NIH. Per the fourth supplemental, HHS may transfer certain funds among the CDC, NIH, PHSSEF, and the Food and Drug Administration accounts, as specified.
a. Amounts provided in P.L. 116-139 are provided as transfers from the Public Health and Social Services Emergency Fund (PHSSEF) and are provided specifically for research and development related to COVID-19 tests, as specified for each transfer.
b. Of this total, not less than $156 million shall be provided for "the study of, construction of, demolition of, renovation of, and acquisition of equipment for, vaccine and infectious diseases research facilities of or used by NIH, including the acquisition of real property."
c. NLT stands for "not less than."
By convention, CRS does not add amounts provided as an emergency requirement to the NIH program levels in the remainder of this report. The FY2020 regular and emergency appropriations amounts are presented separately.
FY2021 Budget and Appropriations
President Trump's FY2021 initial Budget and Appropriations President Biden’s FY2022 budget request (February 10, 2020) proposedMay 28, 2021) proposes that NIH be provided with a
total program level of $38.694 billion, a decrease of $2.99 billion (-7.2%) from FY2020-51.953 bil ion, an increase of $9.017 bil ion (+21.0%) from FY2021-
enacted levels. The proposed FY2020FY2022 program level would have beenbe made up of28
$50.456 bil ion in discretionary LHHS budget authority (nontransfer); $1.272 bil ion pursuant to the PHS program evaluation transfer; $84 mil ion for the Superfund research program and related activities from
Interior/Environment appropriations; and
$141 mil ion in annual funding for the mandatory type 1 diabetes research
program.29
Under this request, al existing IC accounts would receive an increase compared to FY2021-enacted levels (see made up of15
- $37.630 billion in LHHS appropriations, including the $404 million for the Cures Act Innovation Account (the full amount authorized for FY2021);
- $741 million in transfers to NIH pursuant to the PHS Evaluation Tap authority;
- $74 million for the Superfund Research Program in Interior/Environment appropriations; and
- $150 million in proposed annual funding for the mandatory type 1 diabetes program.
Under the request, all existing IC accounts would receive a decrease compared to FY2020-enacted levels (see Appendix A). The Building and Facilities account would receive an increase in LHHS budget authority, from $200 million in FY2020 to $300 million in FY2021.16
Subsequently, on March 17, 2020, the Office of Management and Budget submitted an amendment to President Trump's original request that would increase funding for the National Institute of Allergy and Infectious Disease (NIAID) by $440 million relative to the original request. 17 The purpose of this additional requested funding was "to ensure [NIAID] has the resources beginning October 1, 2020, to continue critical basic and applied research on coronaviruses and other infectious diseases." This amendment to the original proposal, if enacted, would result in NIAID receiving an increase of $9.3 million above the FY2020 level. Taking into account this amendment, as of the date of this report, the FY2021 budget request would provide NIH with a total program level of $39.133 billion, a decrease of $2.55 billion (-6.1%) from FY2020-enacted levels, with a total of $38.811 billion by provided by LHHS appropriations.
In addition, the FY2021 budget request proposes consolidating the Agency for Healthcare Research and Quality (AHRQ) into NIH, forming a 28th IC—the National Institute for Research on Safety and Quality (NIRSQ). The creation of a new NIH institute would require amendments to the PHSA, especially Section 401(d), which specifies that "[i]n the National Institutes of Health, the number of national research institutes and national centers may not exceed a total of 27." Under the FY2021 request, NISRQ would receive a total appropriation of $355.112 million, including $256.66 million in discretionary LHHS budget authority and $98.452 million in mandatory appropriations from the Patient-Centered Outcomes Research Trust Fund (PCORTF) in Social Security Act Section 1181.18 Congress did not adopt the Administration's similar proposals to consolidate AHRQ into NIH as NIRSQ in FY2018 through FY2020.19
The budget request proposes select specified FY2021 funding levels for programs and activities within and across the NIH accounts based on the Administration's research priorities, as summarized in Table A-3. If adopted, these funding levels would likely be specified in report and/or explanatory statement language accompanying LHHS appropriations bills. For the most part, Congress does not specify NIH funding for particular diseases or areas of research, instead allowing the ICs to award funding within their mission areas. Funding awards are generally made on a competitive basis through various funding mechanisms intended to balance scientific opportunity with health priorities.20
Trends
Table 2 Appendix A). In addition, the full amount ($496 mil ion) authorized by the 21st Century Cures Act for FY2021 (P.L. 114-255) would be appropriated to the Innovation Account. The Buildings and Facilities (B&F) account would receive an increase of $50 mil ion
(+25%) in LHHS discretionary budget authority, but an overal decrease of $175 mil ion (-41%)
26 T he NEF amount is not reflected in the FY2021 NIH program level in cited FY2022 budget request tables. 27 See NIH, Congressional Justification: FY2022, May 28, 2021, p. 89-91, at https://officeofbudget.od.nih.gov/pdfs/FY22/br/2022%20CJ%20Overview%20Volume%20May%2028.pdf. Specifically, FY2022 budget documents reflect a transfer from NIH to HHS OIG, transfers between IC accounts, and do not account for the NEF transfer to the B&F account. 28 NIH, Congressional Justification: FY2022, May 28, 2021, p. 89-91, at https://officeofbudget.od.nih.gov/pdfs/FY22/br/2022%20CJ%20Overview%20Volume%20May%2028.pdf .
29 T his proposed amount for the mandatory type 1 diabetes research program differs from the already enacted amount for FY2022 of $150 million in PHSA Section 330B, as amended in P.L. 116-260, Division BB, T itle III. According to the budget request, the FY2022 amount reflects sequestration of $8.55 million. See “Budget Mechanism T able,” p. 92 in https://officeofbudget.od.nih.gov/pdfs/FY22/br/2022%20CJ%20Overview%20Supplementary%20Tables.pdf .
Congressional Research Service
7
link to page 14 link to page 13 National Institutes of Health (NIH) Funding: FY1996-FY2022
when accounting for the additional NEF transfer of $225 mil ion directed to the B&F account in
FY2021 appropriations.30
The FY2022 budget request also proposes the creation of an Advanced Research Projects Agency
for Health (ARPA-H) within NIH. The budget request included $6.5 bil ion for ARPA-H “to build platforms and capabilities to deliver cures for cancer, Alzheimer’s disease, diabetes, and other diseases.”31 The $6.5 bil ion for ARPA-H would account for 72.1% of the FY2022 budget request’s $9.017 bil ion increase from FY2021-enacted levels. Further information on the ARPA-
H proposal is provided below.
Advanced Research Projects Agency for Health (ARPA-H) in the FY2022
Budget Request
On May 28, 2021, the Office of Budget and Management (OMB) submitted President Biden’s FY2022 budget request to Congress. This budget request proposed the creation of an Advanced Research Projects Agency for Health (ARPA-H) within the National Institutes of Health (NIH). The budget request included $6.5 bil ion for ARPA-H “to build platforms and capabilities to deliver cures for cancer, Alzheimer’s disease, diabetes, and other diseases.” Funding was requested for a period of three years to “al ow for both scale-up in FY 2022 and redeployment of resources in the next two years if projects fail to meet performance milestones.” The vast majority of funding would support extramural research, with a smal amount of funding reserved for staffing and administrative functions. Unlike NIH Institutes and Centers (ICs), ARPA-H would not have its own intramural research program. ARPA-H would be modeled after the Defense Advanced Research Projects Agency (DARPA) , which primarily works with the Department of Defense (DOD), and would contain several “DARPA model” characteristics, including a flat and nimble organizational structure, tenure-limited program managers with a high degree of autonomy to select and fund projects, and a milestone-based contract approach. While this organizational structure would be “operational y unique” from NIH ICs, ARPA-H would stil coordinate research and activities with NIH ICs and other HHS agencies. The FY2022 budget request describes four broad project areas that ARPA-H would fund:
tackling bold chal enges requiring large scale, sustained, cross-sector coordination;
creating new capabilities (e.g., technologies, data resources, disease models);
supporting high-risk exploration that could establish entirely new paradigms; and
overcoming market failures through critical solutions, including financial incentives.
Most ARPA-H awards would be given to industry, universities, and nonprofit research institutions, and may involve some agreements with other federal agencies. ARPA-H would make use of some of NIH’s flexible hiring and funding authorities, such as its Other Transaction Authority mechanisms.32 For further information and analysis regarding ARPA-H, see CRS Insight IN11674, Advanced Research Projects Agency for Health (ARPA-H): Considerations for Congress
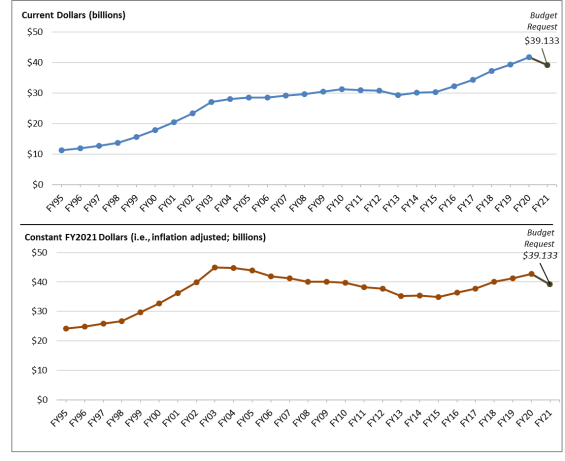
Trends Table 1 outlines NIH program level funding over the previous 25 years; Figure 1 illustrates il ustrates funding trends in both current (also calledcal ed nominal dollars) and projected constant (i.e., inflation-
adjusted) FY2021FY2022 dollars (funding shown is total budget authority).
NIH has seen periods of high and low funding growth. Between FY1994
30 Accounting for the directed NEF transfer, the Buildings and Facilities account has a total FY2021 funding level of $425 million. T his total account amount is not reflected in budget request documents.
31 NIH, Congressional Justification: FY2022, May 28, 2021, p . 10, at https://officeofbudget.od.nih.gov/pdfs/FY22/br/2022%20CJ%20Overview%20Volume%20May%2028.pdf.
32 NIH, Congressional Justification: FY2022, May 28, 2021, pp. 10-11, at https://officeofbudget.od.nih.gov/pdfs/FY22/br/2022%20CJ%20Overview%20Volume%20May%2028.pdf and HHS, “FY2022 Budget in Brief,” pp. 59-60, at https://www.hhs.gov/sites/default/files/fy-2022-budget-in-brief.pdf.
Congressional Research Service
8
link to page 13 link to page 14 National Institutes of Health (NIH) Funding: FY1996-FY2022
NIH has seen periods of high and low funding growth. Between FY1996 and FY1998, funding for NIH grew from $11.0 billion to $13.7 billion928 bil ion to $13.675 bil ion (nominal dollars). Over the next five years, Congress and the President doubled the NIH budget to $27.2 billion167 bil ion in FY2003. In each of FY1999 through FY2003, NIH received annual funding increases of 14% to 16%. From FY2003 to FY2015, NIH funding increased more graduallygradual y in nominal dollars.2133 In some years, (FY2006, FY2011, and FY2013) funding for the agency decreased in nominal dollars.2234 From FY2016
through FY2020, NIH has seen funding increases of over 5% each year. The largest increase was from FY2017 to FY2018, where the program level increased by $3.0 billion (+8.7010 bil ion (+8.8%), making this the largest single-year nominal dollar increase since FY2003.
(If adopted, the FY2022
request program level would surpass this prior largest annual program level increase).
The lower half of Figure 1 shows NIH funding adjusted for inflation (in projected constant FY2021FY2022 dollars) using the Biomedical Research and Development Price Index (BRDPI).2335 It shows that the purchasing power of NIH funding peaked in FY2003 (the last year of the five-year doubling period) and then declined fairly steadily for more than a decade until back-to-back consecutive
funding increases were provided in each of FY2016 through FY2020FY2021. The FY2021 program level is 3.3% below the peak FY2003 program level. The FY2022. The FY2021 budget request would provide a
program level that is 13.0% below14.4% above the peak FY2003 program level.
33 Amounts shown in Table 1 include appropriations for the Global Fund to Fight AIDS, T B, and Malaria (FY2002 -FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identify ing resources for the Global Fund; this responsibility was transferred to another federal agency. For further details on the amounts transferred out by fiscal year, see the
“Supplemental Appropriation Data T able” for “History of Congressional Appropriations, Fiscal Years 2000-2012” the peak FY2003 program level.
Program Level Funding in Current and Projected Constant (FY2021) Dollars. |
 |
. Notes: By convention, program level |
Table 2. NIH Funding, FY1995-FY2021
in “Coronavirus Supplemental Appropriations”).
Congressional Research Service
10
link to page 15 link to page 14 National Institutes of Health (NIH) Funding: FY1996-FY2022
Table 1. NIH Funding, FY1996-FY2022
Program Level Funding in Current and Constant (FY2021) Dollars (billions)
|
Fiscal Year |
Program Level Current $ |
% Change |
Program Level Projected Constant FY2021 $ |
|
|
1995 |
11.300 |
3.1% |
24.101 |
|
|
1996 |
11.928 |
5.6% |
24.806 |
|
|
1997 |
12.741 |
6.8% |
25.780 |
|
|
1998 |
13.675 |
7.3% |
26.762 |
|
|
1999 |
15.629 |
14.3% |
29.648 |
|
|
2000 |
17.841 |
14.1% |
32.628 |
|
|
2001 |
20.459 |
14.7% |
36.212 |
|
|
2002 |
23.321 |
14.0% |
39.955 |
|
|
2003 |
27.167 |
16.5% |
44.963 |
|
|
2004 |
28.037 |
3.2% |
44.736 |
-0.5% |
|
2005 |
28.594 |
2.0% |
43.917 |
-2.3% |
|
2006 |
28.560 |
-0.1% |
41.924 |
-6.8% |
|
2007 |
29.179 |
2.2% |
41.266 |
-8.2% |
|
2008 |
29.607 |
1.5% |
40.000 |
-11.0% |
|
2009 |
30.545 |
3.2% |
40.093 |
-10.8% |
|
2010 |
31.238 |
2.3% |
39.793 |
-11.5% |
|
2011 |
30.916 |
-1.0% |
38.288 |
-14.8% |
|
2012 |
30.861 |
-0.2% |
37.736 |
-16.1% |
|
2013 |
29.316 |
-5.0% |
35.187 |
-21.7% |
|
2014 |
30.143 |
2.8% |
35.419 |
-21.2% |
|
2015 |
30.311 |
0.6% |
34.906 |
-22.4% |
|
2016 |
32.311 |
6.6% |
36.418 |
-19.0% |
|
2017 |
34.301 |
6.2% |
37.681 |
-16.2% |
|
2018 |
37.311 |
8.8% |
39.990 |
-11.1% |
|
2019 |
39.313 |
5.4% |
41.256 |
-8.2% |
|
2020 |
41.685 |
6% |
42.686 |
-5.1% |
|
2021PB |
39.133 |
-6.1% |
39.133 |
-13.0% |
Sources: NIH Budget Office, Appropriations History FY2022) Dol ars (bil ions)
Program Level
Program Level Projected
% Below
Fiscal Year
Current $
% Change
Constant FY2021 $
FY2003a
1996
11.928
5.6%
25.045
1997
12.741
6.8%
26.028
1998
13.675
7.3%
27.020
1999
15.629
14.3%
29.934
2000
17.841
14.1%
32.942
2001
20.459
14.7%
36.561
2002
23.321
14.0%
40.340
2003
27.167
16.5%
45.396
2004
28.037
3.2%
45.167
-0.5%
2005
28.594
2.0%
44.341
-2.3%
2006
28.560
-0.1%
42.328
-6.8%
2007
29.179
2.2%
41.664
-8.2%
2008
29.607
1.5%
40.385
-11.0%
2009
30.545
3.2%
40.480
-10.8%
2010
31.238
2.3%
40.176
-11.5%
2011
30.916
-1.0%
38.657
-14.8%
2012
30.861
-0.2%
38.099
-16.1%
2013
29.316
-5.0%
35.526
-21.7%
2014
30.143
2.8%
35.760
-21.2%
2015
30.311
0.6%
35.243
-22.4%
2016
32.311
6.6%
36.769
-19.0%
2017
34.301
6.2%
38.044
-16.2%
2018
37.311
8.8%
40.375
-11.1%
2019
39.313
5.4%
41.661
-8.2%
2020
41.685
6.0%
43.483
-4.2%
2021
42.936
3.0%
43.887
-3.3%
2022PB
51.953
21.0%
51.953
+14.4%
Sources: NIH Budget Office, Appropriations History by Institute/Center (1938 to Present), at https://officeofbudget.od.nih.gov/approp_hist.html. The FY2020 and FY2021. The FY2020, FY2021, and FY2022 program levels are based on NIH, Congressional Justification: FY2022, May 28, 2021, p. 89-91,on NIH, "FY2021 Budget Request by IC (Summary Table)," at https://officeofbudget.od.nih.gov/pdfs/FY21/br/5-SupplementaryTables.pdf, with FY2021 request amended to reflect budget request amendment in letter from Michael R. Pence, President of the Senate, to Donald Trump, President of the United States, March 17, 2020, at https://www.whitehouse.gov/wp-content/uploads/2020/03/Letter-regarding-additional-funding-to-support-the-United-States-response-to-COVID-19-3.17.2020.pdf.
Inflation pdfs/FY22/br/2022%20CJ%20Overview%20Volume%20May%2028.pdf . Inflation adjustment reflects the Biomedical Research and Development Price Index (BRDPI), updated January 2020 March 2021, at https://officeofbudget.od.nih.gov/gbiPriceIndexes.html.
. Notes: By convention, budget tables, such as as Table 2,1, include amounts "“transferred in"” pursuant to PHS tap but do not include any amounts "“transferred out"” under this same authority. Program level includes all al budget authority, including appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002 -FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy Al ergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. In general, amounts provided to NIH for emergency requirements are requirements are
Congressional Research Service
11
link to page 6 National Institutes of Health (NIH) Funding: FY1996-FY2022
excluded from these totals (e.g., the FY2020 amount doesand FY2021 amounts do not include the amounts provided in the coronavirus supplemental appropriations acts, summarized in Table 1 of this report in “Coronavirus Supplemental Appropriations”). PB denotes "President'“President’s Budget.” a. FY2003 was the year that NIH received the most program level funding.
Congressional Research Service
12
link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 National Institutes of Health (NIH) Funding: FY1996-FY2022
Appendix A. s Budget."
a. FY2003 was the peak funding year for the NIH program level.
b. The FY2020 program level shown in table differs from enacted amounts in Further Consolidated Appropriations Act, 2020 (P.L. 116-94), accounting for a transfer of $5 million from the Office of the Director to the HHS Office of the Inspector General (OIG). In addition, FY2021 budget documents do not reflect the Nonrecurring Expenses Fund transfer of $225 million to NIH in the FY2020 program level, as directed by P.L. 116-94.
Appendix A.
NIH Funding Details
NIH Funding Details Table A-1. National Institutes of Health Funding
(budget authority, in mil ions of dol ars)
FY2020
FY2021
FY2021
FY2022
Institutes/Centers
Final
Request
Final
Request
Cancer Institute (NCI)
$6,440
$5,881
$6,559
$6,733
Heart, Lung, and Blood Institute (NHLBI)
$3,625
$3,298
$3,665
$3,846
Dental/Craniofacial (budget authority, in millions of dollars)
|
Institutes/Centers |
|
|
|
|
|
Cancer Institute (NCI) |
$6,440 |
$5,881 |
— |
— |
|
Heart, Lung, and Blood Institute (NHLBI) |
$3,625 |
$3,298 |
— |
— |
|
Dental/Craniofacial Research (NIDCR) |
$478 |
$435 |
— |
— |
Research (NIDCR)
$478
$435
$485
$516
Diabetes/Digestive/Kidney |
$2,115 |
$1,924 |
— |
— |
|
Neurological Disorders/Stroke (NINDS) |
$2,447 |
$2,245 |
— |
— |
|
$5,876 |
$5,885 |
— |
— |
|
$1,706 |
$1,931 |
— |
— |
|
Child Health/Human Development (NICHD) |
$1,557 |
$1,416 |
— |
— |
|
National Eye Institute (NEI) |
$823 |
$749 |
— |
— |
|
$803 |
$730 |
— |
— |
|
National Institute on Aging (NIA) |
$3,546 |
$3,226 |
— |
— |
|
Arthritis/Musculoskeletal/Skin Diseases (NIAMS) |
$625 |
$568 |
— |
— |
|
Deafness/Communication Disorders (NIDCD) |
$491 |
$446 |
— |
— |
|
National Institute of Mental Health (NIMH) |
$2,043 |
$1,845 |
— |
— |
|
National Institute on Drug Abuse (NIDA) |
$1,458 |
$1,432 |
— |
— |
|
Alcohol Abuse/Alcoholism (NIAAA) |
$547 |
$497 |
— |
— |
|
Nursing Research (NINR) |
$172 |
$157 |
— |
— |
|
Human Genome Research Institute (NHGRI) |
$604 |
$550 |
— |
— |
|
$405 |
$368 |
— |
— |
|
Minority Health/Health Disparities (NIMHD) |
$336 |
$305 |
— |
— |
|
Complementary/Integrative Health (NCCIH) |
$152 |
$138 |
— |
— |
|
Advancing Translational Sciences (NCATS) |
$833 |
$788 |
— |
— |
|
Fogarty International Center (FIC) |
$81 |
$74 |
— |
— |
|
National Library of Medicine (NLM) |
$457 |
$416 |
— |
— |
|
$2,247 |
$2,099 |
— |
— |
|
$157 |
$109 |
— |
— |
|
Buildings and Facilities (B&F) |
$200 |
$300 |
— |
— |
National Institute for Research on Safety & Quality (NIRSQ)
—
$257
—
—
Advanced Research Projects Agency for Health (ARPA-H)
—
—
—
$6,500
Subtotal, |
— |
$257 |
— |
— |
|
Subtotal, NIH (LHHS Discretionary BA) |
$40,223 |
$38,811 |
— |
— |
|
PHS Program Evaluation (provided to NIGMS) |
$1,231 |
$741 |
— |
— |
|
$81 |
$74 |
— |
— |
|
|
— |
— |
— |
|
$150 |
$150 |
— |
— |
|
Patient-Centered Outcomes Research Trust Fund (PCORTF) |
— |
$98 |
||
|
NIH Program Level |
$41,685 |
$39,133 |
— |
— |
Source: NIH, "FY2021 Budget Request by IC (Summary Table),"NIH (LHHS Discretionary BA)
$40,223
$38,070
$41,432
$50,456
PHS Program Evaluation (provided to NIGMS)
$1,231
$741
$1,272
$1,272
Congressional Research Service
13
link to page 17 link to page 17 link to page 17 link to page 18 link to page 16 link to page 6 link to page 6 National Institutes of Health (NIH) Funding: FY1996-FY2022
FY2020
FY2021
FY2021
FY2022
Institutes/Centers
Final
Request
Final
Request
Superfund (Interior approp. to NIEHS)i
$81
$74
$82
$84
Nonrecurring Expenses Fund (NEF) Transfer (to
($225)
—
($225)
—
Buildings and Facilities)j
Mandatory type 1 diabetes funds (to NIDDK)k
$150
$150
$150
$141l
Patient-Centered Outcomes Research Trust Fund
—
$98
—
—
(PCORTF)
NIH Program Level
$41,685
$39,133
$42,936
$51,953
Source: NIH, “FY2022 Budget Request by IC (Summary Table),” at https://officeofbudget.od.nih.gov/pdfs/FY21/br/5-SupplementaryTables.pdf, pdfs/FY22/br/2022%20CJ%20Overview%20Supplementary%20Tables.pdf , pg. 89, except as noted below.
FY2021 request amounts from Rep. Nancy Pelosi, “Explanatory Statement Submitted by Mrs. Lowey, Chairwoman of the House Committee on Appropriations Regarding H.R. 133, Consolidated Appropriations Act, 2021,” House of Representatives, Congressional Record, daily edition, vol. 166, part No.218—Book IV (December 21, 2020). Notes: Totals may differ from the sum of the components due to rounding. Amounts in table may differ from actuals in many cases. By convention, budget tables such as as Table A-1 do not subtract the amount of transfers to the evaluation tap from the agencies' appropriation. Amounts for the columns headed "FY2021 House," and "FY2021 Senate" will be added, if available, as each action is completed. ’ appropriation. In general, amounts provided to NIH for emergency requirements requirements are excluded from these totals (e.g., FY2020 amount does FY2020 and FY2021 amounts do not include the amounts provided in the coronavirus supplemental appropriations acts, summarized in Table 1 of this report).
a. Amounts for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) in “Coronavirus Supplemental Appropriations”). a. Amounts for the NIDDK do not include mandatory funding for type 1 diabetes research (see note h).
b. k). b. The White House amended the NIAID FY2021 budget request on March 17, 2020, in a supplemental
request letter for COVID-19 funding, to $5,885,470,000, which is $439,584,000 above the original FY2021 budget request.
c. Amounts for NIGMSbudget request.
c. Amounts for National Institute of General Medical Sciences (NIGMS) do not include funds from PHS Evaluation Set-Aside (§241 of the PHS Act). Though the budget request provides an increase to NIGMS through discretionary LHHS budget authority (BA) compared to FY2020, the total amount for NIGMS with the PHS evaluation transfer included would be less than FY2020-enacted levels.
d. Amounts for National Institute of Environmental Health Sciences (NIEHS) do not include Interior/Environment d. FY2020 and FY2021 funding level for NICHD adjusted for comparability in NIH FY2022 budget tables to
reflect the proposed transfer of the ECHO and INCLUDE programs from OD to NICHD.
e. Amounts for NIEHS do not include Interior/Environment Appropriations amount for Superfund research
(see note g).
e. i).
f.
Includes $12.6 million for the Gabriella Miller Kids First mil ion transfer from the Pediatric Research Initiative Fund (PRIF) as authorized by the Gabriel a Mil er Kids First Research Act. FY2020 and FY2021 amounts for this account adjusted for comparability reflect the proposed transfer of ECHO and INCLUDE programs from OD to NICHD in the FY2022 request.
g. Research Act.
f. The amount shown for the NIH Innovation Account in each column represents only a portion of the total
appropriation to the account ($492 million for the FY2020; $404 million for FY2021)404 mil ion for FY2021: $496 mil ion for FY2022. The remaining funds for this account are incorporated, reflected, where applicable, into the totals for other ICs. For FY2021FY2022, this includes $195 194 mil ion to NCI for cancer research and $50 million and $76 mil ion to each of NINDS and NIMH for the BRAIN Initiative.
g. ($152 mil ion total for BRAIN).
h. Amounts for the Building and Facilities account do not include directed transfers from the nonrecurring
expenses fund in FY2020 and FY2021 enacted appropriations (see note j).
i.
This is a separate account in the Interior/Environment appropriations for National Institute of Environmental Health Sciences (NIEHS)NIEHS research activities related to Superfund research.
h.
j.
The nonrecurring expenses fund (NEF) permits HHS to transfer unobligated balances of expired discretionary discretionary funds from FY2008 and subsequent years into the NEF account. Congress and the President authorized use of the funds for capital acquisitions including information technology (IT) and facilities infrastructure (42 U.S.C. §3514a).
i. Though FY2020 LHHS enacted appropriations (P.L. 116-94) directed an NEF transfer of $225 million to the Buildings and Facilities account, this transfer was not reflected in the FY2021 budget request tables and therefore is shown as a non-add in this table.
j. , and can direct the funds to certain accounts through appropriations acts. NEF transfers are shown as non-add in this budget presentation as these amounts were not reflected in FY2022 budget request tables.
k. Mandatory funds are available to NIDDK for type 1 diabetes research are under PHSA Section 330Bm. For FY2020, this funding has been extended by the Coronavirus Aid, Relief, and Economic Security Act (P.L. 116-136) through FY2020, with a temporary FY2021 extension through November 30, 2020. Cited FY2021 budget request documents show $150 million as the FY2021 proposed funding level.
Program-Specific Funding
, which
was most recently extended through FY2023 by the Consolidated Appropriations Act, 2021 (P.L. 116 -260; Division BB, Title II)
Congressional Research Service
14
link to page 18 National Institutes of Health (NIH) Funding: FY1996-FY2022
l.
FY2022 proposed amount for the type I diabetes research program ($141 mil ion) is lower than enacted funding level for FY2022 ($150 mil ion). According to the budget request, the FY2022 amount reflects sequestration of $8.55 mil ion. See “Budget Mechanism Table,” p. 92 in https://officeofbudget.od.nih.gov/pdfs/FY22/br/2022%20CJ%20Overview%20Supplementary%20Tables.pdf.
Program-Specific Funding In recent years, Congress and the President have increasingly specified funding levels for programs or research areas within NIH accounts throughout the budget and appropriations
process. Congress uses language in reports and explanatory statements accompanying appropriations billsbil s to designate funding for specified purposes. The Administration requests NIH program-specific funding, as outlined in the HHS and NIH budget request documents.This is a relatively new practice that has expanded since FY2015.36 For the most part, Congress does not specify NIH funding for particular diseases or areas of research, instead allowingal owing the ICs to award funding within their mission areas. Funding is generallygeneral y awarded on a flexible and competitive basis through various
funding mechanisms intended to balance scientific opportunity with health priorities.24
In FY202037
In FY2021, Congress used explanatory statement language to specify a certain amount of IC funding for designated purposes, as summarized inin Table A-2. Sometimes the language specifies
that "“no less than"” a certain amount can be designated for a certain purpose; in other cases, language “provides” or “recommends”language "provides" or "recommends" that an amount be spent on a certain purpose. For FY2020, FY2021, while the House report (H.Rept. 116-62450) also included funding levels for some of the below programs, the amounts in the explanatory statement supersede those. Both the explanatory statement and the House report include many additional statements directing the agency to
prioritize certain programs or areas of research, as well wel as expressing the opinion or concerns of Congress regarding NIH; these broad statements are not summarized here.
In addition, the President has proposed broad funding increases for certain research and other areas in his FY2022
budget request.
Table A-2. Specified NIH Funding Levels in FY2020FY2021 Explanatory Statement
Institute/Center
Program
Amount
Cancer Institute (NCI)
NCI Paylines
$250 mil ion, an increase of $38 mil ion
Childhood Cancer Survivorship, Treatment
$30 mil ion
Access, Explanatory Statement
|
Institute/Center |
Program |
Amount |
|
Cancer Institute (NCI) |
Childhood Cancer Data Initiative |
$50 million |
|
Additional cancer research awards |
$212.5 million |
|
|
Childhood Cancer Survivorship, Treatment Access, and Research (STAR) Act |
$25 million |
|
|
Neurological Disorders/Stroke (NINDS) |
|
$250 million |
|
Allergy/Infectious Diseases (NIAID) |
AIDS2020 Conference (International AIDS Conference) |
$5.1 million |
|
Combating antimicrobial resistance (AMR) |
$511 million, an increase of $50 million |
|
|
NASEM study on the long-term medical and economic impacts of increased AMR in the United States |
$1.7 million |
|
|
HIV/AIDS research |
an increase of no less than $25 million over FY2019 level |
|
|
Centers for AIDS Research |
$51 million |
|
|
Universal flu vaccine |
$200 million, an increase of $60 million |
|
|
General Medical Sciences (NIGMS) |
Institutional Development Award (IDeA) Program |
$386.6, an increase of $25 million |
|
Environmental Health Sciences (NIEHS) |
Hurricane Harvey research |
$3 million |
|
Aging (NIA) |
Alzheimer's disease and related dementias |
Increase of $350 million; total funding no less than $2.818 billion |
|
Drug Abuse (NIDA) |
Opioid misuse and addiction |
$250 million |
|
Genome Research (NHGRI) |
Emerging Centers of Excellence in Genomic Sciences |
$10 million |
|
Minority Health/Health Disparities (NIMHD) |
Research Centers in Minority Institutions |
$75 million |
|
Advancing Translational Sciences (NCATS) |
Clinical and Translational Science Awards (CTSAs) |
$578.1 million |
|
Cures Acceleration Network |
up to $60 million |
|
|
Office of the Director (OD)/ Multi-Institute Research Initiatives |
All of Us Precision Medicine Initiative |
$500 million (including $149 million from the Innovation Account) |
|
NASEM study of NIH research on autoimmune conditions that predominately affect women. |
$1.5 million |
|
|
Big data- Chief Data Strategist's work |
$30 million |
|
|
Grants for biomedical research facilities |
$50 million |
|
|
Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative |
$500 million (including $140 million from the Innovation Account) |
|
|
Firearm injury and mortality prevention research |
$12.5 million |
|
|
HHS Office of National Security allocation for foreign threats program |
$5 million |
|
|
$15 million |
|
|
NASEM study related to organ donation and transplantation. |
$1.5 million |
|
|
Best Pharmaceuticals for Children Act research |
$25 million |
|
|
Investigation of Co-Occurring Conditions Across the Lifespan to Understand Down Syndrome (INCLUDE) |
$60 million |
|
|
NASEM study on long-term medical and economic impacts of the inclusion of women and racial minorities in clinical research. |
$1.2 million |
Source: U.S. Congress, House and Senate Committees on Appropriations, Subcommittee on the Departments of Labor, Health and Human Services, Education, and Related Agencies, Division A—Department H—Department of Labor, Health and Human Services, and Education and Related Agencies [LHHS] Appropriations Act, 20202021, committee print, 116th Cong., 2nd sess., December 21, 2020, pp. 44-71, 154-159. a. Amount likely includes $109 mil ion from the Innovation Account as authorized in the Cures Act. b. Amount likely includes $100 mil ion from the Innovation Account for the BRAIN Initiative as authorized by
the Cures Act (split between NINDS and NIMH in FY2021 appropriations).
Table A-3. Specified NIH Funding Levels in FY2022print, 116th Cong., 2nd sess., December 16, 2019, pp. 49-85, 187-189.
Notes: NASEM is the National Academies of Sciences, Engineering, and Medicine, private nonprofit institutions that advise on policy related to science, technology, and health. The predecessor organization, National Academy of Sciences, was created by congressional charter in 1863.
|
Program/Activity |
Amount |
|
Opioids and Pain Research |
$1.4 billion—$533 million for the Helping End Addiction Long-Term (HEAL) Initiative and more than $900 million to support ongoing research. |
|
Methamphetamine and Other Stimulant Use- developing medication-assisted treatment and evidence-based psychosocial treatment |
$50 million |
|
Childhood Cancer Data Initiative |
$50 million |
|
Centers for AIDS Research |
$16 million |
|
Influenza research |
$423 million—$200 million for developing a universal influenza vaccine |
|
Tick-borne diseases research |
$115 million |
|
Artificial Intelligence for Chronic Disease—utilizing artificial intelligence to deepen understanding of the underlying causes of chronic diseases and identify successful early treatments |
$50 million |
|
Gene Vector Production—creating a consortium with industry, academic, and federal stakeholders to increase the efficiency of vector production and speed up gene therapy clinical trials and treatments |
$30 million |
|
Ruth L. Kirschstein Institutional National Research Service Award Program |
$848 million |
|
IDeA States Pediatric Clinical Trials Network |
$15 million |
|
Neonatal research |
$100 million |
|
National Institute for Research on Safety and Quality (NIRSQ) Programs |
|
|
Health Services Research, Data, and Dissemination Research Portfolio |
$57 million |
|
Improving Maternal Health in America Initiative |
$7 million |
|
Patient Safety Research |
$60 million |
|
Medical Expenditure Panel Survey (MEPS) |
$72 million |
Appendix B.
Congressional Research Service
17
National Institutes of Health (NIH) Funding: FY1996-FY2022
Appendix B. Acronyms and Abbreviations
Acronym/
Abbreviation
Organization/Term
ARPA-H
Advanced Research Projects Agency for Health
DARPA
Defense Advanced Research Projects Agency
DOD
Department of Defense
FIC
Fogarty International Center
FY
Fiscal Year
IC
Institutes and Centers
NASEM
National Academies of Sciences, Engineering, Acronyms and Abbreviations
|
Organization/Term |
|
FIC |
Fogarty International Center |
|
FY |
Fiscal Year |
|
NASEM |
National Academies of Sciences, Engineering, and Medicine |
|
NCATS |
National Center for Advancing Translational Sciences |
|
NCCIH |
and Medicine
NCATS
National Center for Advancing Translational Sciences
NCCIH
National Center for Complementary |
|
NCI |
National Cancer Institute |
|
NEI |
National Eye Institute |
|
NHGRI |
National Human Genome Research Institute |
|
NHLBI |
National Heart, Lung, and Blood Institute |
|
NIA |
National Institute on Aging |
|
NIAAA |
National Institute on Alcohol Abuse and Alcoholism |
|
NIAID |
|
|
NIAMS |
National Institute of Arthritis |
|
NIBIB |
National Institute of Biomedical |
|
NICHD |
National Institute of Child Health and Human Development |
|
NIDA |
National Institute on Drug Abuse |
|
NIDCD |
National Institute on Deafness and Other Communication Disorders |
|
NIDCR |
National Institute of Dental and Craniofacial Research |
|
NIDDK |
National Institute of Diabetes and Digestive and Kidney Diseases |
|
NIEHS |
National Institute of Environmental Health Sciences |
|
NIGMS |
National Institute of General Medical Sciences |
|
NIMH |
National Institute of Mental Health |
|
NIMHD |
National Institute on Minority Health and Health Disparities |
|
NINDS |
National Institute of Neurological Disorders and Stroke |
|
NINR |
National Institute of Nursing Research |
|
NLM |
National Library of Medicine |
|
OD |
NIH Office of the Director |
Author Contact Information
Acknowledgments
CRS Research Assistant Isaac Nicchitta provided valuable assistance in analysis and writing for this report.
Footnotes
| 1. |
"Mandatory spending" is controlled by authorization acts; "discretionary spending" is controlled by appropriations acts. For further information, see CRS Report R44582, Overview of Funding Mechanisms in the Federal Budget Process, and Selected Examples. |
| 2. |
The Public Health Service also includes the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality (AHRQ), the Health Resources and Services Administration (HRSA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Indian Health Service (IHS), and the Agency for Toxic Substances and Disease Registry (ATSDR). |
| 3. |
For further information on The National Institutes of Health (NIH), see CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues. |
| 4. |
NIH, "What We Do- Budget," March 3, 2020, at https://www.nih.gov/about-nih/what-we-do/budget. |
| 5. |
Ibid. |
| 6. |
The Hazardous Substance Basic Research and Training Program (Superfund Research Program) funds research on the health effects of exposures to hazardous substances and related solutions at the National Institute of Environmental Health Sciences. It is authorized by 311(a) of the Comprehensive Environmental Response, Compensation, and Liability Act of 1980 (42 U.S.C. §9660(a)) and Section 126(g) of the Superfund Amendments and Reauthorization Act of 1986. |
| 7. |
For more information on the PHS Evaluation Tap, or PHS Evaluation Set-Aside, see discussion in CRS Report R44916, Public Health Service Agencies: Overview and Funding (FY2016-FY2018). |
| 8. |
See Section 204 of Division A of P.L. 116-94 for the FY2020 maximum set-aside level. The last time that an appropriations act set the PHS tap percentage at a level other than 2.5% was in FY2009, when it was 2.4% (see P.L. 111-8). The FY2020 omnibus also retained a change to this provision, first included in the FY2014 omnibus, allowing tap transfers to be used for the "evaluation and the implementation" of programs funded in the HHS title of the LHHS Appropriations Act. Prior to FY2014, such provisions had restricted tap funds to the "evaluation of the implementation" of programs authorized under the Public Health Service Act. |
| 9. |
See section on 21st Century Cures Act in CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues. |
| 10. |
CRS Report R45778, Exceptions to the Budget Control Act's Discretionary Spending Limits. |
| 11. |
P.L. 114-255, §1001. |
| 12. |
Except for the full FY2020 mandatory diabetes program extension, all FY2020 NIH funding was provided by the Further Consolidated Appropriations Act, 2020 (P.L. 116-94). |
| 13. |
The nonrecurring expenses fund (NEF) permits HHS to transfer unobligated balances of expired discretionary funds from FY2008 and subsequent years into the NEF account. The use of funds is authorized by law for capital acquisitions including information technology (IT) and facilities infrastructure (42 U.S.C. §3514a). |
| 14. |
This program level accounts for a transfer of $5 million from the Office of the Director to the HHS Office of the Inspector General (OIG). In addition, FY2021 budget request tables do not reflect the Nonrecurring Expenses Fund transfer of $225 million to NIH in the FY2020 program level, as directed by P.L. 116-94. |
| 15. |
NIH, Congressional Justification: FY2021, February 10, 2020, p. 75, at https://officeofbudget.od.nih.gov/pdfs/FY21/br/1-OverviewVolumeSingleFile-toPrint.pdf. |
| 16. |
P.L. 116-94 directed a transfer of $225 million from the HHS Nonreccurring Expenses Fund to the NIH Buildings and Facilities account in FY2020-enacted appropriations. However, this transfer is not reflected in the budget tables of the NIH FY2021 Congressional Justification. |
| 17. |
Letter from Michael R. Pence, President of the Senate, to Donald Trump, President of the United States, March 17, 2020, at https://www.whitehouse.gov/wp-content/uploads/2020/03/Letter-regarding-additional-funding-to-support-the-United-States-response-to-COVID-19-3.17.2020.pdf. |
| 18. |
For more information about the Patient-Centered Outcomes Research Trust Fund, see CRS Insight IN11010, Funding for ACA-Established Patient-Centered Outcomes Research Trust Fund (PCORTF) Extended Through FY2029. |
| 19. |
See NIH sections of CRS Report R44888, Federal Research and Development Funding: FY2018; CRS Report R45150, Federal Research and Development (R&D) Funding: FY2019; and CRS Report R45715, Federal Research and Development (R&D) Funding: FY2020. |
| 20. |
CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues. |
| 21. |
|
| 22. |
For instance, the FY2006 total was 0.1% lower than the previous year, the first time that NIH appropriations had decreased since FY1970; the FY2011 total, provided in the Full-Year Continuing Appropriations Act, 2011 (P.L. 112-10), was 1.0% below the previous fiscal year; the FY2013 total, provided in the Consolidated and Further Continuing Appropriations Act, 2013 (P.L. 113-6), was reduced by the March 2013 sequestration and a transfer of funding under the authority of the HHS Secretary ($1.553 billion and $173 million, respectively), resulting in a budget that was 5.0% lower than the prior year. |
| 23. |
The index is developed for NIH by the Bureau of Economic Analysis of the Department of Commerce. It reflects the increase in prices of the resources needed to conduct biomedical research, including personnel services, supplies, and equipment. It indicates how much the NIH budget must change to maintain purchasing power. See "NIH Price Indexes," at https://officeofbudget.od.nih.gov/gbiPriceIndexes.html. |
| 24. |
CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues. |