National Institutes of Health (NIH) Funding: FY1996-FY2026
Changes from April 4, 2019 to January 22, 2020
This page shows textual changes in the document between the two versions indicated in the dates above. Textual matter removed in the later version is indicated with red strikethrough and textual matter added in the later version is indicated with blue.
National Institutes of Health (NIH) Funding: FY1994-FY2020
Contents
- NIH Funding: FY1994-FY2020
- Funding Sources
- Trends
- FY2020 Budget Request
- Trends
NIH Funding: FY1994-FY2020
The National Institutes of Health (NIH) is the primary federal agency charged with conducting and supporting biomedicalfor medical, health, and behavioral research. It is the largest of the eight health-related agencies that make up the Public HealthHealth Service (PHS) within the Department of Health and Human Services (HHS).1 NIH's organization consists of the Office of the Director (OD) and 27 Institutes and Centers (ICs) that focus on aspects of health, human development, and biomedical science. The OD sets overall policy for NIH and coordinates the programs and activities of all NIH components, particularly in areas of research that involve multiple institutes.
NIH activities cover a wide range of basic, clinical, and translational research, focused on particular diseases, areas of human health and development, or more fundamental aspects of biology and behavior. Its mission also includes research training and health information collection and dissemination.2 More than 80% of the NIH budget funds extramural research (i.e., external) through grants, contracts, and other awards.3 This funding supports research performed by more than 300,000 individuals who work at over 2,500 hospitals, medical schools, universities, and other research institutions around the country.4 About 10% of the agency's budget supports intramural research (i.e., internal) conducted by nearly 6,000 NIH physicians and scientists, most of whom are located on the NIH campus in Bethesda, MD.5
Funding Sources
Funding for NIH comes primarily from the annual Labor, HHS, and Education (LHHS) appropriations bill, with an additional smaller amount for the Superfund Research Programamount for Superfund-related activities from the Interior/Environment appropriations bill..6 Those two bills provide NIH's discretionary budget authority.6 7
In addition, NIH has received mandatory funding of $150 million annually that is provided in Public Health Service Act (PHSA), Section 330B, for a special program on type 1 diabetes research, though under current law, no new funding will be available for this program after September 30, 2019.7 Some funding is also transferred to NIH pursuant to the "PHS Evaluation Tap" Transfer authority.8 The total funding available for NIH activities, taking account of add-ons and PHS tap transfers, is known as the NIH program level.9
Trends
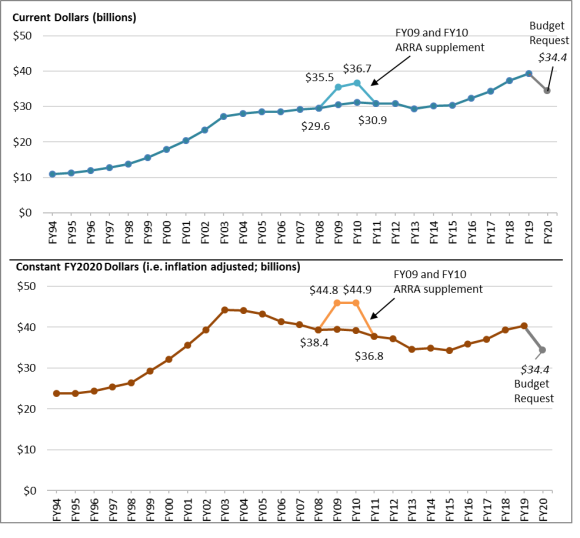
Table 1 outlines NIH program level funding over the past 25 years, and Figure 1 illustrates funding trends in both current (also called nominal dollars) and projected constant (i.e., inflation-adjusted) FY2020 dollars.
NIH has seen periods of high and low funding growth. Between FY1994 and FY1998, funding for NIH grew from $11.0 billion to $13.7 billion in nominal terms. Over the next five years, Congress and the President doubled the NIH budget to $27.2 billion in FY2003. In each of these years, NIH received annual funding increases of 14% to 16%. Since FY2003, NIH funding has increased more gradually in nominal dollars. Funding peaked in FY2010 before declining in FY2011 through FY2013, with increases in subsequent years.10 In some years, (FY2006, FY2011, and FY2013) funding for the agency decreased in nominal dollars.11 From FY2016 through FY2019, the NIH has seen funding increases of over 5% each year. The largest increase was from FY2017 to FY2018, where the program level increased by $3.0 billion (+8.7%), making this the largest single-year nominal dollar increase since FY2003 (excluding one-time funds provided by the American Recovery and Reinvestment Act of 2009 [ARRA, P.L. 111-5]).
|
The 21st Century Cures Act and the NIH Innovation Account The 21st Century Cures Act ("the Cures Act," P.L. 114-255) created the NIH Innovation account and specified that funds in the account must be appropriated in order to be available for expenditure. The Cures Act specified that the following amounts shall be transferred to the NIH Innovation account: $352 million for FY2017; $496 million for FY2018; $711 million for FY2019; $492 million for FY2020; $404 million for FY2021; $496 million for FY2022; $1,085 million for FY2023; $407 million for FY2024; $127 million for FY2025; and $226 million for FY2026. All amounts authorized by the Cures Act have been fully appropriated from FY2017 to FY2019.12 President Trump's FY2020 budget request requested the full amount authorized by the Cures Act for FY2020. For further information, see CRS Report R44720, The 21st Century Cures Act (Division A of P.L. 114-255). |
For FY2019, the NIH has a program level total of $39.308 billion. Under the LHHS appropriations act (H.R. 6157, P.L. 115-245), NIH received $37.933 billion in discretionary LHHS budget authority, including amounts authorized by the 21st Century Cures Act (see text box).13 Adding to this total the amounts for the evaluation tap ($1.147 billion), the mandatory type 1 diabetes program ($150 million), and Superfund related activities ($79 million)14 brings the program-level total to $39.308 billion. This program level provides the NIH with $2 billion (5.4%) more than the FY2018 program level and $4.52 billion (13.0%) more than President Trump's FY2019 budget request for the NIH. This program level is $744 million (1.9%) more than the House committee recommendation15 but is close to the earlier Senate-passed program level recommendation.16
The lower half of Figure 1 portrays NIH funding adjusted for inflation (in projected constant FY2020 dollars) using the Biomedical Research and Development Price Index (BRDPI).17 It shows that the purchasing power of NIH funding (non-ARRA) peaked in FY2003 (the last year of the five-year doubling period) and then fairly steadily declined for more than a decade (excluding ARRA) until back-to-back funding increases were provided in FY2016, FY2017, FY2018, and FY2019.
FY2020 Budget Request
President Trump's FY2020 budget request would provide NIH a total program level of $34.368 billion, a decrease of $4.941 billion (-12.6%) compared with FY2019-enacted levels.18 The proposed FY2020 program level total would include
- $33.410 billion provided through LHHS appropriations (including the full amount authorized by the Cures Act),
- $741 million from the PHS evaluation transfer,
- $66.581 million provided through Interior/Environment appropriations for Superfund-related activities, and
- $150 million in proposed funding for the mandatory type 1 diabetes program.
In addition, the FY2020 Budget Request proposes consolidating the Agency for Healthcare Research and Quality (AHRQ) into NIH, forming a 28th IC—the National Institute for Research on Safety and Quality (NIRSQ). The creation of a new NIH institute would require an amendment to the PHSA Section 401(d), which specifies that "[i]n the National Institutes of Health, the number of national research institutes and national centers may not exceed a total of 27."
Under the FY2020 budget proposal, all the existing ICs and budget activity lines, except for Buildings and Facilities, would receive a decrease compared to FY2019-enacted levels.19 The Buildings and Facilities appropriation of $200 million would not change from FY2019 to FY2020. NISRQ would receive $256 million in funding for FY2020. The budget request also aims to reduce the direct cost of research by proposing a cap on the percentage of an investigator's salary that can be paid with NIH grant funds at 90%.
As shown in Table 1, the proposed FY2020 program level would be 22.4% less than the FY2003 program level (peak funding year), in constant FY2020 dollars.
Program Level Funding in Current and Projected Constant (FY2020) Dollars. | |
 | |
Some funding is also transferred to NIH pursuant to the PHS Evaluation Set-Aside or the "PHS Evaluation Tap" Transfer authority.9 Authorized by Section 241 of the Public Health Service Act, the evaluation tap allows the Secretary of HHS, with the approval of appropriators, to redistribute a portion of eligible PHS agency appropriations across HHS for program evaluation and implementation purposes. The PHSA section limits the set-aside to not less than 0.2% and not more than 1% of eligible program appropriations. However, LHHS appropriations acts have commonly established a higher maximum percentage for the set-aside and have distributed specific amounts of "tap" funding to selected HHS programs. Since FY2010, and including in FY2020, this higher maximum set-aside level has been 2.5% of eligible appropriations.10 The total funding available for NIH activities, taking account of add-ons and PHS tap transfers, is referred to as the NIH program level.11 Under the Administration's FY2020 budget proposal, all the existing ICs and budget activity lines, except for Buildings and Facilities, would have received a decrease compared with FY2019-enacted levels.13 The Buildings and Facilities appropriation of $200 million would not have changed from FY2019 to FY2020. The proposed NIRSQ would have received $256 million in funding for FY2020. The budget request also aimed to reduce the direct cost of research by proposing a cap on the percentage of an investigator's salary that can be paid with NIH grant funds at 90%.14 The Senate did not complete committee or floor consideration of FY2020 LHHS appropriations. The majority of the Senate Appropriations Committee, however, released a draft bill and a draft committee report.17 Separately, the Senate Appropriations Committee passed an FY2020 Interior/Environment bill with funding for the Superfund Research Program (S. 2580). On December 20, 2019, Congress and the President mostly finalized the FY2020 NIH program level (except for full-year type 1 diabetes funding) by enacting the Further Consolidated Appropriations Act, 2020 (P.L. 116-94), which included final FY2020 LHHS appropriations in Division A, Interior/Environment appropriations in Division D, and a temporary extension for the special diabetes program for type 1 diabetes through May 22, 2020. The enacted FY2020 NIH program level is made up of the following: Congress did not adopt the Administration's proposals to consolidate AHRQ into NIH or to cap the percentage of an investigator's salary that can be paid with NIH grant funds at 90%. Congress did not adopt similar proposals by the Administration in FY2017 through FY2019.19 NIH has seen periods of high and low funding growth. Between FY1994 and FY1998, funding for NIH grew from $11.0 billion to $13.7 billion (nominal dollars). Over the next five years, Congress and the President doubled the NIH budget to $27.2 billion in FY2003. In each of FY1999 through FY2003, NIH received annual funding increases of 14% to 16%. From FY2003 to FY2015, NIH funding increased more gradually in nominal dollars.20 In some years, (FY2006, FY2011, and FY2013) funding for the agency decreased in nominal dollars.21 From FY2016 through FY2020, the NIH has seen funding increases of over 5% each year. The largest increase was from FY2017 to FY2018, where the program level increased by $3.0 billion (+8.7%), making this the largest single-year nominal dollar increase since FY2003 (excluding one-time funds provided by the American Recovery and Reinvestment Act of 2009 [ARRA, P.L. 111-5]). The 21st Century Cures Act and the NIH Innovation Account The 21st Century Cures Act ("the Cures Act," P.L. 114-255) created a new NIH Innovation account for funding programs authorized by the act. For appropriated amounts to the account—up the limit authorized for each fiscal year—the amounts are subtracted from any cost estimate for enforcing the discretionary spending limit for each fiscal year (i.e., the budget caps). In effect, appropriations to the NIH Innovation Account as authorized by the Cures Act are not subject to discretionary spending limits. The NIH Director may transfer these amounts from the NIH Innovation account to other NIH accounts but only for the purposes specified in the Cures Act. If the NIH Director determines that the funds for any of the four Innovation Projects are not necessary, the amounts may be transferred back to the NIH Innovation account. The Cures Act specified that the following amounts shall be transferred to the NIH Innovation account: $352 million for FY2017; $496 million for FY2018; $711 million for FY2019; $492 million for FY2020; $404 million for FY2021; $496 million for FY2022; $1,085 million for FY2023; $407 million for FY2024; $127 million for FY2025; and $226 million for FY2026. All amounts authorized by the Cures Act have been fully appropriated from FY2017 to FY2020.22 For further information, see CRS Report R44720, The 21st Century Cures Act (Division A of P.L. 114-255), and CRS Report R45778, Exceptions to the Budget Control Act's Discretionary Spending Limits.
Program Level Funding in Current and Projected Constant (FY2020) Dollars. Notes: By convention, program level totals include amounts "transferred in" pursuant to PHS tap, but do not include any amounts "transferred out" under this same authority. Program level includes all budget authority, including appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002-FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. ARRA supplementary funding is from the American Recovery and Reinvestment Act of 2009, P.L. 111-5. In general, amounts provided to NIH for emergency requirements are excluded from these totals (e.g., FY2015 amount does not include $238 million for the NIAID for research on Ebola that was provided in P.L. 113-235, Title VI of Division G). |
Table 1. NIH Funding, FY1994-FY2020
Program Level Funding in Current and Constant (FY2020) Dollars (billions)
|
Fiscal Year |
Program Level Current $ |
% Change |
Program Level Projected Constant FY2020 $ |
% Below FY2003a |
|
1994 |
$10.956 |
$23.817 |
||
|
1995 |
11.300 |
3.1% |
23.741 |
|
|
1996 |
11.928 |
5.6% |
24.436 |
|
|
1997 |
12.741 |
6.8% |
25.395 |
|
|
1998 |
13.675 |
7.3% |
26.363 |
|
|
1999 |
15.629 |
14.3% |
29.206 |
|
|
2000 |
17.841 |
14.1% |
32.141 |
|
|
2001 |
20.459 |
14.7% |
35.671 |
|
|
2002 |
23.321 |
14.0% |
39.359 |
|
|
2003 |
27.167 |
16.5% |
44.292 |
|
|
2004 |
28.037 |
3.2% |
44.069 |
-0.5% |
|
2005 |
28.594 |
2.0% |
43.262 |
-2.3% |
|
2006 |
28.560 |
-0.1% |
41.299 |
-6.8% |
|
2007 |
29.179 |
2.2% |
40.650 |
-8.2% |
|
2008 |
29.607 |
1.5% |
39.403 |
-11.0% |
|
2009 |
30.545 |
3.2% |
39.495 |
-10.8% |
|
2010 |
31.238 |
2.3% |
39.199 |
-11.5% |
|
2011 |
30.916 |
-1.0% |
37.716 |
-14.8% |
|
2012 |
30.861 |
-0.2% |
37.173 |
-16.1% |
|
2013 |
29.316 |
-5.0% |
34.662 |
-21.7% |
|
2014 |
30.143 |
2.8% |
34.891 |
-21.2% |
|
2015 |
30.311 |
0.6% |
34.386 |
-22.4% |
|
2016 |
32.311 |
6.6% |
35.875 |
-19.0% |
|
2017 |
34.301 |
6.2% |
37.119 |
-16.2% |
|
2018 |
37.311 |
8.8% |
39.353 |
-11.2% |
|
2019 |
39. |
5.4% |
40. |
-8. |
|
2020 |
34.368 |
|
34.368 |
- |
|
NIH Funding Including ARRA Supplement |
||||
|
2009 |
35.499 |
$46.02 |
||
|
2010 |
36.684 |
$46.15 |
||
Source: NIH Budget Office, Appropriations History by Institute/Center (1938 to Present), at http://officeofbudget.od.nih.gov/approp_hist.html. The FY2019 and F2020 program levels are based on budget data from NIH, "Justification of Estimates for Appropriations Committees FY2020--Overview, Vol. 1," p. 78, except for FY2019 appropriations to NIEHS throughU.S. Congress, House and Senate Committees on Appropriations, Subcommittee on the Departments of Labor, Health and Human Services, Education, and Related Agencies, Division A--Department of Labor, Health and Human Services, and Education and Related Agencies [LHHS] Appropriations Act, 2020, committee print, 116th Cong., 2nd sess., December 16, 2019, pp. 187-189, with Superfund research program amounts from Title III of Division E from the Consolidated Appropriations Act, 2019 (P.L. 116-6) and from Title III of Division D from the Further Consolidated Appropriations Act, 2020 (P.L. 116-94). Inflation adjustment reflects the Biomedical Research and Development Price Index (BRDPI), updated January 2019, https://officeofbudget.od.nih.gov/gbiPriceIndexes.html.
Notes: By convention, budget tables, such as Table 1, include amounts "transferred in" pursuant to PHS tap, but do not include any amounts "transferred out" under this same authority. Program level includes all budget authority, including appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002-FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. ARRA supplementary funding is from the American Recovery and Reinvestment Act of 2009, P.L. 111-5. In general, amounts provided to NIH for emergency requirements are excluded from these totals (e.g., FY2015 amount does not include $238,000,000 for the NIAID for research on Ebola that was provided in P.L. 113-235, Title VI of Division G).
a. FY2003 was the peak funding year for the NIH program level.
b. PB means "President's Budget."
Author Contact Information
(budget authority, in millions of dollars)
Institutes/Centers
Cancer Institute (NCI)
$6,144
$5,247
$6,444
—
$6,440
Heart, Lung, and Blood Institute (NHLBI)
$3,488
$3,003
$3,659
—
$3,624
Dental/Craniofacial Research (NIDCR)
$462
$397
$484
—
$477
$2,030
$1,746
$2,129
—
$2,114
Neurological Disorders/Stroke (NINDS)
$2,274
$2,026
$2,386
—
$2,445
Allergy/Infectious Diseases (NIAID)
$5,523
$4,754
$5,808
—
$5,885
$1,726
$1,732
$1,886
—
$1,706
Child Health/Human Development (NICHD)
$1,506
$1,297
$1,580
—
$1,557
National Eye Institute (NEI)
$797
$686
$835
—
$824
$775
$667
$813
—
$803
National Institute on Aging (NIA)
$3,083
$2,654
$3,286
—
$3,544
Arthritis/Musculoskeletal/Skin Diseases (NIAMS)
$605
$521
$635
—
$625
Deafness/Communication Disorders (NIDCD)
$474
$408
$498
—
$491
National Institute of Mental Health (NIMH)
$1,870
$1,630
$1,962
—
$2,038
National Institute on Drug Abuse (NIDA)
$1,420
$1,296
$1,489
—
$1,462
Alcohol Abuse/Alcoholism (NIAAA)
$526
$452
$551
—
$545
Nursing Research (NINR)
$163
$140
$171
—
$169
Human Genome Research Institute (NHGRI)
$576
$495
$604
—
$606
Biomedical Imaging/Bioengineering (NIBIB)
$389
$336
$408
—
$404
Minority Health/Health Disparities (NIMHD)
$315
$271
$341
—
$336
Complementary/Integrative Health (NCCIH)
$146
$126
$154
—
$152
Advancing Translational Sciences (NCATS)
$806
$694
$846
—
$833
Fogarty International Center (FIC)
$78
$67
$85
—
$81
National Library of Medicine (NLM)
$442
$380
$464
—
$457
$1,922
$1,769
$2,063
—
$2,252
$196
$157
$157
—
$157
Buildings and Facilities (B&F)
$200
$200
$200
—
$200
—
$256
—
—
—
Subtotal, NIH (LHHS Discretionary BA, non-transfer)
$37,937
$33,410
$39,937
—
$40,228
PHS Program Evaluation (provided to NIGMS)
$1,147
$741
$1,147
—
$1,231
Nonrecurring Expenses Fund (NEF) Transfer
—
—
—
—
$225
$79
$67
$80
$81
$81
$150
$150
$150
—
$150
NIH Program Level
$39,313
$34,368
$41,314
—
$41,915
Source: U.S. Congress, House and Senate Committees on Appropriations, Subcommittee on the Departments of Labor, Health and Human Services, Education, and Related Agencies, Division A--Department of Labor, Health and Human Services, and Education and Related Agencies [LHHS] Appropriations Act, 2020, committee print, 116th Cong., 2nd sess., December 16, 2019, pp. 187-189, and H.Rept. 116-62, pp. 332-334, except as noted below.
Notes: Totals may differ from the sum of the components due to rounding. Amounts in table may differ from actuals in many cases. By convention, budget tables such as Table A-1 do not subtract the amount of transfers to the evaluation tap from the agencies' appropriation. a. The Senate did not complete committee or floor consideration of FY2020 LHHS appropriations. The majority, however, released a draft bill and a draft committee report. Separately, the Senate Appropriations Committee passed an Interior/Environment bill with funding for the Superfund Research Program (S. 2580). b. Amounts for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) do not include mandatory funding for type 1 diabetes research (see note h). c. Amounts for National Institute of General Medical Sciences (NIGMS) do not include funds from PHS Evaluation Set-Aside (§241 of the PHS Act). Though the budget request would have provided an increase to NIGMS through discretionary LHHS budget authority compared to FY2019, the total amount for NIGMS with the PHS evaluation transfer included is less than FY2019-enacted levels. The FY2020 NIGMS amount is similarly higher than the FY2019-enacted level when accounting for the PHS Evaluation Set-Aside. d. Amounts for National Institute of Environmental Health Sciences (NIEHS) do not include Interior/Environment Appropriations amount for Superfund research (see note g). e. Includes $12.6 million for the Gabriella Miller Kids First Research Act. f. The amount shown for the NIH Innovation Account in each column represents only a portion ($196 million for FY2019, $157 million for FY2020) of the total appropriation to the account ($711 million for FY2019, $492 million for FY2020). The remaining funds for this account are incorporated, where applicable, into the totals for other ICs. For the FY2020, this includes $195 to NCI for cancer research and $70 million to each of NINDS and NIMH for the BRAIN Initiative. g. Amount for an NIRSQ proposed by the Trump Administration does not include the estimated $112.5 million in mandatory funding transfers from the Patient-Centered Outcomes Research Trust Fund (PCORTF) in FY2019, which were provided outside of the annual appropriations process. h. This is a separate account in the Interior/Environment appropriations for National Institute of Environmental Health Sciences (NIEHS) research activities related to Superfund research. The FY2019-enacted amount is from Title III of Division E from the Consolidated Appropriations Act, 2019 (P.L. 116-6); the House-proposed FY2020 amount is from House-passed Department of the Interior, Environment, and Related Agencies Appropriations Act, 2020 (H.R. 3055); the Senate committee amount is from Department of the Interior, Environment, and Related Agencies Appropriations Act, 2020 (S. 2580); and the FY2020 amount is from Title III of Division D from the Further Consolidated Appropriations Act, 2020 (P.L. 116-94). i. Mandatory funds are available to NIDDK for type 1 diabetes research under PHSA Section 330Bm were provided by Section 50902 of P.L. 115-123 for FY2018 and FY2019, specified at $150 million annually. For FY2020, several temporary extensions of the funding have been provided in FY2020 continuing resolutions (P.L. 116-59, P.L. 116-69) and most recently in Section 402 of Division N, Title I, Health and Human Services Extenders in P.L. 116-94, which provided $96.6 million in funding for the program until May 22, 2020. Several legislative proposals have been introduced to extend the program (some propose increased program funding), but none have been enacted. Cited FY2020 budget documents show $150 million as the FY2020 funding level, and therefore CRS uses this amount for budget analysis.Program Funding from FY2020 Explanatory Statement
In recent years, Congress has increasingly used language in reports and explanatory statements accompanying appropriations bills to designate funding for specific research areas, activities, or programs at NIH. For the most part, Congress does not specify funding for designated purposes and allows the ICs to allocate program funding through various agency mechanisms.24 In some cases, Congress uses report language to specify a certain amount of IC funding for a designated purpose, as summarized in Table A-2.Sometimes the report language specifies that "no less than" a certain amount can be designated for a certain purpose; in other cases, report language "provides" or "recommends" that an amount be spent on a certain purpose. While the House report (H.Rept. 116-62) also included funding levels for some of the below programs, the amounts in the explanatory statement supersede those. Both the explanatory statement and the House report include many additional statements directing the agency to prioritize certain programs or areas of research, as well as expressing the opinion or concerns of Congress regarding NIH; these broad statements are not summarized here.
Table A-2. Specified NIH Funding Levels in FY2020 Explanatory StatementInstitute
Program
Amount
Cancer Institute (NCI)
Childhood cancer data initiative
$50 million
Additional cancer research awards
$212.5 million
Childhood Cancer Survivorship, Treatment Access, and Research (STAR) Act
$25 million
Neurological Disorders/Stroke (NINDS)
Opioid misuse and addiction
$250 million
Allergy/Infectious Diseases (NIAID)
AIDS2020 Conference (International AIDS Conference)
$5.1 million
Combating antimicrobial resistance (AMR)
$511 million, an increase of $50 million
NASEM study on the long-term medical and economic impacts of increased AMR in the United States
$1.7 million
HIV/AIDS research
an increase of no less than $25 million over FY2019 level
Centers for AIDS Research
$51 million
Universal flu vaccine
$200 million, an increase of $60 million
General Medical Sciences (NIGMS)
Institutional Development Award (IDeA) Program
$386.6, an increase of $25 million
Environmental Health Sciences (NIEHS)
Hurricane Harvey research
$3 million
Aging (NIA)
Alzheimer's disease and related dementias
Increase of $350 million; total funding no less than $2.818 billion
Drug Abuse (NIDA)
Opioid misuse and addiction
$250 million
Genome Research (NHGRI)
Emerging Centers of Excellence in Genomic Sciences
$10 million
Minority Health/Health Disparities (NIMHD)
Research Centers in Minority Institutions
$75 million
Advancing Translational Sciences (NCATS)
Clinical and Translational Science Awards (CTSAs)
$578.1 million
Cures Acceleration Network
up to $60 million
Office of the Director (OD)/ Multi-Institute Research Initiatives
NASEM study of NIH research on autoimmune conditions that predominately affect women.
$1.5 million
Big data- Chief Data Strategist's work
$30 million
Grants for biomedical research facilities
$50 million
Firearm injury and mortality prevention research
$12.5 million
HHS Office of National Security allocation for foreign threats program
$5 million
Environmental Influences on Child Health Outcomes Program
$15 million
Best Pharmaceuticals for Children Act research
$25 million
Investigation of Co-Occurring Conditions Across the Lifespan to Understand Down Syndrome (INCLUDE)
$60 million
NASEM study on long-term medical and economic impacts of the inclusion of women and racial minorities in clinical research.
$1.2 million
Source: U.S. Congress, House and Senate Committees on Appropriations, Subcommittee on the Departments of Labor, Health and Human Services, Education, and Related Agencies, Division A--Department of Labor, Health and Human Services, and Education and Related Agencies [LHHS] Appropriations Act, 2020, committee print, 116th Cong., 2nd sess., December 16, 2019, pp. 187-189.
Notes: NASEM ia the National Academies of Sciences, Engineering, and Medicine, private nonprofit institutions that advise on policy related to science, technology, and health. The predecessor organization, National Academy of Sciences, was created by congressional charter in 1863.
Organization/Term
FIC
Fogarty International Center
FY
Fiscal Year
NASEM
National Academies of Sciences, Engineering, and Medicine
NCATS
National Center for Advancing Translational Sciences
NCCIH
National Center for Complementary and Integrative Health
NCI
National Cancer Institute
NEI
National Eye Institute
NHGRI
National Human Genome Research Institute
NHLBI
National Heart, Lung, and Blood Institute
NIA
National Institute on Aging
NIAAA
National Institute on Alcohol Abuse and Alcoholism
NIAID
National Institute of Allergy and Infectious Diseases
NIAMS
National Institute of Arthritis and Musculoskeletal and Skin Diseases
NIBIB
National Institute of Biomedical Imaging and Bioengineering
NICHD
National Institute of Child Health and Human Development
NIDA
National Institute on Drug Abuse
NIDCD
National Institute on Deafness and Other Communication Disorders
NIDCR
National Institute of Dental and Craniofacial Research
NIDDK
National Institute of Diabetes and Digestive and Kidney Diseases
NIEHS
National Institute of Environmental Health Sciences
NIGMS
National Institute of General Medical Sciences
NIMH
National Institute of Mental Health
NIMHD
National Institute on Minority Health and Health Disparities
NINDS
National Institute of Neurological Disorders and Stroke
NINR
National Institute of Nursing Research
NLM
National Library of Medicine
OD
NIH Office of the Director
Author Contact Information
Footnotes
| 1. |
The Public Health Service also includes the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality (AHRQ), the Health Resources and Services Administration (HRSA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Indian Health Service (IHS), and the Agency for Toxic Substances and Disease Registry (ATSDR). |
||||||||||||||||||
| 2. |
For further information on NIH, see CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues. |
||||||||||||||||||
| 3. |
Department of Health and Human Services, Fiscal Year 2018 Budget in Brief, Washington, DC, May 2017, p. 38. Updated numbers were not available in the FY2019 or FY2020 HHS Budget in Brief. |
||||||||||||||||||
| 4. |
Ibid. |
||||||||||||||||||
| 5. |
Ibid. |
||||||||||||||||||
| 6. |
The Hazardous Substance Basic Research and Training Program (Superfund Research Program) funds research on the health effects of exposures to hazardous substances and related solutions at the National Institute of Environmental Health Sciences. It is authorized by 311(a) of the Comprehensive Environmental Response, Compensation, and Liability Act of 1980 (42 U.S.C. 9660(a)) and Section 126(g) of the Superfund Amendments and Reauthorization Act of 1986.
|
||||||||||||||||||
|
42 U.S.C. §254c-3. |
|||||||||||||||||||
|
For more information on the PHS Evaluation Tap, or PHS Evaluation Set-Aside, see discussion in CRS Report R44916, Public Health Service Agencies: Overview and Funding (FY2016-FY2018). |
|||||||||||||||||||
| 9. |
Totals include amounts "transferred in" pursuant to PHS tap, but do not include any amounts "transferred out" under this same authority. |
||||||||||||||||||
|
|
See §204 of Division A of P.L. 116-94 for the FY2020 maximum set-aside level. The last time that an appropriations act set the PHS tap percentage at a level other than 2.5% was in FY2009, when it was 2.4% (see P.L. 111-8). The FY2020 omnibus also retained a change to this provision, first included in the FY2014 omnibus, allowing tap transfers to be used for the "evaluation and the implementation" of programs funded in the HHS title of the LHHS appropriations act. Prior to FY2014, such provisions had restricted tap funds to the "evaluation of the implementation" of programs authorized under the Public Health Service Act. 11.
|
|
Totals include amounts "transferred in" pursuant to PHS tap, but do not include any amounts "transferred out" under this same authority. 12.
|
|
NIH, "Justification of Estimates for Appropriations Committees--Overview FY2020, Vol. 1," p. 78. 13.
|
Though the budget request provides an increase to the National Institute of General Medical Sciences (NIGMS) through discretionary LHHS budget authority, the total amount for NIGMS with the PHS evaluation transfer included is less than FY2019-enacted levels. For proposed FY2020 IC funding levels see Table A-1.
14.
|
|
NIH, "Justification of Estimates for Appropriations Committees--Overview FY2020, Vol. 1." 15.
|
|
The Labor, Health and Human Services, Education, Defense, State, Foreign Operations, and Energy and Water Development Appropriations Act, 2020. 16.
|
|
Commerce, Justice, Science, Agriculture, Rural Development, Food and Drug Administration, Interior, Environment, Military Construction, Veterans Affairs, Transportation, and Housing and Urban Development Appropriations Act, 2020. 17.
|
|
CRS Insight IN11114, FY2020 LHHS Appropriations: Status. 18.
|
|
The nonrecurring expenses fund (NEF) permits HHS to transfer unobligated balances of expired discretionary funds from FY2008 and subsequent years into the NEF account. Congress authorized use of the funds for capital acquisitions including information technology (IT) and facilities infrastructure (42 U.S.C. §3514a). 19.
|
|
For further background, see NIH sections of CRS Report R44516, Federal Research and Development Funding: FY2017; CRS Report R44888, Federal Research and Development Funding: FY2018; and CRS Report R45150, Federal Research and Development (R&D) Funding: FY2019. |
Amounts shown in Table 1 include appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002-FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. For further details on the amounts transferred out by fiscal year, see the "Supplemental Appropriation Data Table" for "History of Congressional Appropriations, Fiscal Years 2000-2012" at http://officeofbudget.od.nih.gov/approp_hist.html. |
|
For instance, the FY2006 total was 0.1% lower than the previous year, the first time that the NIH appropriation had decreased since FY1970; the FY2011 total, provided in the Full-Year Continuing Appropriations Act, 2011 (P.L. 112-10), was 1.0% below the previous fiscal year; and the FY2013 total, provided in the Consolidated and Further Continuing Appropriations Act, 2013 (P.L. 113-6), was reduced by the March 2013 sequestration and a transfer of funding under the authority of the HHS Secretary ($1.553 billion and $173 million, respectively), resulting in a budget that was 5.0% lower than the prior year. |
|||||||||||||||||||
|
The first round of funding was provided by Section 194 of the Further Continuing and Security Assistance Appropriations Act, 2017 (CR, P.L. 114-254). The CR appropriated $352 million in the NIH Innovation account for necessary expenses to carry out the four NIH Innovation Projects as described in Section 1001(b)(4) of the Cures Act. The second round of funding was provided by the FY2018 omnibus (P.L. 115-141). The third round of funding | |||||||||||||||||||
| 13. |
NIH, "Justification of Estimates for Appropriations Committees- Overview FY2020, Vol. 1," p. 78. |
||||||||||||||||||
| 14. |
Provided by P.L. 116-6, Consolidated Appropriations Act, 2019. |
||||||||||||||||||
| 15. |
The House appropriations committee recommendations provide for an NIH program level total of $38.564 billion, calculated from figures in H.Rept. 115-952, pp. 573-575, and using the House Superfund appropriations recommendation of $80 million to NIEHS from H.Rept. 115-765, p. 82. |
||||||||||||||||||
| 16. |
The Senate appropriations committee recommendations provide for an NIH program level total of $39.312 billion, calculated from figures in H.Rept. 115-952, pp. 573-575, and using the Senate Superfund appropriations recommendation of $78 million to NIEHS from S.Rept. 115-276, p. 95. |
||||||||||||||||||
|
The index is developed for NIH by the Bureau of Economic Analysis of the Department of Commerce. It reflects the increase in prices of the resources needed to conduct biomedical research, including personnel services, supplies, and equipment. It indicates how much the NIH budget must change to maintain purchasing power. See "NIH Price Indexes," at https://officeofbudget.od.nih.gov/gbiPriceIndexes.html. |
|||||||||||||||||||
CRS Report R41705, The National Institutes of Health (NIH): Background and Congressional Issues |
NIH, "Justification of Estimates for Appropriations Committees--Overview FY2020, Vol. 1," p. 78. |
||||||||||||||||||
| 19. | Though the budget request provides an increase to NIGMS through discretionary LHHS budget authority, the total amount for NIGMS with the PHS evaluation transfer included is less than FY2019-enacted levels. For proposed FY2020 IC funding levels see NIH, "Justification of Estimates for Appropriations Committees- Overview, Vol. 1," p. 78. |