The National Health Service Corps
Changes from April 26, 2018 to January 4, 2022
This page shows textual changes in the document between the two versions indicated in the dates above. Textual matter removed in the later version is indicated with red strikethrough and textual matter added in the later version is indicated with blue.
Contents
- Introduction
- Program Overview
- Federal Scholarship Program
- Federal Loan Repayment Program
- Federal Students to Service (S2S) Loan Repayment Program
- Zika Loan Repayment Program
- State Loan Repayment Program
- NHSC Funding
- Program Size
- Recruitment
- Field Strength
- Types of NHSC Providers
- Legislative Proposals to Expand NHSC Provider Eligibility
- Administrative Authority to Expand NHSC Provider Eligibility
- NHSC Provider Locations
- Provider Retention
Figures
Summary
The National Health Service Corps January 4, 2022 The National Health Service Corps (NHSC) provides scholarships and loan repayments to health care providers in exchange for a period of service in a health professional shortage area (HPSA). Elayne J. Heisler The program places clinicians at facilities—generally not-for-profit or government-operated— Specialist in Health that might otherwise have difficulties recruiting and retaining providers.
The program’s clinicians Services provided care to an estimated 23.6 million patients in 2021. The NHSC is administered by the Health Resources and Services Administration (HRSA), within the Department of Health and Human Services (HHS). Congress created the NHSC in the Emergency Health Personnel Act of 1970 (P.L. 91-623), and its programs have been reauthorized and amended several times since then.
The Patient Protection and Affordable Care Act of 2010 (ACA; P.L. 111-148) permanently reauthorized the NHSC. Prior to the ACA, the NHSC had been funded with discretionary appropriations. The ACA created a new mandatory funding source for the NHSC—, the Community Health Center Fund (CHCF), which was intended to supplement the program'’s annual appropriation. However, betweenfrom FY2012 andto FY2017, the CHCF entirely replaced the NHSC'’s discretionary appropriation. Forappropriations. Beginning in FY2018, the NHSC received $105 million from discretionary appropriations in P.L. 115-141 to support awards to expand and improve access to opioid and other substance use disorder treatment providers. The law also reserves $30 million from the $105 million for the new Rural Communities Opioid Response initiative administered by the Federal Office of Rural Health Policy within HRSA. For FY2018, CHCF funding represents 75% of the program's appropriation.
The CHCF is time-limited. Initially an appropriation from FY2011 through FY2015, the CHCF was subsequently extended in the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA, P.L. 114-10) through FY2017 and then extended for an additional two years (i.e., through FY2019) in the Bipartisan Budget Act of 2018 (BBA 2018, P.L. 115-123).
From FY2011 through FY2017, the most recent year of final data available, the NHSC offered more than 39program received discretionary appropriations again. These funds were appropriated for loan repayment for substance use disorder treatment providers, with some funds reserved for loan repayment for providers placed at rural facilities and at Indian Health Service facilities. In FY2021, the American Rescue Plan Act of 2021 (ARPA, P.L. 117-2) provided a one-time appropriation of $800 million to expand the number of scholarship and loan repayment awards the program can make. ARPA also reserved $100 million for states to make loan repayment awards.
Though the NHSC has received discretionary appropriations in recent years, the CHCF represents more than 70% of the program’s annual funding. The CHCF is time-limited. At its outset, it was an appropriation for FY2011 through FY2015, but it has been extended several times, most recently through FY2023 in the Consolidated Appropriations Act, 2021 (P.L. 116-260).
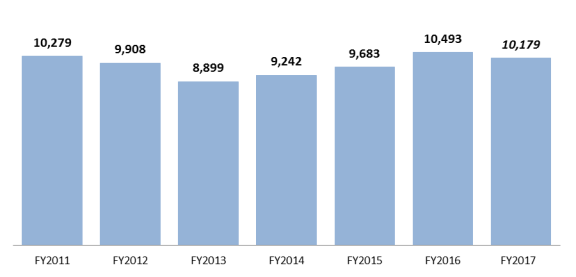
From FY2011 through FY2020, the NHSC offered more than 48,000 loan repayment agreements and scholarship awards to individuals who have agreed to serve for a minimum of two years in a HPSA. In FY2017HPSAs. In FY2020, the NHSC made 5,711offered more than 9,000 loan repayment agreements and scholarship awards. The number of awards the NHSC makes is only one component of program size, because not all awardees are currently serving as NHSC providers; some are still completing their training (e.g., scholarship award recipients). As such, the NHSC also measures its field strength: the number of NHSC providers who are fulfilling a service obligation in a HPSA in a given year. In FY2017FY2020, total NHSC field strength was 10,17916,229. NHSC providers are currently serving in a variety of settings throughout the entire United States and its territories. The majority of NHSC providers serve in outpatient settings, most commonly at federally qualified health centers.
Introduction
Congressional Research Service
link to page 4 link to page 5 link to page 6 link to page 7 link to page 7 link to page 7 link to page 8 link to page 9 link to page 9 link to page 10 link to page 12 link to page 12 link to page 13 link to page 14 link to page 15 link to page 17 link to page 17 link to page 14 link to page 15 link to page 17 link to page 10 link to page 12 link to page 21 The National Health Service Corps
Contents
Introduction ..................................................................................................................................... 1 Program Overview .......................................................................................................................... 2
Federal Scholarship Program .................................................................................................... 3 Federal Loan Repayment Program ............................................................................................ 4
Main Loan Repayment Program ......................................................................................... 4 Federal Students to Service (S2S) Loan Repayment Program............................................ 4 Substance Use Disorder Repayment Program .................................................................... 5 Rural Community Loan Repayment Program .................................................................... 6
State Loan Repayment Program ................................................................................................ 6
NHSC Funding ................................................................................................................................ 7 Program Size ................................................................................................................................... 9
Recruitment ............................................................................................................................... 9 Field Strength .......................................................................................................................... 10
Types of NHSC Providers .............................................................................................................. 11 NHSC Provider Locations ............................................................................................................. 12 Provider Retention ......................................................................................................................... 14 Legislative Proposals Related to the NHSC .................................................................................. 14
Figures Figure 1. Trends in National Health Service Corps (NHSC) Field Strength .................................. 11 Figure 2. National Health Service Corps Field Strength, by Discipline ........................................ 12 Figure 3. NHSC Providers by State, Territory ............................................................................... 14
Tables Table 1. National Health Service Corps (NHSC) Funding for FY2011-FY2021 ............................ 7 Table 2. National Health Service Corps (NHSC) Recruitment, FY2011-FY2020 .......................... 9
Contacts Author Information ........................................................................................................................ 18
Congressional Research Service
The National Health Service Corps
Introduction The National Health Service Corps (NHSC) is a clinician recruitment and retention program that aims to reduce health workforce shortages in underserved areas. The NHSC has three components: (1) a federal scholarships program, (2) a federal loan repayment program, and (3) a state-operated loan repayment program. Under each of these programs, health providers receive either scholarships or loan repayments in exchange for a service commitment at an NHSC-approved facility located in a federally designated health professional shortage area (HPSA, see text box).11 Participants in the state loan repayment programs may also serve in state-designated shortage areas; federal program participants may not. NHSC-approved facilities are generally nonprofit or government-operated (federal, state, local, andor tribal) organizations that provide care to patients without regard for the patient'’s ability to pay. The program’s clinicians provided care to an estimated 23.6 million patients in calendar year 2021. This is an increase from FY2019, when the program estimated that its clinicians provided care to 13.7 million patients.2
The three NHSC programs are managed by
Health Professional Shortage Areas (HPSAs)
the Bureau of Health
s ability to pay.
Health Professional Shortage Areas (HPSAs) HPSAs are areas—rural or urban—with a shortage of primary medical care,
Workforce (BHW) in the
dental, or mental health providers. Specific population groups (e.g., populations
Health Resources and
with unusually high needs for health services, as indicated by measures such as
Service Administration
the poverty rate and the infant mortality rate) and specific facilities (e.g., a community health center, or a facility operated by the Indian Health Service)
(HRSA), an agency in the
may also be designated as HPSAs.
Department of Health and
The HPSA designation is made based on ratios of provider per population; the
Human Services (HHS).
specified ratio may change, based on the type of HPSA (e.g., primary care or
The NHSC was created
mental health). For example, an area may be designated a primary care HPSA if
by the Emergency Health
it has a ful
provide an adequate
care needs.
supply of trained health
HPSA scores range from 0 to 25 (26 for dental HPSAs), with a higher score
providers in federally
indicating greater shortages.
designated HPSAs.3 Since
Source: Health Resources and Services Administration, Shortage Designation:
the program’s inception,
Health Professional Shortage Areas & Medically Underserved Areas/Populations,
Congress has
at |
The three NHSC programs are managed by the Bureau of Health Workforce (BHW) in the Health Resources and Service Administration (HRSA), an agency in the Department of Health and Human Services (HHS). The NHSC was created by the Emergency Health Personnel Act of 1970 to provide an adequate supply of trained health providers in federally designated HPSAs.2 Since the program's inception, Congress has reauthorized and revised the program several shortage-designation and CRS Infographic IG10015,
reauthorized and revised
Health Professional Shortage Areas (HPSAs).
the program several
1 NHSC providers supported by the federal programs must serve at an NHSC-approved service site; time spent at an unapproved site, even if that site is within a health professional shortage area (HPSA), does not count toward the clinician’s service commitment. See U.S. Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA), National Health Service Corps Loan Repayment Program, Fiscal Year 2021, Application & Program Guidance, March 2021, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/lrp-application-guidance.pdf, p. 44.
2 HHS, “HHS Announces Record Health Care Workforce Awards in Rural and Underserved Communities” press release, November 22, 2021, https://www.hhs.gov/about/news/2021/11/22/hhs-announces-record-health-care-workforce-awards-in-rural-underserved-communities.html, and “HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019,” Rockville, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf, p. 12.
3 P.L. 91-623 was enacted on December 31, 1970. The NHSC is authorized in Sections 331-338 of the Public Health Service Act (PHSA) (42 U.S.C. §254d et. seq.). The federal regulation states the purpose of the loan repayment (42 C.F.R. §62.21) and the scholarship program (42 C.F.R. §62.1).
Congressional Research Service
1
link to page 12 The National Health Service Corps
times, with the most recent reauthorization included in the Patient Protection and Affordable Care Act (P.L. 111-148, ACA). The ACA permanently reauthorized the NHSC, creating, among other things, a mandatory funding stream for the program and implementing a part-time option, which allows part-time service in exchange for an extended service commitment.3
4
This report provides an overview of the NHSC, including the program'’s funding, the number and types of providers the program supports, and the locations where they serve.
Program Overview
The NHSC consists of three programs: (1) a federal scholarshipsscholarship program,; (2) a federal loan repayment program, which includes several temporary component loan repayment programs; and and (3) a state-operated loan repayment program. The federal scholarship program provides scholarships in exchange for a service commitment at the end of a recipient'’s education, including any training required before licensure. The two loan repayment programs provide clinicians with loan repayment in exchange for an immediate service commitment.45 HRSA administers the federal scholarship and loan repayment programs and provides funds to states. States match these funds to operate state loan repayment programs.6 The largest program —by funding and by participants—is the federal loan repayment program, followed by the state loan repayment program, and then the scholarship program.
The section below describes these three programs. The discussion focuses on program differences; however, the programs share a number of common elements. Specifically, all three programsthe core programs generally require a minimum service commitment of two years in a HPSA.5 All7 Several of the component loan repayment programs require a three-year service commitment, including the substance use disorder loan repayment program, the rural community workforce loan repayment program, and the Student to Service loan repayment program (these programs are discussed below). All NHSC programs are restricted to U.S. citizens or U.S. nationals,68 and all provide awards that are exempt from federal income and employment taxes. In addition, all three programs allow physicians,79 dentists, physician assistants, nurse midwives, and nurse practitioners to participate, but the loan repayment programs also permit additional provider types to participate.810 The three program types are described below; Table 2 presents data on the number of awards made under each of these programs.
4 For additional changes included in the Affordable Care Act, see CRS Report R41278, Public Health, Workforce, Quality, and Related Provisions in ACA: Summary and Timeline.
5 PHSA Section 338G authorizes a fourth program that would provide a $25,000 loan to an NHSC member in exchange for two-years of service in a HPSA in private practice. This program has never been implemented.
6 Funding included in the American Rescue Plan Act (ARPA) for the state loan repayment program waived the state matching requirement.
7 Some individuals may serve more than two years. For example, some may serve part-time in exchange for an extended service commitment and some may extend their commitment upon receiving a continuation award, which entails additional scholarship or loan repayment in exchange for an extended commitment. See HHS, HRSA. “National Health Service Corps,” http://nhsc.hrsa.gov/. 8 U.S. nationals are individuals born in certain U.S. territories. 9 Physicians include individuals who have graduated from allopathic medical schools, which award Medical Doctor (MD) degrees and osteopathic medical schools which grant Doctors of Osteopathy (DO) degrees. Graduates of foreign medical schools are not eligible for the NHSC.
10 For example, the federal loan repayment program permits mental and behavioral health providers and dental hygienists to participate. The state loan repayment program allows these additional providers and permits states to designate additional provider types as eligible based on the state’s workforce needs.
Congressional Research Service
2
The National Health Service Corps
Generally, NHSC awards are made competitively, with scholarships awarded based on eligibility and a set of selection factors (e.g., the participant’s commitment to primary care practice and the likelihood of remaining in a shortage area after the NHSC service commitment has ended).11 Loan repayment awards are made based on the HPSA score of the site and on the loan repayment program’s eligibility and selection factors.12
Federal Scholarship Program Federal Scholarship Program
The NHSC Scholarship Program is established in Section 338A of the Public Health Service Act (PHSA).913 It provides scholarships—including tuition, reasonable education expenses, and a monthly living stipend—to individuals enrolled full-time in specified education programs at a fully accredited U.S. school.1014 Eligible schools/programs include medical schools (allopathic and osteopathic), physician assistant programs, dental schools, and advance practice nursing schools. Individuals must agree to complete their training (including residency training or required clinical hours, where applicable) in primary care.1115 For each year of scholarship support received (or partial year after the first year), students must agree to provide an additionala year of service in a HPSA. For example, if a full-time service scholar receives three years of scholarship support the scholar would owe three years of full-time service at an approved facility. Scholars incur a minimum service commitment of two years. The number of school years of NHSC scholarship support received by the scholar may not exceed four school years.1216 As such, through the scholarship program, the maximum required years of full-time service at an approved facility is four years.
NHSC scholars begin their service commitment upon the completion of training, including any advance clinical training needed for licensure (e.g., primary care residency for physicians). Participants must also have obtained a professional license, certificate, or registration before beginning their service commitment. NHSC scholars must fulfill their service commitment on a full-time basis and are required to fulfill their service commitment in a HPSA of "greatest need." Each year HRSA determines the HPSA score indicative of "greatest need." For example, from October 1, 2016, through September 30, 2017greatest need. This varies by provider type. For example, for class year 2022, NHSC scholars must work at NHSC-approved service sites with a HPSA score of 17 or above for their discipline (e.g., a dental scholar is required to serve in an area with a dental HPSA score above 17).1320 or above for primary care physicians or nurse practitioners, 14 or above for primary care physician assistants, and 10 or above for nurse midwives. Scores also vary for mental health HPSAs and dental HPSA providers.17 Individuals participating in the federal loan repayment program may serve part-time and may serve in areas with lower HPSA scores, but scholars may not. At the end of their service commitment, scholars may apply for continuation 11 HHS, HRSA, NHSC Scholarship Program, School Year 2021-2022 Application & Program Guidance, p. 8, https://nhsc.hrsa.gov/sites/default/files/nhsc/scholarships/scholarship-application-guidance.pdf.
12 HHS, HRSA, National Health Service Corps Loan Repayment Program, Fiscal Year 2021, Application & Program Guidance, March 2021, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/lrp-application-guidance.pdf, p. 20-21.
13 42 U.S.C. §254l. 14 Individuals who attend foreign medical schools are not eligible for the NHSC scholarship program. 15 For physicians, this is defined as family medicine, general internal medicine, general pediatrics, obstetrics/gynecology, general psychiatry, and joint programs in a combination of these specialties (e.g., internal medicine/pediatrics). For nurses, this is defined as adult medicine, family medicine, geriatrics, primary care pediatrics, psychiatric-mental health, or women’s health. For dentists, this is defined as general practice dentistry, advanced education in general dentistry, pediatric dentistry, and public health dentistry.
16 HHS, HRSA, NHSC Scholarship Program, School Year 2021-2022 Application & Program Guidance, p. 5, https://nhsc.hrsa.gov/sites/default/files/nhsc/scholarships/scholarship-application-guidance.pdf.
17 HRSA, NHSC, “Health Professional Shortage Area (HPSA) Score-Class Year 2022,” https://nhsc.hrsa.gov/scholarships/requirements-compliance/jobs-and-site-search/hpsa-score-class-year.
Congressional Research Service
3
The National Health Service Corps
scholars may not. At the end of their service commitment, scholars may apply for continuation awards through the loan repayment program if they still have educational debt remaining and are willing to continue service at an NHSC-approved facility.
Generally, NHSC awards are made competitively, with scholarships awarded based on a set of eligibility and selection factors (e.g., the participant’s commitment to primary care practice and the likelihood of remaining in a shortage area after the NHSC service commitment has ended).18 In HRSA’s 2019 report on NHSC to Congress, the agency disclosed that there were more than 1,800 scholarship applications for the 200 awards made.19
Federal Loan Repayment Program Federal Loan Repayment Program
The NHSC Federal Loan Repayment Program is authorized in PHSA Sections 331(i) and 338B.14 20 In addition to the list of providers who may participate in the scholarship program, dental hygienists and behavioral/mental health providers may also receive loan repayment.1521 Loan repayment recipients must have a license or certificate needed to practice and must be employed or have accepted an offer to be employed at an NHSC-approved work site. Loan repayment is available only for "qualifying educational debt,," which means principal, interest, and related expenses of outstanding government and private student loans obtained for undergraduate or graduate education for tuition, along with reasonable educational and living expenses.16 22 The section below discusses the main federal loan repayment program and additional specific loan repayment programs.
Main Loan Repayment Program
The main federal loan repayment program provides $50,000 for an initial two-year obligation.23 Federal loan repayors have a two-year service commitment, which they may fulfill full-time for two years or part-time for four.
The amount of loan repayment received varies based on the HPSA score of the site where the loan repayor is employed. For full-time service at an approved site with a HPSA score of 14 or above, a loan repayor may receive amounts up to $50,000 for an initial two-year obligation.17 Individuals serving at a site with a HPSA score of 13 or lower may receive up to $30,000 for an initial two years of service. Loan repayment recipients may apply for continuation awards if they have educational debt at the end of their two-year loan repayment commitment. Continuation awards are awarded in one-year intervals, and individuals may apply for and receive continuation awards as long as they have qualifying educational debt and remain employed at an NHSC-approved site.
Federal Students to Service (S2S) Loan Repayment Program
In 2012, HRSA used the authority in PHSA Section 338B18 to establish a new program within the federal loan repayment program called the Students to Service (S2S) Loan Repayment Program. The S2S program provides assistance of up to $120,000 to Continuation awards are awarded in one-year intervals, and individuals may apply for and receive continuation awards as long as they have qualifying educational debt and remain employed at an NHSC-approved site.
Federal Students to Service (S2S) Loan Repayment Program
In 2012, HRSA used the authority in PHSA Section 338B24 to establish a new program within the federal loan repayment program called the Students to Service (S2S) Loan Repayment Program.
18 HHS, HRSA, NHSC Scholarship Program, School Year 2021-2022 Application & Program Guidance, p. 9, https://nhsc.hrsa.gov/sites/default/files/nhsc/scholarships/scholarship-application-guidance.pdf.
19 HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019, Rockville, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf, p. 10.
20 42 U.S.C. §254d(i), as amended, and 42 U.S.C. §254l-1, as amended, and respectively. 21 A behavioral/mental health worker in the NHSC may be a licensed clinical social worker, licensed professional counselor, health service psychologist, marriage and family therapist, physician (e.g., a psychiatrist, including child and adolescent psychiatrists), nurse practitioner (i.e., a psychiatric nurse specialist), or physician assistant (e.g., mental health and psychiatry). See HHS, HRSA, National Health Service Corps Loan Repayment Program, Fiscal Year 2021, Application & Program Guidance, March 2021, https:/nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/lrp-application-guidance.pdf, p. 10-11.
22 HHS, HRSA, National Health Service Corps Loan Repayment Program, Fiscal Year 2021, Application & Program Guidance, March 2021, https:/nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/lrp-application-guidance.pdf.
23 Ibid. 24 42 U.S.C. §254l1(a)(2) requires the Secretary to establish an NHSC loan repayment program to recruit health professionals as needed.
Congressional Research Service
4
The National Health Service Corps
The S2S program provides assistance of up to $120,000 to providers in their last year of training. At its outset, this program was for medical students (allopathic and osteopathic) in their final year of medical school; however, the program has since expanded to include individuals in their last year of dental school, nurse practitioner training, nurse midwifery training, and physician assistant trainingof medical school. In return, S2S program recipients must complete an approved primary care residency19residency (if applicable)25 and undertake their required NHSC service in a HPSA of the greatest need for at least three years (full-time) or six years (half-time).2026 S2S repayors may also complete a one-year fellowship in geriatrics after their primary care residency and before beginning their service commitment.21
Zika Loan Repayment Program
In 2016, HRSA made loan repayment awards through a new program funded by the Zika Response and Preparedness Appropriations Act (P.L. 114-223).22 This program provides up to $70,000 in loan repayment in exchange for a three-year service commitment at NHSC approved sites in Puerto Rico or other U.S. territories affected by Zika.23 Health professionals eligible for the federal loan repayment program are also eligible for this program. Licensed professionals in medical specialties and allied health fields who may be able to provide Zika-related care (e.g., physical therapy and certain medical specialties) are also eligible.24
State Loan Repayment Program
certain fellowships that may be one or two years. These include one-year fellowships in geriatrics or obstetrics/gynecology, two-year child psychiatry fellowships, and one or two-year addiction medicine fellowships.27
Substance Use Disorder Repayment Program
Beginning in FY2018, HRSA received discretionary funding to provide loan repayments to behavioral health professionals who are providing substance use disorder treatment (SUD) in HPSAs. Language included in appropriations acts waives parts of the NHSC statute, which therefore permits a broader range of health professionals and service sites to be included in the program.28 This program is not permanently authorized in statute; as such, it may continue only if similar language is included in annual (or supplemental) appropriations laws.
The program’s purpose is to expand evidence-based SUD treatment and counseling available in HPSAs. Under this program, HRSA makes loan repayment to behavioral health providers, some of whom are not otherwise eligible for the NHSC loan repayment program (e.g., pharmacists).29 It also permits program participants to fulfill their service commitment in behavioral health treatment sites. Generally, NHSC sites are primary care focused, and, as such, facilities that focus exclusively on substance use treatment, such as opioid use disorder treatment programs, would not otherwise be eligible to receive NHSC clinicians. Because part of the program’s focus is on increasing access to opioid use disorder treatment, the program prioritizes awards to providers who have a DATA 2000 waiver that permits them to treat individuals with opioid use disorder with medication assisted treatment (MAT).30 The SUD workforce loan repayment program
25 Students must complete a residency in family practice, general internal medicine, general pediatrics, psychiatry, obstetrics-gynecology, internal medicine/family practice, or internal medicine/pediatrics. HHS, HRSA, National Health Service Corps, Students to Service Loan Repayment Program, FY2022, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/nhsc-students2service-lrp-application-program-guidance.pdf, p. 8.
26 In FY2022, for the S2S Program, sites with HPSAs scores of 14 or above are determined to be of high-need. See HHS, HRSA, National Health Service Corps, Students to Service Loan Repayment Program, FY2022, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/nhsc-students2service-lrp-application-program-guidance.pdf, p. 22.
27 Ibid., p. 19. 28 For example, the language appropriating FY2021 funds in P.L. 116-260, was as follows: That $120,000,000 shall remain available until expended for the purposes of providing primary health services, assigning National Health Service Corps (“NHSC”) members to expand the delivery of substance use disorder treatment services, notwithstanding the assignment priorities and limitations under Sections 333(a)(1)(D), 333(b), and 333A(a)(1)(B)(ii) of the PHS Act, and making payments under the NHSC Loan Repayment Program under Section 338B of such act. For FY2022, the federal government is operating under a continuing resolution. This generally continues the programs that were included in the FY2021 appropriations laws at the FY2021 funding level. See Division A of P.L. 117-43.
29 HHS, HRSA, National Health Service Corps, Substance Use Disorder Workforce Loan Repayment Program, FY2021, Application and Program Guidance, March 2021, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/sud-lrp-application-guidance.pdf, p. 6.
30 Ibid., p. 9. For information about medication assisted treatment and DATA 2000 waivers, see CRS In Focus IF10219, Opioid Treatment Programs and Related Federal Regulations.
Congressional Research Service
5
The National Health Service Corps
provides $75,000 in loan repayment in exchange for a three-year full-time service commitment in a designated mental health or primary medical care HPSA. It provides $37,500 in loan repayment for a three-year half-time service commitment.
Rural Community Loan Repayment Program
The Rural Community Loan Repayment program is similar to the SUD loan repayment program with regard to eligible providers and sites. Like that program, the Rural Community Loan Repayment program focuses on increasing access to opioid use disorder treatment. As such, the program includes awarding priority to providers who have a DATA 2000 waiver for MAT.31 Since FY2018, the program has been funded using a portion of the discretionary appropriations provided for SUD loan repayment. This program provides $100,000 for a three-year full-time service commitment for SUD treatment providers in rural areas.32 It also provides $50,000 for half-time clinical practice.33
State Loan Repayment Program The state loan repayment program is authorized in PHSA Section 338I.34The state loan repayment program is authorized in PHSA Section 338I.25 The program is similar to the Federal Loan Repayment Program, except that (1) it is a matching grant between the state and the NHSC,35 (2) states may choose to expand or contract the types of clinicians who are eligible to participate in their program, and (3) states may require more than two years of service in exchange for loan repayment. For example, states have the option of addressing their unique workforce needs by making additional types of professionals eligible, such as registered nurses and pharmacists, although neither of these provider types are eligible to participate in the main federal loan repayment program. State loan repayors must provide care in a HPSA in exchange for their award, but states determine the approved service sites (i.e., facility types) for their programs. State loan repayment participants must also serve two years as an initial commitment, but states may require longer minimum service commitments or may vary the service commitment length by provider type. State loan repayment recipients may fulfill their service commitments on a full- or part-time basis.
31 HHS, HRSA, National Health Service Corps, Rural Community Loan Repayment Program, FY2021, Application and Program Guidance, March 2021, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/rural-lrp-application-guidance.pdf, p. 10. For information about medication assisted treatment and DATA 2000 waivers, see CRS In Focus IF10219, Opioid Treatment Programs and Related Federal Regulations, and CRS Report R45279, Buprenorphine and the Opioid Crisis: A Primer for Congress. DATA 2000 waivers are also known as “x” waivers.
32 HHS, HRSA, National Health Service Corps, Rural Community Loan Repayment Program, FY2021, Application and Program Guidance, March 2021, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/rural-lrp-application-guidance.pdf, p. 7.
33 Ibid. 34 PHSA Section 338I(a)(2) (42 U.S.C. §254q–1) authorizes the Secretary to make grants to states for the NHSC State Loan Repayment program provided that a state agency agrees to administer the program. Within 42 C.F.R. §62.54, the state agencies administering the State Loan Repayment Program must comply with regulations to ensure that their health workforce meets requirements for training, placement in medically underserved areas, and comparability to the NHSC Federal Loan Repayment Program, among other things. For program guidance, see HHS, State Loan Repayment Contacts, http://nhsc.hrsa.gov/loanrepayment/stateloanrepaymentprogram/contacts.html.
35 Funding included in the American Rescue Plan Act of 2021 for the state loan repayment program waived the state matching requirement.
Congressional Research Service
6
link to page 10 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 link to page 11 The National Health Service Corps
NHSC Funding The amount of total funds that the NHSC receives determines the number of awards that the program can make. Historically, the NHSC had been exclusively funded as part of HRSA’s discretionary appropriation. However, that is no longer completely the case, as the program is now primarily funded by the mandatory Community Health Center Fund (CHCF). The CHCF is time-limited. At its outset, it was an appropriation from FY2011 through FY2015, but it has been extended several times, most recently in the Consolidated Appropriations Act, 2021 (P.L. 116-260), which extended funding through FY2023.36
The CHCF was intended to supplement NHSC appropriations. However, from FY2012 to FY2017, the CHCF entirely replaced the NHSC’s discretionary appropriation. Beginning in FY2018, the program received discretionary appropriations again, though these funds have been appropriated for loan repayment substance use disorder treatment providers with some funds reserved for loan repayment for providers placed at Indian Health Service facilities. Though the NHSC has received discretionary appropriations in recent years, the CHCF represents more than 70% of the program’s annual funding. In FY2021, the American Rescue Plan Act of 2021 provided a one-time appropriation of $800 million to temporarily expand the number of awards the program can make.37
Table 1 presents funding provided for the program between FY2011 and FY2021. The table also shows the percentage of funding that comes from discretionary and mandatory sources.
Table 1. National Health Service Corps (NHSC) Funding for FY2011-FY2021
(Dollars in millions)
FY
FY
FY
FY
FY
FY
FY
FY
FY
FY
FY
2011
2012
2013
2014
2015 2016
2017
2018
2019
2020
2021
Discretionary
$25a
__
__
__
__
__
__
$105b
$120c
$120d
$120c
Mandatory
$290
$295
$300e
$305f
$310g
$310h
$310i
$310j
$310j
$310k
$310l
(CHCF)
Mandatory
$800m
(ARPA)
Final
$315
$295
$285
$283
$287
$310
$289
$415
$430
$430
$1,230n
% Mandatory
92%
100%
100%
100%
100%
100%
100%
75%
72%
72%
90%o
commitments on a full- or part-time basis.
NHSC Funding
The amount of total funds that the NHSC receives determines the number of awards that the program can make. Historically, the NHSC had been exclusively funded as part of HRSA's discretionary appropriation. However, that is no longer the case, as the program is now funded by the mandatory Community Health Center Fund (CHCF). The ACA created the CHCF and provided mandatory funding for it over a five-year period (FY2011-FY2015).26 The fund was intended to supplement the NHSC budget; however, from FY2012 to FY2017, it made up the entirety of the program's funding. The CHCF was initially set to expire at the end of FY2015; however, it was extended for two years (FY2016 and FY2017) as part of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA, P.L. 114-10, CHIP is the State Children's Health Insurance Program).27 At the start of FY2018, no mandatory funds had been appropriated for the NHSC; however, a temporary extension (P.L. 115-96) ultimately provided mandatory funding for the first two quarters of FY2018, and the Bipartisan Budget Act of 2018 (BBA 2018, P.L. 115-123) later provided full-year funding for FY2018 and FY2019. Amounts provided by the CHCF have also been reduced in some years as part of the mandatory spending sequester (pursuant to the Balanced Budget and Emergency Deficit Control Act of 1985, as amended).28 Although the program had not received discretionary appropriations from FY2012 through FY2017, it received $105 million in FY2018 in P.L. 115-141 , with funds directed toward supporting health care providers who provide opioid and other substance use disorder treatment in HPSAs.
Table 1 presents funding provided for the program between FY2011 and FY2019—though amounts for FY2019 are subject to change. The table also shows the percentage of funding that comes from discretionary and mandatory sources. For FY2019, the table shows mandatory amounts already appropriated for the program, but readers should note that the FY2019 President's budget requested providing discretionary, rather than mandatory, funding for the program in that year.
|
Funding by Fiscal Year |
2011 |
2012 |
2013 |
2014 |
2015 |
2016 |
2017 |
2018 |
2019 |
|
Discretionary |
|
__ |
__ |
__ |
__ |
__ |
__ |
|
__ |
|
Mandatory |
$290 |
$295 |
|
|
|
|
|
|
|
|
Final |
$315 |
$295 |
$285 |
$283 |
$287 |
$310 |
$289 |
$415 |
TBD |
|
% Mandatory |
92% |
100% |
100% |
100% |
100% |
100% |
100% |
75% |
TBD |
Sources: Table prepared by CRS based on information from U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, Rockville, Rockvil e, MD, volumes FY2013 through FY2019.
FY2022. Notes: Abbreviations in the table notes: ACA = Patient Protection and Affordable Care Act of 2010 (P.L. 111-148, as amended); 148, as amended); ARPA= American Rescue Plan Act of 2021(P.L. 117-2); ARRA = American Recovery and Reinvestment Act of 2009 (P.L. 111-5); BBA 2018 = Bipartisan Budget Act of 2018 (P.L. 115-123); BBEDCA = Balanced Budget and Emergency Deficit Control Act of 1985( P.L. 112-25); CARES Act=Coronavirus Aid, Relief, and Economic Security Act (P.L. 116-136); CHCF = Community Health Center Fund; FY=fiscal year; NHSC = National Health Service Corps; MACRA = Medicare Access and CHIP Reauthorization Act of 2015 (P.L. 114-10); );
36 For more information, see CRS Report R46818, Health Care-Related Expiring Provisions of the 117th Congress, First Session. For information on differences between discretionary and mandatory spending, see CRS Report R44582, Overview of Funding Mechanisms in the Federal Budget Process, and Selected Examples.
37 HHS, “HHS Announces Record Health Care Workforce Awards in Rural and Underserved Communities” press release, November 22, 2021, https://www.hhs.gov/about/news/2021/11/22/hhs-announces-record-health-care-workforce-awards-in-rural-underserved-communities.html.
Congressional Research Service
7
The National Health Service Corps
and Office of Management and Budget (OMB); TBD = to be determined. Funding levels for FY2011-FY2018FY2021 are as enacted or adjusted for sequestration, where applicable.
a. For FY2022, the NHSC is receiving discretionary appropriations at the FY2021 level under continuing appropriations under P.L. 117-43 and P.L. 117-70. The Consolidated Appropriations Act, 2021 (P.L. 116-260), provided $310 mil ion to the CHCF for FY2022. a. ARRA represented a source of discretionary funds that were appropriated to the NHSC in FY2009, but
those funds are not considered to be an FY2011 appropriation. StillStil , they were reflected in the FY2011 budget. ARRA contributed $57 millionmil ion (not shown in the table) for federal loan repayments. See Justification of Estimations for Appropriations Committees, RockvilleRockvil e, MD, vol. FY2013, p. 76.
b.
b. P.L. 115-141; $30 million of included $105 mil ion for loan repayment for substance use disorder provider; $30 mil ion of
the amount appropriated ($105 million) is to be made availablemil ion) was reserved for a new Rural Communities Opioid Response Initiative administered by the Federal Office of Rural Health Policy in HRSA.
c. ACA appropriated $300 million
c. P.L. 115-245 included $105 mil ion for loan repayment for substance use disorder providers and reserved
$15 mil ion of that amount to place these providers at Indian Health Service, tribally operated, and Urban Indian organization facilities.
d. P.L. 116-94 included $105 mil ion for loan repayment for substance use disorder providers and reserved
$15 mil ion of that amount to place these providers at Indian Health Service, tribally operated, and Urban Indian organization facilities.
e. ACA appropriated $300 mil ion in mandatory funding for the NHSC to be used in FY2013. However, this
amount was subject to the 5.1% mandatory spending sequestration, resulting in a total of $284.7 millionmil ion for FY2013. The sequestration order was issued pursuant to the BBEDCA, as amended.
d.
f.
ACA appropriated $305 millionmil ion in mandatory funding for the NHSC to be used in FY2014. However, this amount was subject to the 7.2% mandatory spending sequestration, resulting in $283 millionmil ion for FY2014.
e.
g. ACA appropriated $310 millionmil ion in mandatory funding for the NHSC to be used in FY2015. However, this
amount was subject to the 7.3% mandatory spending sequestration, resulting in $287 millionmil ion for FY2015.
f.
h. MACRA extended mandatory funding for the NHSC, as part of the CHCF, for FY2016 and FY2017, at $310 million
mil ion in mandatory funding each fiscal year. However, this funding extension was enacted after the mandatory spending sequester for FY2016 was calculated by OMB. As a consequence, OMB did not include the FY2016 funding in the sequester calculation, and thus no sequester was ordered for the NHSC funding in FY2016. (See OMB Report to Congress on the Joint Committee Reductions for Fiscal Year 2016, February 2, 2015, available at https://obamawhitehouse.archives.gov/sites/default/files/omb/assets/legislative_reports/sequestration/2016_jc_sequestration_report_speaker.pdf.). P.L. 114-223 provided $6 millionmil ion in supplemental NHSC funding for Zika response. See discussion in CRS Report R44460, Zika Response Funding: Request and Congressional Action.
g.
i.
MACRA appropriated $310 millionmil ion in mandatory funding for the NHSC to be used in FY2017. However, this amount is subject to the 6.9% mandatory spending sequestration, resulting in $289 million.
h. mil ion.
j.
BBA 2018 appropriated $310 millionmil ion in mandatory funding for the NHSC for each of FY2018 and FY2019. These funds were appropriated after OMB had calculated the mandatory amounts to be sequestered in these fiscal years. As a result, no sequestration was applied to these mandatory NHSC funds.
i. The FY2019 President's budget requested $310 million in discretionary funding for the NHSC. However, three days before the FY2019 budget was released, P.L. 115-123 appropriated $310 million in mandatory funding for the NHSC in FY2019. The President's budget requests that NHSC be funded by discretionary spending, instead of mandatory spending, in FY2019. See Letter from Mick Mulvaney, Director Office of Management and Budget, to The Honorable Paul D. Ryan, Speaker of the House of Representatives, February 12, 2018, https://www.whitehouse.gov/wp-content/uploads/2018/02/Addendum-to-the-FY-2019-Budget.pdf.
k. ARPA provided $800 mil ion to remain available until expended. It reserved $100 mil ion for the state loan
repayment program but waived the requirement that states match the funds they receive. The law required that states use no more than 10% of the ARPA funds they receive to administer their state loan repayment programs.
l.
P.L. 116-260 appropriated $310 mil ion in mandatory funding for the NHSC for each of FY2021 through FY2023.
m. The CARES Act appropriated $310 mil ion in mandatory funding for the NHSC for FY2020. These funds
were appropriated after OMB had calculated the mandatory amounts to be sequestered in these fiscal years. As a result, no sequestration was applied to these mandatory NHSC funds.
n. ARPA funds are available until expended, as such, these funds may not all be expended in FY2021. The
amount that was appropriated for exclusive use in FY2021 is $430 mil ion.
o. If only calculating funds that are exclusively available for FY2021, the percentage mandatory would have
been 72%.
Congressional Research Service
8
link to page 12 link to page 13 link to page 13 link to page 13 The National Health Service Corps
Program Size Program Size
NHSC program size is measured in three ways: (1) funding, discussed above; (2) recruitment, which is the number of awards in different categories; and (3) field strength, which is the number of NHSC clinicians currently fulfilling their service commitments. Recruitment in a given year is generally smaller than the program'’s field strength because the latter includes loan repayors who are currently fulfilling their service commitments, including those who are fulfilling a second year of their service commitment, and individuals who received scholarships or S2S agreements in earlier years who have completed their required training and are currently fulfilling their service commitments. The section below discusses recruitment and field strength.
Recruitment
Recruitment From FY2011 through FY2017FY2020, the most recent year of final data available, the NHSC offered provided more than 3954,000 loan repayment agreements and scholarship awards to individuals who have agreed to serve for a minimum of two years in a HPSA. In FY2011, the beginning of the ACA's CHCF, the NHSC received its largest appropriation to date, whichThe resumption of discretionary appropriations for loan repayments in FY2018 increased the number of loan repayment awards that the NHSC was able to make. The number of awards made has varied since FY2011, with an increase in FY2016, while the number of awards made in FY2017 was more similar to the number awarded in FY2015.29program was able to make. Table 2 shows NHSC clinician recruitment activity for the NHSC'NHSC’s active programs, by type of award, from FY2011 through FY2017.
FY2020.
Table 2. National Health Service Corps (NHSC) Recruitment, FY2011- FY2017
(ByFY2020
(by number of awards or agreements, [except for states, by number of participants])
|
Program |
FY2011 |
FY2012 |
FY2013 |
FY2014 |
FY2015 |
FY2016 |
FY2017 |
|||||||
|
Federal Loan Repayment Agreements (New) |
|
|
|
|
|
|
| |||||||
|
|
|
|
|
|
|
| |||||||
|
Total Federal Loan Repayment (New & Continuing) |
5,418 |
4,267 |
4,505 |
4,880 |
4,775 |
5,190 |
4,813 |
|||||||
|
Students to Service Loan Repayment Agreements |
|
|
|
|
|
|
| |||||||
|
Scholarship Awards (New) |
|
|
|
|
|
|
| |||||||
|
Scholarship Awards (Continuing) |
|
|
|
|
|
|
| |||||||
|
Total Scholarship Awards (New & Continuing) |
262 |
222 |
196 |
197 |
207 |
213 |
188 |
|||||||
|
|
|
|
|
|
|
| |||||||
|
Total Awards (all types) |
6,074 |
4,839 |
5,226 |
5,620 |
5,698 |
6,129 |
5,801 |
Source: Prepared by CRS, based on data in U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, FY2019, Rockville, MD, p. 74.
FY2022 Rockvil e, MD, p. 90. a. Includes individuals who received loan repayment for providing substance use disorder treatment services,
and those receiving awards through rural community loan repayment program.
Field Strength Field Strength
The number of awards the NHSC makes at any point in time is only one component of program size, as not all awardees are currently serving as NHSC providers. Specifically, NHSC scholars and S2S program participants are still completing their training. As such, the NHSC also measures its field strength, which is the number of NHSC providers who are fulfilling a service obligation in a HPSA in a given year.30 In FY2017, the most recent year in which data are available38 In FY2020, total NHSC field strength was 10,179.3116,229.39 Field strength is a measure of both the NHSC appropriation, which affects the number of awards that can be made, and the relative balance between scholarships and loan repayment, both in the current fiscal year and in the past.3240 The NHSC field strength has increased in recent years as the number of awards made has increased (seesee Figure 1). . As of April 2018, HRSA data indicate that there were 8,256 total providers.33 The majority of these individuals (7,620) were loan repayors10,237) were in the main loan repayment program, which reflects the NHSC'’s prioritization of clinicians who will undertake their service commitment immediately in HPSAs.3441 In contrast, HRSA makes scholarship awards in an earlier year, so the funding investment is not realized for several years, as the scholar completes his or heruntil after the scholars complete their schooling and required training.
Despite increased field strength, more sites are eligible to receive an NHSC provider than there are NHSC providers. Specifically, in April 2018December 2021, there were 4,605more than 1,500 open NHSC positions that could not be filled because the NHSC field strength (which is driven by the program’s appropriation and its ability to make awards) was not sufficient to meet the needs of every NHSC site.42
38 National Advisory Council on the National Health Service Corps, Meeting Minutes Summary, HHS, Rockville, MD, 2012, p. 2, https://nhsc.hrsa.gov/corpsexperience/aboutus/nationaladvisorycouncil/meetingsummaries/011912minutes.pdf.
39 every NHSC site.35
Types of NHSC Providers
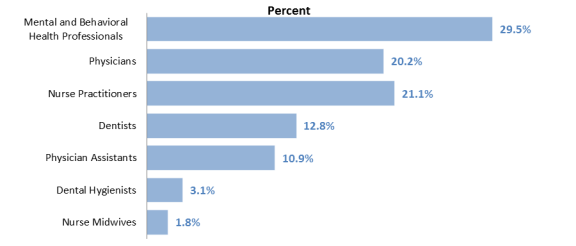
The NHSC is made up of an increasingly diverse set of health professionals. The composition of the NHSC has changed over time. In FY2009, physicians accounted for nearly 35% of providers and were the largest group of providers in the NHSC. In contrast, in FY2016, they made up 21%, and behavioral/mental health providers are now largest provider types.36 Physicians and nurse practitioners are the next largest groups of providers.
In FY2017, the most recent year for which complete data are available, the following three professional groups made up 73% of the NHSC:
Figure 2 shows the NHSC's workforce by provider type in FY2017, the most recent year for which complete data are available.
(September 2017) |
 |
p. 85. In addition to currently obligated NHSC clinicians, some NHSC alumni may remain as providers in a HPSA. These individuals are not included in NHSC field strength data. In FY2021, HHS estimated that the current program’s field strength with awards provided under the American Rescue Plan is approximately 22,000. This figure was included in a press release and does not provide more detailed program data; as such, it is not used in Figure 1. See HHS, “HHS Announces Record Health Care Workforce Awards in Rural and Underserved Communities” press release, November 22, 2021, https://www.hhs.gov/about/news/2021/11/22/hhs-announces-record-health-care-workforce-awards-in-rural-underserved-communities.html.
40 See section on “NHSC Funding” for a detailed discussion of NHSC funding sources. 41 Ibid. 42 data.HRSA.gov, “National Health Service Corps,” https://data.hrsa.gov/tools/data-explorer?paramServiceId=HPOL.
Congressional Research Service
10
link to page 15
The National Health Service Corps
Figure 1. Trends in National Health Service Corps (NHSC) Field Strength
(FY2011-FY2020, by number of providers who are fulfilling a service obligation in a HPSA in a given year)
Source: Prepared by CRS, based on data in U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, Notes: Total providers = 10,179. Physicians include both allopathic physicians who hold a Doctor of Medicine (MD) degree and osteopathic physicians who hold a Doctor of Osteopathic Medicine (DO) degree. "Other State Loan Repayment Clinicians" may include registered nurses and pharmacists, among others. |
Legislative Proposals to Expand NHSC Provider Eligibility
Some individuals and professional groups have advocated for making additional provider types eligible for the NHSC. For example, legislation in the 115th Congress (H.R. 1378) would make chiropractors eligible to participate in the federal scholarship and loan repayment programs, and H.R. 1639 and S. 619 would make physical therapists eligible for the federal loan repayment program.
The Consolidated Appropriations Act, 2018 (P.L. 115-141), expanded eligibility for the NHSC loan repayment program to substance use disorder counselors; the law also increased NHSC funding and specified that this funding be used to support substance use disorder providers. These specifications in the law may avert a number of the potential concerns that exist with other efforts to expand NHSC eligible provider types or sites. Specifically, because the number of applicants applying for awards exceeds the funding available, past efforts to expand provider eligibility have been met with concerns that it would increase competition for the program unless there was an increase in appropriations. Moreover, adding new provider types or site type does not guarantee that newly eligible clinicians or sites would receive awards, because there are no quotas for specific numbers of providers by discipline; however, the changes in the Consolidated Appropriations Act, 2018 (P.L. 115-141), specify that funds be used to support the newly added providers. Generally, NHSC awards are made competitively, with scholarships generally awarded based on participant characteristics (e.g., the participant's commitment to primary care practice and the likelihood of remaining in a shortage area after the NHSC service commitment has ended).39 Loan repayment awards are made based on the HPSA score of the site and on the loan repayment program participant's characteristics.40
Administrative Authority to Expand NHSC Provider Eligibility
Although legislation has been used to modify eligible disciplines, the HHS Secretary has some authority to add disciplines without new laws being enacted. For example, exchanges among the Secretary of HHS and the House and Senate Appropriations Committees seem to suggest that Congress recognizes the Secretary's authority to include additional disciplines in the NHSC without congressional action. For example, in 2012, the Senate Appropriations Committee urged the Secretary to offer loan repayments to pharmacists and chiropractors through the NHSC.41
Despite what appeared at that time to be congressional support for administrative action, in 2013, the Secretary declined to include pharmacists on the list of eligible NHSC providers. The Secretary's response to this request from the Senate Appropriations Committee was based on an interpretation that pharmacy and chiropractor services would be outside of the core intent of the NHSC to provide "primary health services."42
In 2015, the Senate Appropriations Committee again raised the issue of the Secretary's authority to add pharmacists, which are sometimes part of primary care teams; however, these providers remain ineligible for loan repayment. Similar conversations have occurred between HHS and the House Appropriations Committee regarding optometry.43
In each of these instances, HHS has not agreed to expand the program's eligibility out of concern that doing so would shift the program away from its traditional focus of providing primary care to underserved populations. HHS also emphasized that the program is currently competitive and that adding new disciplines as eligible could redirect NHSC funds away from already identified clinical shortage areas and add new ones.44 Another concern is that adding new providers may limit the total number of individuals served by the NHSC because the new provider types (e.g., optometrists and chiropractors) serve a narrower subset of the population than do primary care providers.
Despite debates on expanding the clinicians eligible for the NHSC, Congress has, at times, clarified the range of eligible providers. For example, the 21st Century Cures Act, enacted in 2016, clarified that adolescent and child psychiatrists are eligible to participate in the federal loan repayment program.45 This law, however, did not expand the list of NHSC providers. Instead, it sought to clarify that, within the existing group of NHSC-eligible psychiatrists, those who specialize in child and adolescent psychiatry are eligible to participate in the NHSC.
NHSC Provider Locations
FY2022, Rockvil e, MD, p. 91. Note: NHSC field strength is the number of NHSC clinicians or providers who are fulfil ing a service obligation in a Health Professional Shortage Area (HPSA) in exchange for a scholarship or loan repayment agreement.
Types of NHSC Providers The NHSC is made up of an increasingly diverse set of health professionals. In FY2009, physicians accounted for nearly 35% of providers and were the largest group of providers in the NHSC. In contrast, in FY2016, they made up 21%, and behavioral/mental health providers had become the largest provider type, at 30% of all providers in that year.43 In FY2018, the SUD workforce loan repayment program began, further increasing the number and type of behavioral/mental health providers in the program. In FY2020, 44% of providers were behavioral/mental health providers.44 Nurse practitioners and then physicians were the next largest groups of providers. Combined with behavioral/mental health providers, these three provider types made up 77% of the NHSC in 2020.
Figure 2 shows the NHSC’s workforce by provider types in FY2020, the most recent year for which complete data are available.
43 HHS, HRSA, Justification of Estimates for Appropriations Committees, FY2011, p. 69. 44 HHS, HRSA, Justification of Estimates for Appropriations Committees, FY2022, p. 86.
Congressional Research Service
11
The National Health Service Corps
Figure 2. National Health Service Corps Field Strength, by Discipline
(September 2020)
Source: Prepared by CRS, based on data in U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, FY2022, Rockvil e, MD, p. 86. Notes: Total providers = 16,229. Physicians include both allopathic physicians who hold a Doctor of Medicine (MD) degree and osteopathic physicians who hold a Doctor of Osteopathic Medicine (DO) degree. “Other State Loan Repayment Clinicians” may include registered nurses and pharmacists, among others.
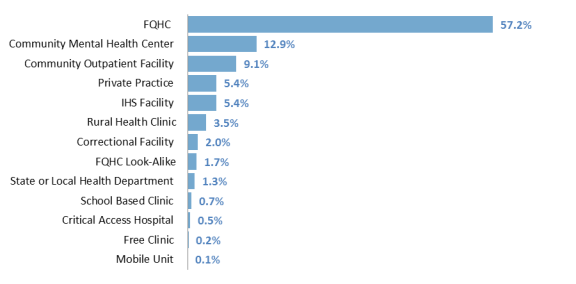
NHSC Provider Locations NHSC providers may serve at a number of facility types that generally focus on providing outpatient primary care to patients regardless of their ability to pay. In addition, some NHSC provider sites generally focus on primary care, such as community mentalfederal health centers, which are more targeted to behavioral health carewhile others may target behavioral health, such as community mental health centers. As mentioned, these facilities must be located in HPSAs. NHSC eligible sites include46
- include45
community mental health centers,
- correctional facilities,
- correctional facilities, critical access hospitals,
- facilities funded by the Indian Health Service (including those operated by Indian
Tribes, Tribal Organizations, and Urban Indian Organizations),
- federal health centers (i.e., Federally Qualified Health Centers [FQHCs]),
- FQHC look-alikes,
- free clinics,
- free clinics, rural health clinics, and
- school-based health centers.
45 Under limited circumstances, NHSC providers may also fulfill their service commitment by working in a private practice in a HPSA. For more information about these facility types, see CRS Report R43937, Federal Health Centers: An Overview for description of health centers and Appendix A for description of other NHSC eligible facility types. Indian Health Service facilities are also described in CRS Report R43330, The Indian Health Service (IHS): An Overview.
Congressional Research Service
12
link to page 17 link to page 17 The National Health Service Corps
NHSC providers can be placed at facilities operated by not-for-profit organizations and by government entities (including state, local, tribal, and federally operated facilities). In addition, HRSA requires that NHSC sites are part of a system of care (e.g., have referral arrangements for specialty care and after-hours arrangements for patient care); have a documented record of sound fiscal management; have a history of using NHSC providers appropriately and efficiently; accept beneficiaries from Medicare, Medicaid, and CHIP; have a sliding scale discount schedule; and have general community support for assigning NHSC providers to the facility.47
More than half46
For the SUD Loan repayment program, HRSA made additional sites eligible. These include outpatient Opioid Treatment Programs (OTPs) certified by the Substance Abuse and Mental Health Services Administration (SAMHSA),47 office-based opioid treatment facilities (OBOTs), and non-opioid SUD treatment facilities.48
Over 60% of all NHSC providers serve at federally qualified health centers (FQHCs), which provide outpatient—generally primary and behavioral—health care to disadvantaged populations regardless of theirpatients’ ability to pay (see Figure 3).48.49 NHSC providers also increasingly provide care at facilities funded by the Indian Health Service, including federal, tribal, and urban Indian health facilities. As of August 2017, 492 (5.4%) providers were fulfilling their service commitment at IHS-funded facilities, an increase from the 421 providers who were placed at IHS facilities as of December 2015.49; this is particularly true with funds appropriated in FY2019-FY2021 to place NHSC providers at IHS-funded facilities.50 As mentioned, NHSC providers generally fulfill their service commitment in outpatient settings. However, some may serve at IHS-funded hospitals, and in recent years, some have fulfilled part of their service commitment (up to 24 hours per week) at critical access hospitals (CAHs), which are small hospitals located in rural areas. As of August 2017, 45 September 30, 2019, 66 NHSC providers were serving at CAHs.51 HRSA requires that these providers split their time between inpatient services at the CAH (up to 24 hours per week) and outpatient services at CAH affiliated-outpatient clinics (not less than 16 hours per week).52
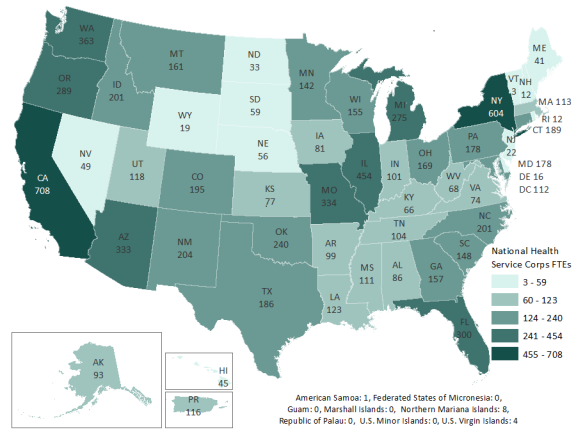
NHSC providers are located at HPSAs throughout the United States and its territories (see Figure 3). According to 2019 data, 36% of all NHSC providers served in rural areas.53
46 HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019, Rockville, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf, p. 5.
47 HHS, Substance Abuse and Mental Health Services Administration, “Certified Opioid Treatment Program,” https://www.samhsa.gov/medication-assisted-treatment/become-accredited-opioid-treatment-program. These are facilities that are permitted to administer and dispense medication assisted treatment (MAT) for treatment of opioid use disorders.
48 HHS, HRSA, National Health Service Corps, Substance Use Disorder Workforce Loan Repayment Program, FY2021, Application and Program Guidance, March 2021, https://nhsc.hrsa.gov/sites/default/files/nhsc/loan-repayment/sud-lrp-application-guidance.pdf, pp. 26-27.
49 For more information, see CRS Report R43937, Federal Health Centers: An Overview. 50 For more information, see CRS Report R43330, The Indian Health Service (IHS): An Overview. 51 HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019, Rockville, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf, p. 3.
52 Ibid. 53 HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019, Rockville, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf. In its FY2021 report on HPSA designations approximately 60% of primary care HPSAs were rural (similar percentages of dental and mental health HPSAs were also considered rural). See Bureau of Health Workforce, HRSA, HHS, Designated Health Professional Shortage Areas, Fourth Quarter of Fiscal Year 2021 Designated HPSA Quarterly Summary, Rockville, MD, September 30, 2021, https://data.hrsa.gov/Default/GenerateHPSAQuarterlyReport.
Congressional Research Service
13
The National Health Service Corps
Figure 3. NHSC Providers by State, Territory
(FY2019)
Source: CRS Analysis of HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019, Rockvil e, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf, p. 16.
Provider Retention The NHSC collects data on the retention of NHSC clinicians. In 2019, the NHSC measured long-term retention as those who remained at their site or in a HPSA after completing their service commitment between 2012 and 2018. 54 Under that measure, in 2019, 85% of NHSC clinicians were retained. The program measured short-term retention in 2019, as clinicians who remained at their practice site after completing their service commitment in the past year (i.e., 2018). More than 80% of recently finished NHSC corps members remained at their practice site in 2019. Note that members who finished in 2018 may be included in both measures. HRSA also modernized its data systems to better track its alumni starting in FY2019, which may provide additional insights into the program.
Legislative Proposals Related to the NHSC This section discusses some common types of legislative proposals that would amend the NHSC and discusses how the new NHSC SUD loan repayment program (including the rural component)
54 Information in this paragraph is drawn from HHS/HRSA, Report to Congress, National Health Service Corps for the Year 2019, Rockville, MD, 2019, https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/nhsc-report-congress-2019.pdf, p. 13.
Congressional Research Service
14
The National Health Service Corps
and a new separate loan repayment program for substance abuse providers interact with proposed legislation.
In general, legislative proposals for the NHSC have sought to expand the types of providers and service locations that are eligible for the program. For example, legislation in the 117th Congress (H.R. 3759 and S. 2676) would make physical therapists eligible for the federal loan repayment program.55 Although legislation has been used to modify the list of eligible disciplines, the HHS Secretary has some authority to add disciplines without new laws being enacted.56 For example, in prior requests from appropriations committees about including pharmacists in the program, the HHS Secretary has declined to do so based on an interpretation that pharmacy and chiropractor services would be outside of the core intent of the NHSC to provide “primary health services.”57 Similar conversations have occurred between HHS and the House Appropriations Committee regarding optometry.58 At present, pharmacists are included in the SUD loan repayment program (including the rural component) and states can elect to include them in their loan repayment programs. Optometrists are not eligible for the federal NHSC loan repayment programs.
In general, HHS has not agreed to expand the list of the main loan repayment program’s eligible provider types out of concern that doing so would shift the program away from its traditional focus of providing primary care to underserved populations. HHS also emphasized that the program is currently competitive and that adding new eligible disciplines could redirect NHSC funds away from already identified clinical shortage areas (and thus potentially create new ones).59 Another concern is that adding new provider types may limit the total number of individuals served by the NHSC, because the new provider types (e.g., physical therapists) generally serve a narrower subset of the population than do primary care providers.
Despite debates on expanding the clinicians eligible for the NHSC, Congress has at times clarified the range of eligible providers. For example, in 2016, the 21st Century Cures Act (P.L. 114-255) clarified that adolescent and child psychiatrists are eligible to participate in the federal loan repayment program.60 Generally, the NHSC does not include subspecialists (which child and
55 Other bills in the 117th and 116th Congresses also propose adding additional types of providers to the program. See, for example, H.R. 3912 and S. 1676 in the 116th Congress, which would have added nephrologists to the program.
56 For information on prior types of health provider expansions considered, see U.S. Congress, Senate Committee on Appropriations, Subcommittee on Departments of Labor, Health and Human Services, and Education, and Related Agencies, Departments Labor, Health and Human Services, and Education, and Related Agencies Appropriation Bill, 2012, To Accompany S. 1599, 112th Cong., 1st sess., September 22, 2011, S.Rept. 112-84 (Washington: GPO, 2012), p. 40.
57 Primary health services are defined as health services regarding family medicine, internal medicine, pediatrics, obstetrics and gynecology, dentistry, or mental health that are provided by physicians or other health professionals. HHS, HRSA, Justification of Estimates for Appropriations Committees, FY2013, p. 371, http://www.hrsa.gov/about/budget/budgetjustification2013.pdf. In P.L. 107-251, Health Care Safety Net Amendments of 2001 (enacted on October 26, 2002), Congress required the Secretary to implement a “Chiropractic/Pharmacist Demonstration Project” under Section 338B of the PHSA (or the NHSC’s Federal Loan Repayment Program). Following a general notice (68 Federal Register 112; 34981; June 11, 2003), the Secretary implemented the program but discontinued it after initial demonstrations were completed. Source: CRS email communication HHS, Office of Legislative Affairs, August 2016.
58 H.Rept. 114-699, Departments of Labor, Health and Human Services, and Education, and Related Agencies Appropriations Bill, 2017, to accompany H.R. 5926, p. 28.
59 HHS, HRSA, Justification of Estimates for Appropriations Committees, FY2017, p. 427, http://www.hrsa.gov/about/budget/budgetjustification2017.pdf. In the 2018 Budget Justification, HRSA also declined to broaden the eligible disciplines for the NHSC. Seeaffiliated-outpatient clinics (not less than 16 hours per week).50
NHSC providers are located at HPSAs throughout the United States and its territories (see Figure 4). According to 2016 data, 23% of all NHSC providers served in rural areas.51
(April 2018) |
 |
|
Legislative efforts have also been undertaken to expand the types of sites eligible for NHSC providers, specifically targeting facilities that could provide treatment for individuals with opioid addiction. For example, in the 115th Congress, S. 1453 would make substance use disorder treatment facilities eligible provider sites. These facilities provide both outpatient and inpatient services, including medication-assisted treatment. Proposals to expand eligible sites may face similar challenges to proposals to expand provider types—namely that the number of sites eligible for NHSC providers exceeds the program's field strength, so adding new site types may increase the number of sites and positions that seek NHSC providers but are unable to obtain one.
Provider Retention
The NHSC collects limited data on whether NHSC providers remain in HPSAs after fulfilling their service commitments. Available data indicate that less than half (43%) remain at their service site, and nearly 80% practice in a HPSA one year after their service commitment has ended.52 An FY2012 study found that more than half remain in a HPSA 10 years after completing their service. These data are similar to what HRSA found in an FY2000 evaluation of the program.
Author Contact Information
Acknowledgments
Bernice Reyes-Akinbileje, former CRS analyst in Health Resources and Services, authored a prior report on the National Health Service Corps, and Calvin C. DeSouza, CRS geographic information specialist, prepared the map included in this report.
Footnotes
| 1. |
NHSC providers supported by the federal programs must serve at an NHSC-approved service site; time spent at an unapproved site, even if that site is within a health professional shortage area (HPSA), does not count toward the clinician's service commitment. See U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Loan Repayment Program, https://nhsc.hrsa.gov/loanrepayment/lrpapplicationguidance.pdf, p. 30. |
| 2. |
P.L. 91-623 was enacted on December 31, 1970. The NHSC is authorized in Sections 331-338 of the Public Health Service Act (PHSA) (42 U.S.C. §254d et. seq.). The federal regulation states the purpose of the loan repayment (42 C.F.R. §62.21) and the scholarship program (42 C.F.R. §62.1). |
| 3. |
For additional changes included in the Affordable Care Act, see CRS Report R41278, Public Health, Workforce, Quality, and Related Provisions in ACA: Summary and Timeline. |
| 4. |
PHSA Section 338G authorizes a fourth program that would provide a $25,000 loan to an NHSC member in exchange for two-years of service in a HPSA in private practice. This program has never been implemented. |
| 5. |
|
| 6. |
U.S. nationals are individuals born in certain U.S. territories. |
| 7. |
Physicians include individuals who have graduated from allopathic medical schools, which award Medical Doctor (MD) degrees and osteopathic medical schools which grant Doctors of Osteopathy (DO) degrees. |
| 8. |
For example, the federal loan repayment program permits mental and behavioral health providers and dental hygienists to participate. The state loan repayment program allows these additional providers and permits states to designate additional provider types as eligible based on the state's workforce needs. |
| 9. |
42 U.S.C. §254l. |
| 10. |
Individuals who attend foreign medical schools are not eligible for the NHSC scholarship program. |
| 11. |
For physicians, this is defined as family medicine, general internal medicine, general pediatrics, obstetrics/gynecology, general psychiatry, and joint programs in a combination of these specialties (e.g., internal medicine/pediatrics). For nurses, this is defined as adult medicine, family medicine, geriatrics, primary care pediatrics, psychiatric-mental health, or women's health. For dentists, this is defined as general practice dentistry, advanced education in general dentistry, pediatric dentistry, and public heath dentistry. |
| 12. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, NHSC Scholarship Program, School Year 2017-2018 Application & Program Guidance, p. 10, https://nhsc.hrsa.gov/downloads/spapplicationguide.pdf. |
| 13. |
Each year, the NHSC uses HPSA scores to determine where NHSC scholars will be placed. For example, from October 1, 2016, through September 30, 2017, NHSC scholars must work at NHSC-approved service sites with a HPSA score of 17 or above for their discipline. U.S. Department of Health and Human Services, Health Resources and Services Administration, NHSC Scholarship Program, School Year 2017-2018 Application & Program Guidance, https://nhsc.hrsa.gov/downloads/spapplicationguide.pdf. Severity of need is determined by a scoring process that the Secretary applies to each designated area. A high-need HPSA is defined as a HPSA score of 14 or above; the higher the score, the greater the need for an NHSC clinician. U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Loan Repayment Program, FY2017, January 2017, pp. 16-17. |
| 14. |
42 U.S.C. §254d(i), as amended, and 42 U.S.C. §254l-1, as amended, and respectively. |
| 15. |
A behavioral/mental health worker in the NHSC may be a licensed clinical social worker, licensed professional counselor, health service psychologist, marriage and family therapist, physician (e.g., a psychiatrist, including child and adolescent psychiatrists), nurse practitioner (i.e., a psychiatric nurse specialist), or physician assistant (e.g., mental health and psychiatry). See U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Loan Repayment Program, FY2017, January 2017, pp. 10-17, https://nhsc.hrsa.gov/loanrepayment/lrpapplicationguidance.pdf. |
| 16. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Loan Repayment Program, FY2017, January 2017, p. 7, https://nhsc.hrsa.gov/loanrepayment/lrpapplicationguidance.pdf. |
| 17. |
|
| 18. |
42 U.S.C. §254l1(a)(2) requires the Secretary to establish an NHSC loan repayment program to recruit health professionals as needed. |
| 19. |
Students must complete a residency in family practice, general internal medicine, general pediatrics, general psychiatry, obstetrics-gynecology, internal medicine/family practice, or internal medicine/pediatrics. |
| 20. |
In FY2017, for the S2S Program, sites with HPSAs scores of 14 or above are determined to be of high-need. See U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps, Students to Service Loan Repayment Program, FY2017, https://nhsc.hrsa.gov/loanrepayment/studentstoserviceprogram/applicationguidance.pdf, p. 5. |
| 21. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps, Students to Service Loan Repayment Program, FY2017, https://nhsc.hrsa.gov/loanrepayment/studentstoserviceprogram/applicationguidance.pdf, pp. 6-7. |
| 22. |
The Zika Response and Preparedness Appropriations Act (P.L. 114-223) allocated $6 million for loan repayment awards. |
| 23. |
For information on awards made under this program, see U.S. Department of Health and Human Services, Health Resources and Services Administration, "HRSA Awards $7M to Workforce Programs to Combat Zika," press release, July 26, 2017, https://www.hrsa.gov/about/news/press-releases/hrsa-awards-seven-million-to-workforce-programs.html. |
| 24. |
The full list of eligible professions for this program is available at U.S. Department of Health and Human Services, Health Resources and Services Administration, "NHSC Zika Loan Repayment Program," https://nhsc.hrsa.gov/loanrepayment/zikainitiative.html. |
| 25. |
PHSA Section 338I(a)(2) (42 U.S.C. §254q–1) authorizes the Secretary to make grants to states for the NHSC State Loan Repayment program provided that a state agency agrees to administer the program. Within 42 C.F.R. §62.54, the state agencies administering the State Loan Repayment Program must comply with regulations to ensure that their health workforce meets requirements for training, placement in medically underserved areas, and comparability to the NHSC Federal Loan Repayment Program, among other things. For program guidance, see HHS, State Loan Repayment Contacts, http://nhsc.hrsa.gov/loanrepayment/stateloanrepaymentprogram/contacts.html. |
| 26. |
The NHSC also received two years of funding in FY2009 and FY2010 as part of the American Recovery and Reinvestment Act of 2009. For more information, see CRS Report R40181, Selected Health Funding in the American Recovery and Reinvestment Act of 2009. |
| 27. |
CRS Report R43962, The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA; P.L. 114-10). CHIP is the State Children's Health Insurance Program (CHIP). |
| 28. |
The Balanced Budget and Emergency Deficit Control Act of 1985 was amended by the Budget Control Act of 2011 (BCA, P.L. 112-25) to provide a budget process mechanism that would reduce mandatory spending and further reduce discretionary spending over an extended period. For mandatory spending, the reductions are to occur through "sequestration" in each fiscal year from FY2013 through FY2027. As originally enacted in the BCA, mandatory sequestration was scheduled to run through FY2021, but this period has subsequently been incrementally extended by P.L. 113-67, P.L. 113-82, P.L. 114-74, and P.L. 115-123. CHCF funds have been subject to sequestration in years in which there was a CHCF appropriation in place at the time the sequester was calculated by the Office of Management and Budget (e.g., CHCF funds were sequestered in FY2013, FY2014, FY2015 and FY2017, but were not sequestered in FY2016, FY2018, or FY2019). |
| 29. |
In FY2011, the NHSC received a total of $315 million in appropriated funds, representing a 121.8% increase over the previous year (from $141 million in FY2010 to $315 million in FY2011) (see "NHSC Funding" in this report). |
| 30. |
National Advisory Council on the National Health Service Corps, Meeting Minutes Summary, HHS, Rockville, MD, 2012, p. 2, https://nhsc.hrsa.gov/corpsexperience/aboutus/nationaladvisorycouncil/meetingsummaries/011912minutes.pdf. |
| 31. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, FY2019, Rockville, MD, p. 75. In addition to currently obligated NHSC clinicians, some NHSC alumni may remain as providers in a HPSA. These individuals are not included in NHSC field strength data. |
| 32. |
See section on "NHSC Funding" for a detailed discussion of NHSC funding sources. |
| 33. |
This number is according to HRSA data on April 26, 2018. Data available at https://datawarehouse.hrsa.gov/Topics/Nhsc.aspx. |
| 34. |
Ibid. |
| 35. |
Ibid. |
| 36. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimates for Appropriations Committees, FY2011, p. 69. |
| 37. |
This number is an underestimate because psychiatrists are counted as physicians and advanced practice psychiatric nurses are counted as nurse practitioners. |
| 38. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, FY2018, Rockville, MD, p. 70. Nurse Practitioners make up 20% of the NHSC's workforce; 2% of these are nurse-midwives. |
| 39. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, NHSC Scholarship Program, School Year 2017-2018 Application & Program Guidance, https://nhsc.hrsa.gov/downloads/spapplicationguide.pdf, pp. 7-9. |
| 40. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Loan Repayment Program, https://nhsc.hrsa.gov/loanrepayment/lrpapplicationguidance.pdf, p. 17. |
| 41. |
U.S. Congress, Senate Committee on Appropriations, Subcommittee on Departments of Labor, Health and Human Services, and Education, and Related Agencies, Departments Labor, Health and Human Services, and Education, and Related Agencies Appropriation Bill, 2012, To Accompany S. 1599, 112th Cong., 1st sess., September 22, 2011, 112-84 (Washington: GPO, 2012), p. 40. |
| 42. |
Primary health services are defined as health services regarding family medicine, internal medicine, pediatrics, obstetrics and gynecology, dentistry, or mental health that are provided by physicians or other health professionals. HHS, HRSA, Justification of Estimates for Appropriations Committees, FY2013, p. 371, http://www.hrsa.gov/about/budget/budgetjustification2013.pdf. In P.L. 107-251, Health Care Safety Net Amendments of 2001 (enacted on October 26, 2002), Congress required the Secretary to implement a "Chiropractic/Pharmacist Demonstration Project" under Section 338B of the PHSA (or the NHSC's Federal Loan Repayment Program). Following a general notice (68 Federal Register 112; 34981; June 11, 2003), the Secretary implemented the program but discontinued it after initial demonstrations were completed. Source: CRS email communication HHS, Office of Legislative Affairs, August 2016. |
| 43. |
H.Rept. 114-699, Departments of Labor, Health and Human Services, and Education, and Related Agencies Appropriations Bill, 2017, to accompany H.R. 5926, p. 28. |
| 44. |
HHS, HRSA, Justification of Estimates for Appropriations Committees, FY2017, p. 427, http://www.hrsa.gov/about/budget/budgetjustification2017.pdf. In the 2018 Budget Justification, HRSA also declined to broaden the eligible disciplines for the NHSC. See Department of Health and Human Services, Health Resources and Services Administration, Justification of Estimations for Appropriations Committees, FY2018, Rockville, MD, p. 331. |
| 45. |
See discussion of Sec. 9023 in CRS Report R44718, The Helping Families in Mental Health Crisis Reform Act of 2016 (Division B of P.L. 114-255). |
| 46. |
Under limited circumstances, NHSC providers may also fulfill their service commitment by working in a private practice in a HPSA. For more information about these facility types, see CRS Report R43937, Federal Health Centers: An Overview for description of health centers and Appendix A for description of other NHSC eligible facility types. Indian Health Service facilities are also described in CRS Report R43330, The Indian Health Service (IHS): An Overview. |
| 47. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Report to Congress For the Year 2016, submitted to the Committee on Health, Education, Labor and Pensions, U.S. Senate and The Committee on Energy and Commerce, U.S. House of Representatives, Rockville, MD, 2017. |
| 48. |
For more information, see CRS Report R43937, Federal Health Centers: An Overview. |
| 49. |
Email from Office of Legislation, Health Resources and Services Administration, Department of Health and Human Services, August 23, 2017 and U.S. Department of Health and Human Services, Indian Health Service, Justification of Estimations for Appropriations Committees, FY2017, Rockville, MD, p. 149. |
| 50. |
Ibid. |
| 51. |
U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Report to Congress For the Year 2016, submitted to the Committee on Health, Education, Labor and Pensions, U.S. Senate and the Committee on Energy and Commerce, U.S. House of Representatives, Rockville, MD, 2017. According to the U.S. Census Bureau, 19.3% of the U.S. population live in rural areas; see United States Census Bureau, "New Census Data Show Differences Between Urban and Rural Populations," press release, December 8, 2016, https://www.census.gov/newsroom/press-releases/2016/cb16-210.html. |
| 52. |
Data in this paragraph are drawn from U.S. Department of Health and Human Services, Health Resources and Services Administration, National Health Service Corps Report to Congress For the Year 2016, submitted to the Committee on Health, Education, Labor and Pensions, U.S. Senate and the Committee on Energy and Commerce, U.S. House of Representatives, Rockville, MD, 2017. |