National Institutes of Health (NIH) Funding: FY1996-FY2026
Changes from June 15, 2017 to May 2, 2018
This page shows textual changes in the document between the two versions indicated in the dates above. Textual matter removed in the later version is indicated with red strikethrough and textual matter added in the later version is indicated with blue.
NIH Funding: FY1994-FY2018
FY2019
Contents
NIH Funding: FY1994-FY2018
FY2019
The National Institutes of Health (NIH) is the primary federal agency charged with conducting and supporting biomedical and behavioral research. ItsIt is the largest of the eight health-related agencies that make up the Public Health Service (PHS) within the Department of Health and Human Services (HHS).1 NIH's organization consists of the Office of the Director (OD) and 27 Institutes and Centers. The OD sets overall policy for NIH and coordinates the programs and activities of all NIH components, particularly in areas of research that involve multiple institutes.
NIH activities cover a wide range of basic, clinical, and translational research, focused on particular diseases, areas of human health and development, or more fundamental aspects of biomedical research. Its mission also includes research training and health information collection and dissemination.12 More than 80% of the NIH budget funds extramural research through grants, contracts, and other awards.23 This funding supports research performed by more than 300,000 individuals who work at over 2,500 hospitals, medical schools, universities, and other research institutions around the country.34 About 10% of the agency's budget supports intramural clinical and basic research conducted by nearly 6,000 NIH physicians and scientists, most of whom are located on the NIH campus in Bethesda, MD.45
Funding for NIH comes primarily from the annual Labor, HHS, and Education (LHHS) appropriations bill, with an additional amount for Superfund-related activities from the Interior/Environment appropriations bill. Those two bills provide NIH's discretionary budget authority.56 In addition, NIH receives mandatory funding of $150 million annually that is provided in the Public Health Service (PHS)PHS Act for a special program on type 1 diabetes research and funding from a PHS Act transfer. The total funding available for NIH activities, taking account of add-ons and transfers, is known as the NIH program level.
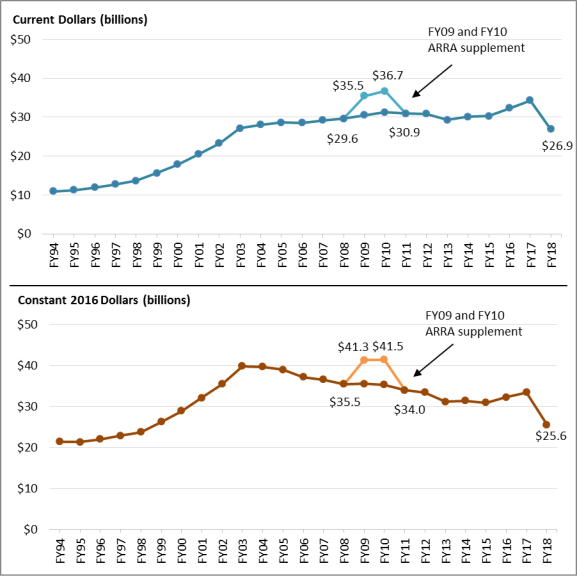
Table 1 outlines NIH program level funding over the past 25 years, and Figure 1 illustrates funding trends in both current (also called nominal dollars) and projected constant (i.e., inflation-adjusted) 20162019 dollars. Between FY1994 and FY1998, funding for NIH grew from $11.0 billion to $13.7 billion in nominal terms. Over the next five years, Congress and the President doubled the NIH budget to $27.2 billion in FY2003. In each of these years, NIH received annual funding increases of 14% to 16%. Since FY2003, NIH funding has increased more gradually in nominal dollars. Funding peaked in FY2010 before declining in FY2011 through FY2013, with increases in subsequent years.67 In some years, funding for the agency decreased in nominal dollars. For instance:
- the FY2006 total was 0.1% lower than the previous year, the first time that the NIH appropriation had decreased since FY1970;
- the FY2011 total, provided in the Full-Year Continuing Appropriations Act, 2011 (P.L. 112-10), was 1.0% below the previous year; and
- the FY2013 total, provided in the Consolidated and Further Continuing Appropriations Act, 2013 (P.L. 113-6), was reduced by the March 2013 sequestration and a transfer of funding under the authority of the HHS Secretary ($1.553 billion and $173 million respectively), resulting in a budget that was 5.0% lower than the prior year.
7
8The NIH program level in FY2016 was $32FY2018 is $37.311 billion, which includedincludes $77 million for Superfund-related research and the $150 million in diabetes research funding.89 The Consolidated Appropriations Act, 20162018 (H.R. 20291625, P.L. 114-113), provided $32115-141), provides $37.084 billion for NIH in Division H (the LHHS appropriations act): $31.304 billion for the NIH institutes and centers (ICs) plus $780 million in funding via the PHS Act transfer.9
For FY2017, the Obama Administration requested an NIH program level total of $33.136 billion (including $77 million for Superfund and $150 million for diabetes research), an increase of $825 million (2.6%) over FY2016. The House FY2017 LHHS appropriations bill (H.R. 5926) would have provided NIH with a total of $33.334 billion, including $792 million in funding via the PHS Act transfer. Adding to this total the amounts for Superfund-related activities ($77 million) and the mandatory type 1 diabetes program ($150 million) would have brought the FY2017 NIH program level to $33.561 billion. The Senate FY2017 LHHS appropriations bill (S. 3040) would have provided NIH with a total of $34.084 billion, including $857 million provided by the PHS Act transfer and an estimated $300 million in new funding from the HHS Non-recurring Expenses Fund (NEF).10 Adding to this total the amounts for Superfund-related activities ($77 million) and the mandatory type 1 diabetes program ($150 million) would have brought the FY2017 NIH program level to $34.311 billion.
Temporary funding for NIH in FY2017 was provided until May 5, 2017, by three continuing resolutions (CRs, P.L. 114-223, P.L. 114-254, and P.L. 115-30). Generally, these CRs provided a formulaic extension of FY2016 funding levels with an across-the-board adjustment and limited exceptions for particular accounts and activities. One exception is that Section 194 of the second CR appropriated $352 million (available until expended) into an NIH Innovation account to carry out four NIH Innovation Projects as described in Section 1001(b)(4) of the 21st Century Cures Act (P.L. 114-255).11 The Cures Act created the NIH Innovation account and specified that funds in the account must be appropriated in order to be available for expenditure; the appropriation in Section 194 of the second CR was needed to fulfill this requirement. The projects authorized by the Cures Act are: the Precision Medicine Initiative, the BRAIN Initiative, cancer research, and regenerative medicine using adult stem cells.
The explanatory statement accompanying the FY2017 LHHS appropriation (Division H of H.R. 244; P.L. 115-31) states that it provides $34.084 billion for NIH activities, a $2 billion (6.2%) increase over FY2016. This amount is calculated by including the $824 million from the evaluation tap as well as $352 million for the NIH Innovation account that was previously appropriated to the agency for FY2017. Adding the amounts for Superfund-related activities ($77 million in Division G of H.R. 244; P.L. 115-31) and the mandatory type 1 diabetes program ($150 million) brings the FY2017 NIH program level to $34.311 billion.
President Trump's FY2018 budget requests an NIH program level total of $26.92 billion, a decrease of $7.391 billion (-21.5%) compared with FY2017 enacted.12 Under the FY2018 budget request, all NIH ICs would receive a decrease compared to FY2017, but the Fogarty International Center would be eliminated and the Office of the NIH Director would retain $25 million in international research and related activities. The Trump budget request also proposes the consolidation of the Agency for Healthcare Research and Quality (AHRQ) with NIH, forming a new institute, the National Institute for Research on Safety and Quality (NIRSQ). The FY2018 budget proposal includes $272 million in budget authority for NIRSQ "to preserve key research activities previously carried out by AHRQ."13 NIRSQ is also projected to receive $107 million in mandatory resources from the Patient-Centered Outcomes Research Trust Fund to continue the targeted dissemination of study results to help patients and providers make better-informed health care decisions.14
The lower half of Figure 1 portrays NIH funding adjusted for inflation (in constant 2016 dollars) using the Biomedical Research and Development Price Index (BRDPI).15 It shows that the purchasing power of NIH funding (non-ARRA) peaked in FY2003 (the last year of the five-year doubling period) and then steadily declined for more than a decade until back-to-back funding increases were provided in FY2016 and FY2017. In constant 2016 dollars, the FY2018 program level request for NIH is 35.9% less than the program level in FY2003.
Program Level Funding in Current and Constant (2016) Dollars President Trump's FY2019 budget requests an NIH program level total of $34.767 billion, a decrease of $2.544 billion (-6.8%) compared with FY2018 enacted.11 One account, Buildings and Facilities, would receive a 55% increase in funding for FY2019 compared to FY2018, and OD would receive a smaller increase; all other accounts for the NIH Institutes and Centers would receive a decrease compared to FY2018. Note that final FY2018 appropriations had not been enacted during the period in which the FY2019 President's request was being formulated. While the total request for NIH represents a decrease from FY2018-enacted levels, it represents an increase from FY2017-enacted levels and the FY2018 continuing resolution levels that were in place at the time FY2019 request levels were being determined.
Figure 1. National Institutes of Health (NIH) Funding, FY1994-FY2019 Request Program Level Funding in Current and Projected Constant (2019) Dollars
|
|
 |
|
|
Sources: NIH Budget Office, Appropriations History by Institute/Center (1938 to Present), at http://officeofbudget.od.nih.gov/approp_hist.html Notes: Program level includes all budget authority including appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002-FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. |
Table 1. NIH Funding, FY1994–FY2018FY2019 Request
Program Level Funding in Current and Constant (20162019) Dollars (billions)
|
Fiscal Year |
Program Level |
% Change |
Program Level Projected Constant |
% Below 2003 |
||||
|
1994 |
$10.956 |
$21.451 |
||||||
|
1995 |
11.300 |
3.1% |
21.383 |
|||||
|
1996 |
11.928 |
5.6% |
22.008 |
|||||
|
1997 |
12.741 |
6.8% |
22.873 |
|||||
|
1998 |
13.675 |
7.3% |
23.745 |
|||||
|
1999 |
15.629 |
14.3% |
26.305 |
|||||
|
2000 |
17.841 |
14.1% |
28.948 |
|||||
|
2001 |
20.459 |
14.7% |
32.128 |
|||||
|
2002 |
23.321 |
14.0% |
35.450 |
|||||
|
2003 |
27.167 |
16.5% |
39.893 |
|||||
|
2004 |
28.037 |
3.2% |
39.691 |
-0.5% |
||||
|
2005 |
28.594 |
2.0% |
38.965 |
-2.3% |
||||
|
2006 |
28.560 |
-0.1% |
37.197 |
-6.8% |
||||
|
2007 |
29.179 |
2.2% |
36.613 |
-8.2% |
||||
|
2008 |
29.607 |
1.5% |
35.489 |
-11.0% |
||||
|
2009 |
30.545 |
3.2% |
35.572 |
-10.8% |
||||
|
2010 |
31.238 |
2.3% |
35.305 |
-11.5% |
||||
|
2011 |
30.916 |
-1.0% |
33.970 |
-14.8% |
||||
|
2012 |
30.861 |
-0.2% |
33.480 |
-16.1% |
||||
|
2013 |
29.316 |
-5.0% |
31.219 |
-21.7% |
||||
|
2014 |
30.143 |
2.8% |
31.425 |
-21.2% |
||||
|
2015 |
30.311 |
0.6% |
30.970 |
-22.4% |
||||
|
2016 |
32.311 |
6.6% |
32.311 |
-19.0% |
||||
|
2017 |
34.311 |
6.2% |
33.441 |
-16.2% |
||||
|
2018
37.311 8.7% 38.349 -11.2% |
26.920 |
- |
25.551 |
- |
||||
|
NIH Funding |
||||||||
|
2009 |
35.499 |
40.546 |
||||||
|
2010 |
36.684 |
40.663 |
||||||
Source: NIH Budget Office, Appropriations History by Institute/Center (1938 to Present), at http://officeofbudget.od.nih.gov/approp_hist.html. FY2017 is the enacted amount, FY2018 request ishttp://officeofbudget.od.nih.gov/approp_hist.html. FY2017 and FY2018 enacted amounts are from the Explanatory Statement on the Consolidated Appropriations Act, FY2018 (H.R. 1625, P.L. 115-141), in the March 22, 2018 Congressional Record, pp. H2681, H2733-H2735. FY2019 request amounts are from Department of Health and Human Services, Fiscal Year 20182019 Budget in Brief, Washington, DC, May 2017, p. 36February 2018, p. 40. Inflation adjustment reflects the Biomedical Research and Development Price Index (BRDPI), updated February 2017January 2018, https://officeofbudget.od.nih.gov/gbiPriceIndexes.html.
Notes: Amounts in table may differ from actuals in many cases. By convention, budget tables, such as Table 1 do not subtract the amount of PHS Act transfers from the agencies' funding. Program Level includes all budget authority, including appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002-FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. ARRA supplementary funding is from the American Recovery and Reinvestment Act of 2009, P.L. 111-5. In general, amounts provided to NIH for emergency requirements are excluded from these totals (e.g., FY2015 amount does not include $238,000,000 for the National Institute for Allergy and Infectious Diseases (NIAID[NIAI]) for research on Ebola that was provided in P.L. 113-235, Title VI of Division G.
Author Contact Information
Footnotes
| 1. |
The Public Health Service also includes the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality (AHRQ), the Health Resources and Services Administration (HRSA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Indian Health Service (IHS), and the Agency for Toxic Substances and Disease Registry (ATSDR).
|
|
|
Department of Health and Human Services, Fiscal Year 2018 Budget in Brief, Washington, DC, May 2017, p. 38. |
||
|
Ibid. |
||
|
Ibid. |
||
|
NIH received a total of $10.4 billion in supplemental, one-time FY2009 appropriations in the American Recovery and Reinvestment Act (ARRA) of 2009 (P.L. 111-5). ARRA funds were made available for obligation for two years; $4.95 billion was obligated in FY2009, and $5.45 billion in FY2010. CRS Report R43304, Public Health Service Agencies: Overview and Funding (FY2010-FY2016). |
||
|
Amounts shown in Table 1 include appropriations for the Global Fund to Fight AIDS, TB, and Malaria (FY2002-FY2011) that were subject to transfer-out. As of FY2012, NIH no longer receives appropriations for the National Institute of Allergy and Infectious Diseases (NIAID) identifying resources for the Global Fund; this responsibility was transferred to another federal agency. For further details on the amounts transferred out by fiscal year, see the "Supplemental Appropriation Data Table" for "History of Congressional Appropriations, Fiscal Years 2000-2012" at http://officeofbudget.od.nih.gov/approp_hist.html. |
||
|
The FY2012 amount of $30.861 billion appears to be 0.2% below the FY2011 amount of $30.916 billion. However, the FY2011 amount includes $297.3 million that was subject to transfer-out for the Global Fund to Fight AIDS, TB, and Malaria. |
||
|
||
|
NIH and other HHS agencies and programs authorized under the PHS Act are subject to a budget assessment called the PHS Program Evaluation Set-Aside, also called the evaluation tap. Section 241 of the PHS Act (42 U.S.C. §238j) authorizes the Secretary of HHS to use a portion of eligible appropriations to study the effectiveness of federal health programs |
||
| 10. |
The HHS Secretary is authorized to transfer to the NEF unobligated balances of certain expired discretionary funds. Under current law, NEF funds are available until expended for use by the HHS Secretary for capital acquisitions including facility and information technology infrastructure. Congressional appropriators must be notified in advance of any planned use of NEF funds. NEF funds have been used by HHS for expenses related to the Affordable Care Act, such as the federally facilitated exchanges. (See CRS Report R43066, Federal Funding for Health Insurance Exchanges.) S. 3040 included language that would have repurposed a portion of the NEF for NIH biomedical research activities. H.R. 5926 would have terminated the NEF and rescinded unobligated balances. |
|
| 11. |
For further information, see CRS Report R44720, The 21st Century Cures Act (Division A of P.L. 114-255) and CRS Report R44723, Overview of Further Continuing Appropriations for FY2017 (H.R. 2028). |
|
| 12. |
The proposed decrease to the NIH program level would be larger (-22.5%, rather than -21.5%) if the FY2017 NIH program level were adjusted to include FY2017 funding for the Agency for Healthcare Research and Quality (AHRQ). This adjustment would make the FY2017 estimate more comparable with the FY2018 request level, given the FY2018 President's budget proposal to consolidate AHRQ functions within NIH. |
|
| 13. |
Department of Health and Human Services, Fiscal Year 2018 Budget in Brief, Washington, DC, May 2017, p. 37, https://www.hhs.gov/sites/default/files/Consolidated%20BIB_ONLINE_remediated.pdf. |
|
| 14. |
Ibid., p. 42. |
|
|
|
12.
The FY2019 request level does not reflect the proposal to allocate an additional $750 million to NIH for opioid-related activities from the $10 billion in requested HHS-wide funding. The FY2019 request level is as shown in HHS, Fiscal Year 2019 Budget in Brief, Washington, DC, February 2018, p. 40, https://www.hhs.gov/sites/default/files/fy-2019-budget-in-brief.pdf. |
The index is developed for NIH by the Bureau of Economic Analysis of the Department of Commerce. It reflects the increase in prices of the resources needed to conduct biomedical research, including personnel services, supplies, and equipment. It indicates how much the NIH budget must change to maintain purchasing power. See "NIH Price Indexes," at |