Health Insurance Exchanges and Qualified Health Plans: Overview and Policy Updates
Changes from June 20, 2018 to February 16, 2021
This page shows textual changes in the document between the two versions indicated in the dates above. Textual matter removed in the later version is indicated with red strikethrough and textual matter added in the later version is indicated with blue.
Contents
- Introduction
- Types of Exchanges
- Individual and SHOP Exchanges
- State-Based and Federally Facilitated Exchanges
- Facilitating Purchase of Coverage
- Individual Exchanges
- Eligibility and Enrollment Process
- Enrollment Periods and Enrollment Estimates
- Premium Tax Credits and Cost-Sharing Reductions
- SHOP Exchanges
- Eligibility and Enrollment Process
- Changes in SHOP Exchange Web Portal Functionality
- Enrollment Periods and Enrollment Estimates
- Small Business Health Care Tax Credit
- Individual and SHOP Exchange Enrollment Assistance
- Administering the Exchanges
- Qualified Health Plans
- Types of QHPs and Other Plans Offered Through Exchanges
- Exchange Funding
- Further Reading
Tables
Summary
The Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) requires health insurance exchanges to be established in every state. Exchanges are marketplaces in which consumers and small businesses can shop for and purchase private health insurance coverage. In general, states must have two types of exchanges: an individual exchange and a small business health options program (SHOP) exchange.
Exchanges may be established either by the state itself as a state-based exchange (SBE) or by the Secretary of Health and Human Services (HHS) as a federally facilitated exchange (FFE). Some states have SBE-FPs: they have SBEs but use the federal information technology platform, including the federal exchange website www.Healthcare.gov. In states with FFEs, the exchange may be operated by the federal government alone or in conjunction with the state. States may have different structures for their individual and SHOP exchanges.
Consumers who obtain coverage through the individual exchange may be eligible for financial assistance from the federal government. Financial assistance in the individual exchanges is available in two forms: Overview of Health Insurance Exchanges
February 16, 2021
The Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) required health insurance exchanges to be established in every state. Exchanges are
Vanessa C. Forsberg
virtual marketplaces in which consumers and smal business owners and employees can
Analyst in Health Care
shop for and purchase private health insurance coverage and, where applicable, be
Financing
connected to public health insurance programs (e.g., Medicaid). In general, states must
have two types of exchanges: an individual exchange and a small business health
options program (SHOP) exchange. Exchanges may be established either by the state itself as a state-based exchange (SBE) or by the Secretary of Health and Human Services (HHS) as a federally facilitated exchange (FFE). Some states have SBE-FPs: they have SBEs but use the federal information
technology platform (FP), including the federal exchange website www.HealthCare.gov.
A primary function of the exchanges is to facilitate enrollment. This general y includes operating a web portal that
al ows for the comparison and purchase of coverage; making determinations of eligibility for coverage and financial assistance; and offering different forms of enrollment assistance, including Navigators and a cal center. Exchanges also are responsible for several administrative functions, including certifying the plans that wil be
offered in their marketplaces.
The ACA general y requires that the private health insurance plans offered through an exchange are qualified health plans (QHPs). To be a certified as a QHP, a plan must be offered by a state-licensed health insurance issuer and must meet specified requirements, including covering the essential health benefits (EHB). QHPs sold in the individual and SHOP exchanges must comply with the same state and federal requirements that apply to QHPs
and other health plans offered outside of the exchanges in the individual and smal -group markets, respectively. Additional requirements apply only to QHPs sold in the exchanges. Exchanges also may offer variations of QHPs,
such as child-only or catastrophic plans, and non-QHP dental-only plans.
Individuals and smal businesses must meet certain eligibility criteria to purchase coverage through the individual and SHOP exchanges, respectively. There is an annual open enrollment period during which any eligible consumer may purchase coverage via the individual exchanges; otherwise, consumers may purchase coverage only if they qualify for a special enrollment period. In general, smal businesses may enroll at any time during the year. There are plans available in al individual exchanges, and, as of February 2020, about 10.7 mil ion people
obtained health insurance through the individual exchanges. (2021 open enrollment data for al states are expected in spring 2021.) Nationwide SHOP exchange enrollment estimates are not regularly released; in addition, there are
no SHOP exchange plans available in more than half of states in 2021.
Plans sold through the exchanges, like private health insurance plans sold off the exchanges, have premiums and out-of-pocket (OOP) costs. Consumers who obtain coverage through the individual exchange may be eligible for federal financial assistance with premiums and OOP costs in the form of premium tax credits and cost-sharing reductions. Small reductions. Smal businesses that use the SHOP exchange may be eligible for small business health insurance tax credits. The tax credits assist small businesses
credits that assist with the cost of providing health insurance coverage to employees.
The ACA generally requires that health insurance plans offered through an exchange are qualified health plans (QHPs). To be a certified as a QHP, a plan must be offered by a state-licensed issuer and must meet specified requirements, including covering the essential health benefits (EHB). QHPs sold in
The federal government spent an estimated $1.8 bil ion on the operation of exchanges in FY2020, and it projected $1.2 bil ion in spending for FY2021. Much of the federal spending on the exchanges is funded by user fees paid by the insurers who participate in FFE and SBE-FP exchanges. States with SBEs finance their own exchange
administration; states with SBE-FPs also finance certain costs (e.g., consumer outreach and assistance programs,
including Navigator programs).
This report provides an overview of the various components of the health insurance exchanges. It begins with summary information about the types of exchanges and their administration. Sections on the individual and SHOP exchanges discuss eligibility and enrollment, plan costs and financial assistance available to eligible consumers and smal businesses, insurer participation, and other topics. The final sections address types of enrollment assistance available to exchange consumers and federal funding for the exchanges.
Congressional Research Service
link to page 5 link to page 6 link to page 6 link to page 6 link to page 7 link to page 9 link to page 10 link to page 11 link to page 11 link to page 12 link to page 12 link to page 14 link to page 15 link to page 16 link to page 18 link to page 21 link to page 23 link to page 23 link to page 24 link to page 24 link to page 26 link to page 26 link to page 26 link to page 27 link to page 28 link to page 28 link to page 28 link to page 30 link to page 30 link to page 30 link to page 31 link to page 31 link to page 31 link to page 33 link to page 33 link to page 9 link to page 21 link to page 32 link to page 32 Overview of Health Insurance Exchanges
Contents
Introduction ................................................................................................................... 1 Overview ....................................................................................................................... 2
Types and Administration of Exchanges ........................................................................ 2
Individual and SHOP Exchanges ............................................................................ 2 State-Based and Federal y Facilitated Exchanges ...................................................... 3 Exchange Administration....................................................................................... 5
Qualified Health Plans................................................................................................ 6
Individual Exchanges ...................................................................................................... 7
Eligibility and Enrollment ........................................................................................... 7
Interaction with Medicaid, CHIP, and Medicare ........................................................ 8
Open and Special Enrollment Periods ...................................................................... 8 Special Enrollment Periods and COVID-19 ............................................................ 10 Enrollment Estimates .......................................................................................... 11
Premiums and Cost Sharing ...................................................................................... 12
Premium Tax Credits and Cost-Sharing Reductions ................................................. 14
Insurer Participation................................................................................................. 17
SHOP Exchanges .......................................................................................................... 19
Eligibility and Enrollment ......................................................................................... 19
Enrollment Periods ............................................................................................. 20
Online Enrollment versus Direct Enrollment........................................................... 20 Enrollment Estimates .......................................................................................... 22 Congressional Member and Staff Enrollment via the D.C. SHOP Exchange ................ 22
Premiums and Cost Sharing ...................................................................................... 22
Smal Business Health Care Tax Credit .................................................................. 23
Insurer Participation................................................................................................. 24
Exchange Enrollment Assistance ..................................................................................... 24
Navigators and Other Exchange-Based Enrollment Assistance........................................ 24
Brokers, Agents, and Other Third-Party Assistance Entities ............................................ 26
Exchange Spending and Funding ..................................................................................... 26
Initial Grants for Exchange Planning and Establishment ................................................ 26 Ongoing Federal Spending on Exchange Operation....................................................... 27
Funding Sources for Federal Exchange Spending ......................................................... 27
User Fees Collected from Participating Insurers ...................................................... 27 Other Federal Funding Sources............................................................................. 29
State Financing of the Exchanges ............................................................................... 29
Figures Figure 1. Individual and SHOP Exchange Types by State, Plan Year 2021................................ 5 Figure 2. Plan Year 2021 Insurer Participation in the Individual Exchanges, by County............ 17 Figure 3. Federal User Fee for Insurers Participating in Specified Types of Individual
Exchanges, by Plan Year.............................................................................................. 28
Congressional Research Service
link to page 42 link to page 42 link to page 13 link to page 13 link to page 16 link to page 18 link to page 20 link to page 20 link to page 35 link to page 39 link to page 43 link to page 44 link to page 34 link to page 39 link to page 41 link to page 44 link to page 46 Overview of Health Insurance Exchanges
Figure C-1. Centers for Medicare & Medicaid Services “Health Insurance Exchanges
Transparency Table,” FY2021 ...................................................................................... 38
Tables Table 1. Open Enrollment Periods for Individual Exchanges on the Federal Platform, by
Plan Year .................................................................................................................... 9
Table 2. Nationwide Individual Exchange Enrollment Estimates, by Plan Year ....................... 12 Table 3. Annual Out-of-Pocket Limits, by Plan Year ........................................................... 14 Table 4. Data on Premiums, Advance Premium Tax Credits, and Cost-Sharing Reductions
Nationwide, by Plan Year ............................................................................................ 16
Table A-1. Exchange Types and Key Details by State, Plan Year 2021 ................................... 31 Table B-1. Types of Plans Offered Through the Exchanges .................................................. 35 Table C-1. CMS Federal Exchange Funding Sources for Specified Fiscal Years ...................... 39 Table D-1. HHS “Notice of Benefits and Payment Parameters,” Final Rule by Year................. 40
Appendixes Appendix A. Exchange Information by State ..................................................................... 30 Appendix B. Types of Plans Offered Through the Exchanges ............................................... 35 Appendix C. Exchange Spending and Funding Details from CMS Budget Justifications .......... 37 Appendix D. Additional Resources .................................................................................. 40
Contacts
Author Information ....................................................................................................... 42
Congressional Research Service
link to page 16 Overview of Health Insurance Exchanges
Introduction The Patient Protection and Affordable Care Act (ACA; exchanges must comply with the same state and federal requirements that apply to QHPs and other health plans offered outside of the exchanges in the individual and small-group markets, respectively. Exchanges also may offer variations of QHPs, such as child-only or catastrophic plans, and non-QHP dental-only plans.
This report provides an overview of the various components of the health insurance exchanges. It begins with summary information about how exchanges are structured and then discusses both individual and SHOP exchanges in terms of eligibility and enrollment, financial assistance for certain exchange consumers and small businesses, and enrollment assistance entities. The report also describes exchanges' role in certifying plans as qualified to be sold in their marketplaces and outlines the range of plans offered through exchanges. Finally, the report briefly addresses funding for the exchanges. Where applicable, the report references other CRS reports that have more information on various topics.
Introduction
The Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) requires required health insurance exchanges (also known as marketplaces) to be established in every state. ACA The ACA
exchanges are virtual marketplaces in which consumers and small smal businesses can shop for and purchase private health insurance coverage and, where applicable, be connected to public health insurance programs (e.g., Medicaid).1 1 Certain consumers and small employers are eligible for financial assistance for private health insurance purchased (only) through the exchanges. Exchanges are intended to simplify the experience of obtaining health insurance. They are not intended to supplant the private market outside of the exchanges but rather to provide an
additional source of private health insurance coverage options.
This report provides an overview of key aspects of the health insurance exchanges. The report includes summary information about the major functions of exchanges and how they are structured. It describes individual and small business eligibility and enrollment processes, provides enrollment estimates, explains the financial assistance available to certain consumers and small businesses, and discusses consumer enrollment assistance options. The report also reviews the role of exchanges in certifying participating plans and outlines the range of plans offered through exchanges. It briefly addresses funding for the exchanges. It provides a high-level description of these exchange-related topics while referencing other CRS reports with further information on specific topics, including on topics related to market stabilization policy considerations.
Types of Exchanges
The exchanges may be administered by state governments and/or the federal government.
Regardless, the major functions of the exchanges are (1) to facilitate consumers’ and smal businesses’ purchase of coverage (by operating a web portal, making determinations of eligibility for coverage and any financial assistance, and offering different forms of enrollment assistance) and (2) to certify, recertify, and otherwise monitor the plans that are offered in those
marketplaces.
Although a relatively smal proportion of people in the U.S. obtain their coverage through the exchanges,2 the administration and functioning of these marketplaces are ongoing topics of interest to congressional audiences and other stakeholders. An understanding of the exchanges
can provide context for current health policy discussions and proposals related to health care coverage and costs, the roles of the public and private sectors in the provision of health coverage,
and more.
This report provides an overview of key aspects of the health insurance exchanges. It begins with summary information about types and administration of exchanges and the plans sold in them. Sections on the individual and smal business exchanges discuss eligibility and enrollment, plan costs and financial assistance available to eligible consumers and smal businesses, insurer participation, and other topics. The final sections describe types of enrollment assistance available
to exchange consumers and provide information on federal funding for the exchanges.
Appendixes offer further details, including exchange types by state.
1 In this report, the terms consumers and individuals generally are used interchangeably, as are small businesses and sm all em ployers.
2 For example, as of February 2020, about 10.7 million people obtained health insurance through the individual exchanges. T his figure is approximately 3% of the current U.S. population of 330 million people. See Table 2 regarding exchange enrollment estimates and sources. For current U.S. population, see U.S. Census, “U.S. and World Population Clock,” accessed September 2, 2020, at https://www.census.gov/popclock/.
Congressional Research Service
1
link to page 18 link to page 27 Overview of Health Insurance Exchanges
Overview
Types and Administration of Exchanges
Individual and SHOP Exchanges
The ACA Individual and SHOP Exchanges
The ACA required health insurance exchanges to be established in all al states and the District of Columbia (DC).Columbia.3 In general, the health insurance exchanges began operating in October 2013 to allow al ow
consumers to shop for health insurance plans that began as soon as January 1, 2014.
Most states have
There are two types of exchanges—an individual exchangeexchanges and a small business health options program (SHOP) exchange.2exchanges.4 These exchanges are part of the individual (also cal ed non-group) and smal -group segments of the private health insurance market, respectively.5 In an individual exchange, eligible consumers can compare and purchase non-group insurance for themselves and
their families and can apply for premium tax credits (PTCs) and cost-sharing reductions.3subsidies (see “Premium Tax Credits and Cost-Sharing Reductions,” below). In a SHOP exchange, small smal businesses can compare and purchase smallsmal -group insurance and can apply for small smal business health insurance tax credits (“Smal Business Health Care Tax Credit,” below); in addition, employees of small smal businesses can enroll in plans offered by their employers on a SHOP exchange.4 Besides facilitating consumers' and small businesses' purchase of coverage (by operating a web portal, making determinations of eligibility for coverage and any financial assistance, and offering different forms of enrollment assistance), the other major function of the exchanges is to certify, recertify, and otherwise monitor the plans that participate in those marketplaces. Individual and SHOP exchanges can be operated by either the state or the federal government, as described below.
exchange.
Each exchange covers a whole state.6 Within a given exchange, private insurers may offer plans that cover the whole state or only certain areas within the state (e.g., one or more counties). Plans
sold within a given exchange may cover services offered by providers located in more than one
state.
In general, consumers and smal businesses may obtain coverage within their state’s individual or SHOP exchange, respectively, or they may shop in the individual or smal -group health insurance markets outside of the exchanges, which existed prior to the ACA and continue to exist.7 Outside of the ACA exchanges, consumers can purchase coverage through agents or brokers, or they can purchase it directly from insurers. In addition, there were and stil are privately operated websites that al ow the comparison and purchase of coverage sold by different insurers, broadly similar in
concept to the ACA exchanges.8
3 T he Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) also gave the territories the option of establishing exchanges, but none elected to do so, by th e statutory deadline of October 1, 2013. See 42 U.S.C. §18043. 4 T he term individual exchange is used for purposes of this report. It is not defined in exchange-related statute or regulations.
5 T he private health insurance market includes both the group market (largely made up of employer-sponsored insurance) and the individual m arket (which includes plans directly purchased from an insurer). T he group market is divided into small- and large-group market segments; a sm all group is typically defined as a group of up to 50 individuals (e.g., employees), and a large group is typically defined as one with 51 or more individuals.
6 T here is an option for states to coordinate in administering regional exchanges or for a single state to establish subsidiary exchanges that serve geographically distinct areas (see 45 C.F.R. §155.410) , but none have done so. 7 However, plans are not available in all small business health options program (SHOP) exchanges in 2021. 8 An example of a privately owned website that allows for comparison and purchase of coverage from different insurers is ehealthinsurance.com. Note that some types of coverage sold outside of the federal and state exchanges, potentially including some types of coverage available on private sites like t his one, are not subject to some or all federal health insurance requirements. For more information, see CRS Report R46003, Applicability of Federal Requirem ents to Selected Health Coverage Arrangem ents.
Congressional Research Service
2
link to page 28 link to page 28 link to page 44 link to page 24 Overview of Health Insurance Exchanges
State-Based and Federally Facilitated Exchanges
State-Based and Federally Facilitated Exchanges
A state can choose to establish its own state-based exchange (SBE). If a state opts not to administer its own exchange, or if the Department of Health and Human Services (HHS) determines that the state is not in a position to do so, then HHS is required to establish and administer
the exchange in the state as a federally facilitated exchange (FFE). States also
There is one variation on the SBE approach: a state may have a state-based exchange using a federal platform (SBE-FP), which means they have an SBE but use the federally the state oversees the exchange but uses the federal y
facilitated information technology (IT) platform, or federal platform (FP) (i.e., HealthCare.gov).
There is also a variation on the FFE approach: a state may have a state partnership FFE, which al ows the state to manage certain aspects of its exchange while HHS manages the remaining aspects and has authority over the exchange. In early guidance on this option, HHS indicated a
state could elect to perform some plan management and/or certain consumer assistance functions, and HHS would perform other functions, including facilitating enrollment through the federal HealthCare.gov platform and funding Navigator entities in the state.9 In federal and private resources that track exchange data, this variation may not be reported on separately but rather
may be included in overal counts of FFEs, which is the model this report general y follows.10
In rulemaking finalized January 19, 2021 (the 2022 Notice of Benefit and Payment Parameters, or “Payment Notice”11), HHS and the Department of the Treasury established new “direct enrollment” variations of the exchange types: FFE-DE, SBE-DE, and SBE-FP-DE.12 States
electing these options would “adopt a private sector-based enrollment approach as an alternative to the consumer-facing enrollment website operated by the Exchange (for example, HealthCare.gov for the FFEs).” In other words, consumers would enroll in exchange plans via private agents or brokers, rather than on an exchange website like HealthCare.gov. The exchange would stil have to “make available a website listing basic [qualified health plan] QHP
information for comparison,” but this website would direct consumers to “approved partner websites for consumer shopping, plan selection, and enrollment activities.” Per the final rule, this wil be an option for SBEs as of plan year (PY) 2022, and for FFEs and SBE-FPs as of PY2023. The final rule was published but did not take effect before the presidential transition, and as such,
may be reconsidered by the Biden Administration.13
9 See Centers for Medicare & Medicaid Services (CMS) Center for Consumer Information and Insurance Oversight (CCIIO), “General Guidance on Federally-facilitated Exchanges,” May 16, 2012, at https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/Downloads/ffe-guidance-05-16-2012.pdf. Also see CMS, CCIIO, “ Guidance on State Partnership Exchange,” January 3, 2013, at https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/Downloads/partnership-guidance-01-03-2013.pdf. For more information about Navigators, see “ Navigators and Other Exchange-Based Enrollment Assistance” in this report.
10 T his report focuses on the three types of exchanges that are commonly discussed in CMS resources, but other entities may also track states with variations of state partnership FFEs. For example, the Kaiser Family Foundation (KFF) notes FFEs in which the state conducts plan management activities at “ State Health Insurance Marketplace T ypes, 2021,” at https://www.kff.org/health-reform/state-indicator/state-health-insurance-marketplace-types/. 11 See 2022 Payment Notice, starting page 6143, regarding information in this paragraph. T he Notice of Benefits and Payment Parameters, or Payment Notice, is an annually published rule that includes updates and policy changes related to the exchanges and private health insurance. See Table D-1 for Payment Notice citations.
12 For additional discussion of direct enrollment, see “ Online Enrollment versus Direct Enrollment” in the SHOP section of this report.
13 See Office of Management and Budget, “Memorandum for the Heads of Executive Departments and Agencies,” 86 Federal Register 7424, January 28, 2021.
Congressional Research Service
3
link to page 9 link to page 35 link to page 35 link to page 24 link to page 28 Overview of Health Insurance Exchanges
For PY2021, 30 states have FFEs, 15 states have SBEs, and 6 states have SBE-FPs.14 A few states have changed approaches one or more times (e.g., initial y worked to create an SBE but then switched to an SBE-FP or FFE model). Changes in the first few years varied in terms of whether the state moved toward more or less federal involvement, but in several cases, a state transitioned from a fully state-based approach to an SBE-FP (i.e., transitioned toward more federal involvement). Recent and ongoing transitions are general y in the direction of less federal
involvement. As of the publication of this report, five states are transitioning or considering
transitions for PY2022 or beyond.15
SHOP exchanges may be federal y facilitated (FF-SHOP) or state-based (SB-SHOP).16 For PY2021, there are 32 FF-SHOPs and 18 SB-SHOPs. However, in more than half of these states, no insurers are offering medical plans in the SHOP exchange, meaning there is effectively no SHOP exchange there.17facilitated information technology (IT) platform (i.e., HealthCare.gov).
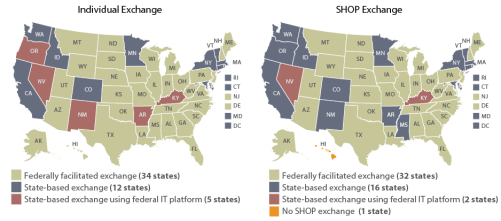
For the 2018 plan year, 34 states have FFEs, 12 states have SBEs, and 5 states have SBE-FPs.5 In addition, state involvement in the FFEs may vary. In many states with FFEs, the exchange is wholly operated and administered by HHS. But in some cases, states partner with HHS to perform some functions, such as plan management or consumer assistance.6
Like the individual exchanges, SHOP exchanges may be federally facilitated (FF-SHOP; 32 states), state-based (SB-SHOP; 16 states), or state-based using the federal IT platform (SB-FP-SHOP; 2 states).7 One state is exempted from operating a SHOP exchange.8 For the 2018 One state is exempted from operating a SHOP exchange.18 For the 2021 plan year, most states'’ individual and SHOP exchanges are administered in the same way (i.e., both state-based or both federallyfederal y facilitated). However, a handful of states have different
approaches for their individual and SHOP exchanges.
See Figure 1 andSome resources refer to this as a bifurcated
approach.
See Figure 1 for individual and SHOP exchange types by state in PY2021, and see Table A-1 for
additional information, including on state transitions to different exchange types.
14 See Table A-1 for details and citations for this paragraph. In tallies throughout this report, the District of Columbia is counted as a state.
15 One of these states, Georgia, received approval through the Section 1332 state innovation waiver process shift to its own Georgia Access Model, essentially a direct enrollment approach, beginning in PY2023. T his 1332 process allows states to waive specified ACA provisions, including provisions related to the establishment of health insurance exchanges and related activities. See CRS Report R44760, State Innovation Waivers: Frequently Asked Questions for more information.
16 As of June 2018, states can no longer select a state-based SHOP using the federal IT platform (SB-FP-SHOP) approach, except that the two states with that model at that time (Nevada and Kentucky) could maintain it. According to CMS, those states no longer use that model. For more information, see “ Online Enrollment versus Direct Enrollment in the SHOP section of this report.
17 See “Insurer Participation” in the SHOP Exchanges section of this report for more information. 18 Hawaii received a Section 1332 waiver exempting it from operating a SHOP exchange.
Congressional Research Service
4
link to page 35 link to page 6 link to page 6 link to page 28 link to page 10
Overview of Health Insurance Exchanges
Figure 1. Individual and SHOP Exchange Types by State, Plan Year 2021
Sources: Congressional Research Service (CRS) il ustration. See data sources in Table A-1. Notes: SHOP = smal for the exchange types by state.
|
 |
|
Facilitating Purchase of Coverage
A primary function of the exchanges is to provide a way for consumers and small in this report regarding individual and SHOP exchanges, and federal and state administration of exchanges. In more than half of states, no insurers are offering medical plans in the SHOP exchange, meaning there is effectively no SHOP exchange there. These states have a circle symbol in the SHOP Exchange map above. See “Insurer Participation” in the SHOP Exchanges section of this report for more information. Hawai received a Section 1332 waiver exempting it from operating a SHOP exchange. For more information, see CRS Report R44760, State Innovation Waivers: Frequently Asked Questions.
Exchange Administration
Whether state-based or federal y facilitated, exchanges are required by law to fulfil certain minimum functions. ACA provisions related to the establishment and operation of the exchanges are codified at 42 U.S.C. §§18031 et seq. Other federal provisions also are relevant, for example
regarding the requirements for plans that may be sold through the exchanges.19
A primary function of the exchanges is to provide a way for consumers and smal businesses to compare and purchase health plan options offered by participating insurers.9
20 This general y includes operating a web portal that al ows for comparing and purchasing coverage, making
determinations of eligibility for coverage and financial assistance, and offering different forms of
enrollment assistance.
Exchanges also are responsible for several administrative functions, including certifying the plans that wil be offered in their marketplaces.21 This includes annual y certifying or recertifying plans to be sold in their exchanges as qualified health plans (QHPs, discussed below). QHP certification involves a review of various factors, including the plan’s benefits, cost-sharing structure, provider network, premiums, marketing practices, and quality improvement activities,
19 See “Qualified Health Plans” in this report. 20 42 U.S.C. §18031(b)(1)(A). 21 42 U.S.C. §18031(d)(4).
Congressional Research Service
5
link to page 12 link to page 16 link to page 16 link to page 16 Overview of Health Insurance Exchanges
to ensure compliance with applicable federal and state standards.22 The QHP certification process is to be completed each year in time for insurers to market their plans and premiums during the
exchanges’ annual open enrollment period (see “Open and Special Enrollment Periods”).
Exchanges’ other administrative activities include collecting enrollment and other data, reporting data to and otherwise interacting with the Departments of HHS and the Treasury, and working
with state insurance departments and federal regulators to conduct ongoing oversight of plans.
Qualified Health Plans In general, health insurance plans offered through exchanges must be qualified health plans (QHPs).23 A QHP is a plan offered by a state-licensed insurer that is certified to be sold in that state’s exchange, covers the essential health benefits (EHB) package, and meets other specified
requirements.24 Covering the EHB package means covering 10 broad categories of benefits and services, complying with limits on consumer cost sharing on the EHB, and meeting certain
generosity requirements (in terms of actuarial value).25
QHPs are subject to the same state and federal requirements that apply to health plans offered outside of exchanges.26 Thus, a QHP offered through an individual exchange must comply with state and federal requirements applicable to individual market plans; a QHP offered through a SHOP exchange must comply with state and federal requirements applicable to smal -group market plans. For example, the requirement to cover the EHB applies to individual and smal -
group plans both in and out of the exchanges.
There are additional requirements that apply only to QHPs sold in the exchanges. For example, an insurer wanting to sel QHPs in an exchange must offer at least one silver-level and one gold-
level plan in al of the areas in which the insurer offers coverage within that exchange. In addition, QHPs must meet network adequacy standards, including maintaining provider networks that are “sufficient in number and types of providers” and include “essential community
providers.”27
A QHP is the only type of comprehensive health plan an exchange may offer, but QHPs may be offered outside of exchanges, as wel . Besides standard QHPs, other types of plans may be available in a given exchange, including child-only plans, catastrophic plans, consumer operated and oriented plans (CO-OPs), and multi-state plans (MSPs). Technical y, these are also QHPs.
22 42 U.S.C. §18031(c)(1); 42 U.S.C. §18031(e). For more information, see, for example, CMS, CCIIO, “ Final 2021 Letter to Issuers in the Federally-facilitated Exchanges,” May 7, 2020, at https://www.cms.gov/CCIIO/Resources/Regulations-and-Guidance/Downloads/Final-2021-Letter-to-Issuers-in-the-Federally-facilitated-Marketplaces.pdf. Hereinafter referred to as “CMS 2021 Letter to Issuers.” 23 42 U.S.C. §18031(d)(2)(B). 24 42 U.S.C. §18021(a)(1). 25 42 U.S.C. §18022. For brief explanation of actuarial value (AV) and cost -sharing limits, see “ Premiums and Cost Sharing” in this report. For more information on the essential health benefits, cost-sharing limits, and AV requirements, see CRS Report R45146, Federal Requirem ents on Private Health Insurance Plans. 26 For more information about federal requirements applicable to different types of plans, see CRS Report R45146, Federal Requirem ents on Private Health Insurance Plans. T his report also addresses states’ roles as the primary regulators of health insurance.
27 See, for example, 42 U.S.C. §§18021, 18023, and 18031; and 45 C.F.R. §§156.200 et seq. Also see the CMS 2021 Letter to Issuers. Network adequacy standards are at 45 C.F.R. §156.200. T he requirement regarding silver and gold plans is discussed in “ Premiums and Cost Sharing” in this report.
Congressional Research Service
6
link to page 39 link to page 39 link to page 9 link to page 18 link to page 18 link to page 28 link to page 28 Overview of Health Insurance Exchanges
Stand-alone dental plans (SADPs) are the only non-QHPs offered in the exchanges. See Table B-
1 for more information.
Under federal law, insurers are not required to offer plans in the exchanges, just as they are not
required to offer plans in markets outside the exchanges. If an insurer does want to offer a plan in an exchange, it must meet applicable federal and state requirements, as discussed in this section and the prior one on “Exchange Administration.” Insurer participation in the individual and
SHOP exchanges is discussed in the sections below.
Individual Exchanges
Individual Exchanges
Eligibility and Enrollment Process
Consumers may purchase health insurance plans for themselves orand their families in their state's individual ’s individual exchange. Consumers may enroll as long as they (1) meet state residency requirements;1028 (2) are not incarcerated, except individuals in custody pending the disposition of charges; and (3) are U.S. citizens, U.S. nationals, or "“lawfully present"” residents.11 29
Undocumented individuals are prohibited from purchasing coverage through the exchanges, even
if they were to pay the entire premium without financial assistance.
Consumers can use their state'’s exchange website (Healthcare.gov or a state-run site) to compare and enroll in plans, and the exchange websites are required to display a calculator that estimates consumers' costs after any cost-sharing reductions or premium tax credits for which they are eligible (see "HealthCare.gov or a state-run site) to apply for
coverage and financial assistance and to compare and enroll in plans. The ACA requires exchanges to provide a “single, streamlined form” that consumers can use to apply for “al applicable State health subsidy programs within the State.”30 This means that through one form, consumers can be determined eligible for exchange financial assistance (see “Premium Tax Credits and Cost-Sharing Reductions"” in this report). Consumers may be linked to, as wel as Medicaid orand the State Children'
Children’s Health Insurance Program (CHIP) enrollment pages if they are eligible.
In addition to using the exchange websites, consumers can , as discussed below.31 The exchange website displays al exchange plans available to a consumer, with estimates of the consumer’s costs, including monthly premiums that reflect the application of any federal financial assistance for
which they are eligible.
In addition to using their exchange website, consumers can apply and enroll by phone, by mail, or in person, in person—including through an agent, broker, or plan issuer—as available by state. Enrollment assistance is available for those who want it (see "Individual and SHOP Exchange Enrollment Assistance" in this report).
Once the exchange receives and verifies consumers' eligibility and enrollment information, it may continue to serve as a conduit through which consumers pay their premiums to their issuers. Alternatively, consumers may pay premiums directly to their issuers.
Enrollment Periods and Enrollment Estimates
Consumers may enroll in coverage through the exchanges only during specified enrollment periods.
Anyone eligible for exchange plan coverage may enroll during an annual open enrollment period (OEP).12 The OEP typically takes place in fall e.g., through exchange Navigators or through agents or brokers; see “Exchange Enrollment
Assistance” in this report).
28 State residency may be established through a variety of means, including actual or planned residence in a state, actual or planned employment in a state, and other circumstances. See 45 C.F.R. §155.305.
29 U.S. citizens and U.S. nationals are eligible for coverage through the exchanges. Lawfully present immigrants are also eligible for coverage through the exchanges. Examples of lawfully present immigrants include those who have qualified non-citizen immigration status without a waiting period, humanitarian statuses or circumstances, valid non -immigrant visas, and legal status conferred by other laws. See 45 C.F.R. §155.305 and HealthCare.gov, “ Coverage for Lawfully Present Immigrants,” at https://www.healthcare.gov/immigrants/lawfully-present-immigrants/. 30 42 U.S.C. §18083, 45 C.F.R. §155.405. 31 Medicaid is a joint federal-state program that finances the delivery of primary and acute medical services, as well as long-term services and supports, to a diverse low-income population, including children, pregnant women, adults, individuals with disabilities, and people aged 65 and older. CHIP is a means-tested program that provides health coverage to targeted low-income children and pregnant women in families that have annual income above Me dicaid eligibility levels but have no health insurance. T he “applicable State health subsidy programs” also include the Basic Health Program, which is operational in two states: Minnesota and New York.
Congressional Research Service
7
link to page 13 Overview of Health Insurance Exchanges
Interaction with Medicaid, CHIP, and Medicare
In conjunction with the streamlined application mentioned above, exchanges must have systems for coordinating with the Medicaid and CHIP programs on eligibility determinations and
enrollment into those programs, for eligible consumers. These systems may vary by state.32
Consumers who are eligible for Medicaid or CHIP may choose to buy exchange coverage instead, but they would not be eligible for financial assistance for exchange coverage (i.e., PTCs or cost-
sharing reduction subsidies).
There are some limitations on the sale of exchange plans to Medicare-eligible or Medicare-enrolled individuals.33 In short, it is general y il egal to sel an individual exchange plan to
someone enrolled in Medicare because it would duplicate coverage.
Open and Special Enrollment Periods
Consumers may enroll in coverage through the exchanges only during specified enrollment
periods.
Anyone eligible for exchange plan coverage may enroll during an annual open enrollment period (OEP).34 The OEP typical y takes place in fal of the year preceding the plan year (PY; the calendar year in the individual exchanges) during which the coverage is effectiveplan year. The OEP for calendar year 2018PY2021 coverage was November 1, 20172020, to December 15, 20172020, for FFE and SBE-FP states. States with SBEs may extend their OEPs, and many do. See Table 1, including table notes, for
details.
Before and during an OEP, consumers already enrolled in coverage through an exchange should receive notification from the exchange and from their insurer about the opportunity to make any
updates to their application data and/or coverage choices. Insurers must notify consumers of changes to their plans such as premiums, benefit coverage, or provider networks (such changes general y cannot be made during a plan year, only in preparation for, and as applicable to, a new
32 45 C.F.R. Part 155, Subpart D, including §155.302. Regarding FFE and SBE-FP states, also see “Medicaid & CHIP Eligibility” in Section 2.1 of CMS, FFE and FF-SHOP Enrollment Manual, June 26, 2018, at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/General-Resources-Items/FFM-and-FF-SHOP-Enrollment -Manual. Information for consumers is at Medicare.gov, “ Medicare & the Marketplace,” at https://www.medicare.gov/about -us/medicare-the-marketplace. Hereinafter referred to as CMS, FFE and FF-SHOP Enrollm ent Manual. Regarding SBE states, also see Sara Rosenbaum et al., Stream lining Medicaid Enrollm ent: The Role of the Health Insurance Marketplaces and the Im pact of State Policies, Commonwealth Fund, March 30, 2016, at https://www.commonwealthfund.org/publications/issue-briefs/2016/mar/streamlining-medicaid-enrollment -role-health-insurance. 33 Medicare is a federal health insurance program that pays for covered health care services for most people aged 65 and older and for certain permanently disabled individuals under the age of 65. T he prohibition on selling an individual exchange plan to someone enrolled in Medicare does not apply to employment -based coverage, including coverage sold in the SHOP exchanges. See CMS, “ Medicare and the Marketplace,” updated December 2019, at https://www.cms.gov/Medicare/Eligibility-and-Enrollment/Medicare-and-the-Marketplace/Overview1.html. Also see Section 2.6.8 of CMS, FFE and FF-SHOP Enrollm ent Manual, June 26, 2018, at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/General-Resources-Items/FFM-and-FF-SHOP-Enrollment -Manual. Information for consumers is at Medicare.gov, “ Medicare & the Marketplace,” at https://www.medicare.gov/about-us/medicare-the-marketplace. CMS, FFE and FF-SHOP Enrollm ent Manual.
34 45 C.F.R. §155.410.
Congressional Research Service
8
link to page 7 link to page 12 Overview of Health Insurance Exchanges
plan year).35 If an existing exchange plan enrollee does not take any action during the OEP, they
general y wil be automatical y reenrolled in the same plan for the upcoming plan year.36
Table 1. Open Enrollment Periods for Individual Exchanges on the Federal Platform,
by Plan Year
Plan Year
2014
2015
2016
2017
2018
2019
2020
2021
Oct. 1,
Nov. 15,
Nov. 1,
Nov. 1,
Nov. 1,
Nov. 1,
Nov. 1,
Nov. 1,
HealthCare.
2013-
2014-
2015-
2016-
2017-
2018-
2019-
2020-
gov OEP
Mar. 31,
Feb. 15,
Jan. 31,
Jan. 31,
Dec. 15,
Dec. 15,
Dec. 15,
Dec. 15,
2014
2015
2016
2017
2017
2018
2019
2020
Source: CRS analysis of Department of Health and Human Services (HHS) reports on enrol ment during annual open enrol ment periods. See the “Pre-effectuated Enrol ment Data” section of CRS Report R46638, Health Insurance Exchanges: Sources for Statistics for reports by year.
Notes: FFE = federal y facilitated exchange; OEP = open enrol ment period; PY = plan year; SBE = state-based exchange; SBE-FP = state-based exchange using the federal information technology platform; SEP = special enrol ment period. See “State-Based and Federal y Facilitated Exchanges” in this report for more information. The HealthCare.gov OEP applies to FFE and SBE-FP states. In some years, there also have been federal OEP extensions or SEPs for broadly applicable situations, such as in the 2018 OEP, due to natural disasters in 2017. See “Open and Special Enrol ment Periods” in this report for more information. The OEPs of SBEs may be longer in a given year. For PY2020, 9 of 13 SBEs extended their OEPs. See CMS, “2020 Marketplace Open Enrol ment Period Public Use Files” at https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Marketplace-Products/2020-Marketplace-Open-Enrol ment-Period-Public-Use-Files.
Consumers also may be al owed, for FFE and SBE-FP states (see Table 1 for enrollment periods). States with SBEs may observe different OEPs. For 2018 coverage, all 12 SBEs' OEPs lasted longer than the federal OEP.13 The OEP for plan year 2019 is currently set as November 1, 2018, to December 15, 2018, for FFE and SBE-FP states.
Consumers also may be allowed to enroll for coverage in an exchange if they qualify for a special enrollment periodspecial enrollment period (SEP). General y (SEP).14 Generally, consumers qualify for SEPs due to a change in personal circumstances—for example, a change in marital status or number of dependents—or loss of qualifying coverage.15 37 HHS also may choose to offer SEPs or extend an OEP for some or all consumers due to broadly applicable circumstances.16 In addition, consumers generally may enroll in Medicaid or CHIP whenever they qualify, regardless of their state's exchange OEP.
Annual individual exchange enrollment estimates to date are shown in Table 1. Given the exchange eligibility determination process as well as the OEPs and SEPs, data on exchange enrollment are releasedal
35 See Section 2.6 of CMS, FFE and FF-SHOP Enrollment Manual; the “Reenrollment Communications to Enrollees” section cites CMS guidance: Updated Federal Standard Renewal and Product Discontinuation Notices, September 2016, at https://www.cms.gov/CCIIO/Resources/Regulations-and-Guidance/Downloads/Final-Updated-Federal-Standard-Renewal-and-Product -Discontinuation-Notices-090216.pdf. T here, see “ Instructions for Attachment 2.” 36 For more information about plan renewal options and processes, including automatic renewals of enrollees in their existing plans or in alternate plans if their existing ones will no longer be available, see Section 2.6 of CMS, FFE and FF-SHOP Enrollm ent Manual. Although this manual describes processes for HealthCare.gov states, SBEs also have processes for automatic reenrollment.
37 Qualifying coverage generally means the types of minimum essential coverage (MEC) that are identified in the Internal Revenue Code (IRC) Section 5000A and its implementing regulations. Most types of comprehensive coverage are considered MEC, including public coverage (e.g., Medicaid, Medicare), as well as private insurance (e.g., employer-sponsored insurance and non-group insurance). For other types of coverage losses that can trigger an exchange special enrollment period (SEP), see 45 C.F.R. §155.420. Also see 45 C.F.R. §147.104 regarding SEPs applicable to the individual and group markets overall.
Congressional Research Service
9
Overview of Health Insurance Exchanges
consumers due to broadly applicable circumstances.38 Subject to statutory requirements, HHS
may make changes to SEPs.39
Federal SEPs apply to FFEs, SBE-FPs and general y to SBEs, but SBEs have flexibility regarding
implementation of some SEPs. SBEs also may create their own SEPs, subject to applicable federal and state laws. Federal SEPs for the individual exchanges may or may not apply to the
federal SHOP exchanges and/or to the individual market outside the exchanges.40
Eligibility for Medicaid or CHIP may be determined at any point during the calendar year and has
no connection to an applicant’s state’s exchange OEP.
Special Enrollment Periods and COVID-19
During the Coronavirus Disease 2019 (COVID-19) pandemic and related economic recession,
there have been questions about SEPs to al ow consumers to enroll in coverage via the exchanges.
In response to COVID-19, most SBEs created SEPs to al ow individuals to purchase coverage. These SEPs general y were open in spring 2020, with varied timing and durations. Some were
extended one or more times. In general, these SEPs were available to any uninsured individuals
eligible for exchange coverage.41
In 2020, HHS did not announce a COVID-related federal SEP for al uninsured individuals to
enroll in coverage in FFEs and SBE-FPs. However, an existing SEP al ows individuals to enroll if they lose their job-based coverage or other qualifying coverage. A June 2020 Centers for Medicare & Medicaid Services (CMS) report on exchange enrollment during the pandemic further stated that “any consumers who qualified for a SEP but missed the deadline as a result of the COVID-19 pandemic—for example, if they were sick with COVID-19 or were caring for
someone who was sick with COVID-19—may also be eligible for another SEP.”42 This is similar to federal SEPs announced in relation to prior disasters. In addition, at least as of the second half of 2020, the federal exchange website HealthCare.gov indicated that losing qualifying coverage since the start of 2020 could qualify someone for an SEP, as opposed to the standard eligibility
criterion of losing qualifying coverage in the prior 60 days.43
38 For example, in 2014, the Department of Health and Human Services (HHS) established an SEP due to technical problems submitting insurance applications through the federal information technology platform (i.e., HealthCare.gov). In 2015, HHS established an SEP around tax season for individuals who had not enrolled in 2015 coverage and were subject to the 2014 individual mandate penalty. For 2018 coverage, HHS established an SEP for consumers in states that were affected by the 2017 hurricanes or other severe weather events. See, for example, HHS, HealthCare.gov, “Special Enrollment Periods for Complex Issues,” at https://www.healthcare.gov/sep-list/. 39 Statutory requirements for exchange SEPs are at 42 U.S.C. §18031(c)(6). Multiple examples and discussion of administrative changes made to SEPs are in the HHS final rule, “ Patient Protection and Affordable Care Act; Market Stabilization,” 82 Federal Register 18346, April 18, 2017, at https://www.federalregister.gov/documents/2017/04/18/2017-07712/patient-protection-and-affordable-care-act-market-stabilization. T he background of this rule also provides information on prior administrative actions related to SEPs.
40 For more information about SEPs, see Section 5 of CMS, FFE and FF-SHOP Enrollment Manual. 41 T he National Association of Insurance Commissioners (NAIC) has been tracking various state-level actions related to COVID-19 and insurance, including SEPs announced by SBEs. See NAIC, “ Coronavirus Resource Center,” “ Life and Health” spreadsheet, at https://content.naic.org/naic_coronavirus_info.htm. 42 CMS, Special Trends Report: Enrollment Data and Coverage Options for Consumers During the COVID-19 Public Health Em ergency, June 2020, at https://www.cms.gov/CCIIO/Resources/Forms-Reports-and-Other-Resources/Downloads/SEP-Report -June-2020.pdf.
43 HealthCare.gov page on special enrollment periods, at https://www.healthcare.gov/coverage-outside-open-enrollment/special-enrollment -period/.
Congressional Research Service
10
link to page 16 Overview of Health Insurance Exchanges
On January 28, 2021, HHS (via CMS) announced a new COVID-19-related SEP, in effect February 15-May 15, 2021, to al ow al exchange-eligible consumers to newly enroll or update their enrollment in an exchange plan.44 Per the announcement, CMS also wil conduct a consumer outreach campaign to promote the SEP. This SEP is available in al states using the HealthCare.gov enrollment platform (FFEs and SBE-FPs); states with SBEs are “strongly
encouraged” by CMS to take similar action.
For information about other coverage options following loss of job-based coverage, see CRS In
Focus IF11523, Health Insurance Options Following Loss of Employment.
Enrollment Estimates
Annual individual exchange enrollment estimates to date are shown in Table 2. Given the exchange eligibility determination process, as wel as the different time frames of OEPs and SEPs, CMS releases data on exchange enrollment in stages. Pre-effectuated enrollment is the number of unique individuals who have been determined eligible to enroll in an exchange plan
and have selected a plan. These individuals may or may not have submitted the first premium payment. In general, cumulative and final pre-effectuated enrollment estimates are released
during and soon after an annual open enrollment period.
Subsequently, effectuated enrollment is the number of unique individuals who have been determined eligible to enroll in an exchange plan, have selected a plan, and have submitted the first premium payment for an exchange plan. Effectuated enrollment estimates generallygeneral y are point-in-time and may change over the coverage year. For example, due to changes in life circumstances, an individual may disenroll (e.g., if later offered coverage through an employer) ,
or enroll (e.g., given eligibility for an SEP) in an exchange plan.
|
PY2014 |
PY2015 |
PY2016 |
PY2017 |
PY2018 |
|
|
Oct. 1, 2013-Mar. 31, 2014 |
Nov. 15, 2014-Feb. 15, 2015 |
Nov. 1, 2015-Jan. 31, 2016 |
Nov. 1, 2016-Jan. 31, 2017 |
Nov. 1, 2017-Dec. 15, 2017 |
|
8.0 million |
11.7 million |
12.7 million |
12.2 million |
|
|
6.3 million as of Dec. 2014 |
|
|
|
Not released as of this report |
Source: CRS analysis based on Department of Health and Human Services (HHS) annual reports of individual exchange enrollment in private health insurance plans. Some of these reports are available at HHS, Assistant Secretary for Planning and Evaluation (ASPE), "Historical Research," at https://aspe.hhs.gov/historical-research. Some are available at CMS, Center for Consumer Information and Insurance Oversight (CCIIO), "Data Resources," at https://www.cms.gov/CCIIO/ Resources/Data-Resources/index.html; others are available elsewhere on the CMS site. The 2018 pre-effectuated estimates are available at CMS, "Health Insurance Exchanges 2018 Open Enrollment Period Final Report," April 3, 2018, at https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2018-Fact-sheets-items/2018-04-03.html. Contact report author for all sources.
Notes: PY = plan year; OEP = open enrollment period; SEP = special enrollment period. FFE = federally facilitated exchange; SBE = state-based exchange; SBE-FP = state-based exchange using the federal information technology platform. See "State-Based and Federally Facilitated Exchanges" in this report for more information.
a. The Healthcare.gov OEP applies to FFE and SBE-FP states. The OEPs of SBEs may be longer in a given year. In some years, there also have been federal OEP extensions or SEPs for broadly applicable situations, such as in the 2018 OEP, due to natural disasters in 2017. See "Enrollment Periods" and footnote 16 in this report.
b. Pre-effectuated enrollment is the number of unique individuals who have been determined eligible to enroll in an exchange plan and have selected a plan but may or may not have submitted the first premium payment. Final pre-effectuated enrollment estimates are typically released following an OEP and include any broadly applicable OEP extensions or longer SBE OEPs. See "Enrollment Periods" in this report for more information.
c. Effectuated enrollment is the number of unique individuals who have been determined eligible to enroll in an exchange plan, have selected a plan, and have submitted the first premium payment for an exchange plan. HHS may release effectuated enrollment estimates for different points in time over a plan year. See "Enrollment Periods" in this report for more information.
d. CMS initially (in June 2016) reported 11.1 million effectuated enrollment as of March 2016. In June 2017, CMS updated this number to 10.8 million as of March 2016 and 9.1 million as of December 2016.
e. As of the date this report was published, these are the latest effectuated data released for 2017.
, outside of an OEP.
CMS also releases average effectuated enrollment estimates over specified time periods (e.g., over the first half of an enrollment year or monthly for the previous enrollment year). See the
“Enrollment Statistics” section of CRS Report R46638, Health Insurance Exchanges: Sources for
Statistics, for HHS reports and resources detailing different enrollment estimates by year.
44 CMS, “ 2021 Special Enrollment Period in response to the COVID-19 Emergency,” January 28, 2021, at https://www.cms.gov/newsroom/fact-sheets/2021-special-enrollment -period-response-covid-19-emergency.
Congressional Research Service
11
link to page 16 link to page 16 link to page 16 link to page 12 link to page 12 link to page 7 Overview of Health Insurance Exchanges
Table 2. Nationwide Individual Exchange Enrollment Estimates, by Plan Year
Plan Year
Nationwide
Enrollment
Estimate
Type
2014
2015
2016
2017
2018
2019
2020
2021
Pre-
Data
effectuateda
expected
final for PY
8.0M
11.7M
12.7M
12.2M
11.8M
11.4M
11.4M
spring
OEP
2021
Effectuated,
Early
early in the
2014
Data
plan year
10.2M,
11.1M,
10.3M,
10.6M,
10.6M,
10.7M,
expected
(point-in-time
estimate
Mar.
Mar.
Feb.
Feb.
Feb.
Feb.
summer
as of date
not
2015
2016
2017
2018
2019
2020
2021
shown)b
found
Effectuated, late in the plan
Data
Data
year (point-in-
6.3M,
8.8M,
9.1M,
8.9M,
9.2M,
9.1M,
expected
expected
time or
Dec.
Dec.
Dec.
Dec.
Dec.
Dec.
summer
summer
average for
2014
2015
2016
2017
2018
2019
2021
2022
month shown)c
Source: CRS analysis based on Department of Health and Human Services (HHS) reports of individual exchange enrol ment. Data sources are in CRS Report R46638, Health Insurance Exchanges: Sources for Statistics, in report sections specified in table notes below. Notes: FFE = federal y facilitated exchange; OEP = open enrol ment period; PY = plan year; SBE = state-based exchange; SBE-FP = state-based exchange using the federal information technology platform. See “Open and Special Enrol ment Periods” and “State-Based and Federal y Facilitated Exchanges” in this report. a. Pre-effectuated enrol ment is the number of unique individuals who have been determined eligible to enrol in
an exchange plan and have selected a plan but may or may not have submitted the first premium payment. Final pre-effectuated enrol ment estimates typical y are released fol owing an OEP and include any broadly applicable OEP extensions or longer SBE OEPs. For these data sources by year, see the “Pre-effectuated Enrol ment Data” section of the report mentioned above.
b. Effectuated enrol ment is the number of unique individuals who have been determined eligible to enrol in an
exchange plan, have selected a plan, and have submitted the first premium payment for an exchange plan. HHS general y releases effectuated enrol ment estimates for a point i time early in the plan year and may release additional point-in-time estimates during the year. Data sources by year are in the “Point-in-Time Effectuated Enrol ment Data” section of the report mentioned above. For example, the 2020 data is from CMS, Early 2020 Effectuated Enrol ment Snapshot, July 2020.
c. See table note (b) regarding effectuated enrol ment and point-in-time estimates. Average estimates reflect
an average over a specified time period, in this case one month. For PY2014 and PY2015, quarterly point-in-time estimates were released, including those shown. Average monthly enrol ment data were not provided for those years. For PYs 2016 and on, average monthly enrol ment data are provided. Although point-in-time and average monthly estimates are not the same, they are provided here to show late-year enrol ment estimates across al plan years. Data sources by year are in the “Point-in-Time Effectuated Enrol ment Data” and “Average Monthly Effectuated Enrolment Data” sections of the report mentioned above. For example, the 2018 data is from the end of the report CMS, Early 2019 Effectuated Enrol ment Snapshot, August 2019.
Premiums and Cost Sharing Typical y, enrollees of private health insurance plans (in or out of the exchanges) pay monthly premiums. They also are general y responsible for out-of-pocket (OOP) costs, or cost sharing, as
Congressional Research Service
12
link to page 9 link to page 18 Overview of Health Insurance Exchanges
they use services. In general, cost sharing includes deductibles, coinsurance, and co-payments, up
to an annual maximum amount of OOP spending.45
Premiums are set by health insurance issuers and are based on their expected medical claims costs
(i.e., the payments they expect to make for covered health benefits for a given group of enrollees, or a given risk pool), administrative expenses, taxes, fees, and profit. The premium-setting process is subject to federal and state requirements, as applicable to plans both in and out of the exchanges. For example, insurers cannot vary premiums based on health status.46 In addition, insurers that want to offer plans in the exchanges must submit their proposed premiums for
federal or state approval (depending on exchange type) each year.47 If consumers do not pay their premiums, insurers may terminate their coverage, subject to applicable federal and state
requirements.48
In addition to setting premiums, insurers set cost-sharing levels, or the share of the costs of covered benefits (or medical claims) for which the insurer and enrollee wil be responsible. Most health plans sold through the exchanges (and non-grandfathered plans sold in the individual and smal -group markets off-exchange49) are subject to minimum actuarial value (AV) standards and accordingly, are given a precious metal designation (platinum, gold, silver, or bronze).50 AV is a
summary measure of a plan’s generosity in terms of cost sharing, estimated for a standard population.51 Actuarial values by metal level are platinum (AV of 90%), gold (80%), silver (70%), and bronze (60%). For example, for a silver plan, the insurer expects to cover approximately 70% of cost sharing for the plan’s enrollees overal . The higher the AV percentage, the lower the cost sharing, on average, for the plan population. However, plans with higher AV also may have higher premiums, on average, to cover their increased share of their enrollees’ medical claims
costs (assuming other factors affecting premiums remain the same, such as administrative expenses). The AV standards, and the related metal levels, are meant, in part, to help consumers in
comparing the value of plans.
45 A deductible is the amount an insured consumer pays for covered health care services before coverage begins (with exceptions). Coinsurance is the share of costs, figured in percentage form, an insured consumer pays for a covered health service. A co-paym ent is the fixed dollar amount an insured consumer pays for a covered health service. Once an insured consumer’s out-of-pocket spending has met an out-of-pocket limit or maximum in a plan year, the insurer will generally pay 100% of covered costs for the remainder of the plan year.
46 See CRS Report R45146, Federal Requirements on Private Health Insurance Plans, for more information about this and other requirements related to setting premiums.
47 See “Exchange Administration” in this report. 48 See 45 C.F.R. §156.270 regarding insurer termination of enrollee coverage, including for nonpayment of premiums. It also addresses the “grace period” of three consecutive months of premium nonpayment for enrollees who receive a premium tax credit (discussed in the “ Premium T ax Credits and Cost -Sharing Reductions” section of this report ).
49 Grandfathered plans are individual or group plans in which at least one individual was enrolled as of enactm ent of the ACA (March 23, 2010) and which continue to meet certain criteria. Plans that maintain their grandfathered status are exempt from some, but not all, federal requirements. T here are no grandfathered plans sold through the exchanges, but they may be available off the exchanges. For more information, see CRS Report R46003, Applicability of Federal Requirem ents to Selected Health Coverage Arrangem ents, as well as HHS, “ Grandfathered Health Insurance P lans,” at https://www.healthcare.gov/health-care-law-protections/grandfathered-plans/. 50 42 U.S.C. §18022(d). 51 Actuarial value (AV) is expressed as the percentage of medical expenses estimated to be paid by the insurer for a standard population and set of allowed charges. It is not a measure of plan generosity for an enroll ed individual or family, nor is it a measure of premiums or benefits packages. AV calculations are required to apply only to the plan’s covered essential health benefits (EHB) that are furnished by an in-network provider, unless otherwise addressed in federal or state law.
Congressional Research Service
13
link to page 39 link to page 18 link to page 20 link to page 44 link to page 16 Overview of Health Insurance Exchanges
With the exception of “catastrophic” plans and stand-alone dental plans (see Table B-1), plans must have at least 60% AV to be sold in the exchanges. Insurers sel ing a given plan in an exchange must offer at least a silver and gold version of the plan throughout each service area in
which the insurers offer coverage.52
Annual OOP limits also apply to al health plans sold in the exchanges (and to al non-grandfathered individual and group plans sold outside the exchanges).53 These limits are updated each year through HHS rulemaking (see Table 3). Plans may set their OOP limits lower than
these maximums. Additional data on premiums and cost sharing are in Table 4 at the end of the following section.
Table 3. Annual Out-of-Pocket Limits, by Plan Year
(federal y set maximums; insurers may set lower out-of-pocket limits)
Plan Year
2014
2015
2016
2017
2018
2019
2020
2021
Self-only coverage
$6,350
$6,600
$6,850
$7,150
$7,350
$7,900
$8,150
$8,550
Coverage other
$12,700
$13,200
$13,700
$14,300
$14,700
$15,800
$16,300
$17,100
than self-only
Percentage increase
N/A
4%
4%
4%
3%
7%
3%
5%
over prior year
Source: CRS analysis of relevant federal rulemaking. These amounts are updated each year through an HHS rule cal ed the Notice of Benefit and Payment Parameters, also known as the Payment Notice. For example, the PY2021 rates were finalized in the 2021 Payment Notice, p. 7127. Although a final 2022 Payment Notice was published in January 2021, it did not include these amounts for PY2022. Annual Payment Notices are cited in Table D-1. Notes: PY = plan year. Out-of-pocket (OOP) limits are related to an insured consumer’s cost sharing, or OOP spending (including deductibles, coinsurance, and co-payments; see “Premiums and Cost Sharing” in this report for more information). Once this OOP spending meets the plan’s OOP limit or maximum in a plan year, the insurer general y wil pay 100% of covered costs for the remainder of the plan year. An individual enrol ed in a plan by themselves has self-only coverage. An individual enrol ed in a plan with a spouse and/or dependents has coverage other than self-only, or family coverage.
Premium Tax Credits and Cost-Sharing Reductions
Premium Tax Credits and Cost-Sharing Reductions
Consumers purchasing coverage through the individual exchanges may be eligible to receive
financial assistance that effectively reduces their cost of that coverage. Eligibility for such assistance is based primarily on income and provided in the form of premium tax credits (PTCs)
and cost-sharing reductions.17
The premium tax credit is generally available to consumers (CSRs).54
The PTC general y is available to consumers with household incomes between 100% and 400% of the federal poverty level (FPL), with some exceptions, and who do not have access to public coverage (e.g., Medicaid) or employment-based coverage that meets certain standards.18 The credit is designed to reduce an eligible individual' individual’s cost of purchasing health insurance coverage
52 45 C.F.R. §156.200(c)(1). 53 Like AV calculations, the annual out -of-pocket limit is only required to apply to the plan’s covered EHB that are furnished by an in-network provider, unless otherwise addressed in federal or state law.
54 For more information about these forms of consumer financial assistance, including applicable eligibility criteria and illustrative examples, see CRS Report R44425, Health Insurance Prem ium Tax Credits and Cost-Sharing Subsidies.
Congressional Research Service
14
link to page 20 link to page 20 Overview of Health Insurance Exchanges
s cost of purchasing health insurance coverage through the exchange. The amount of the premium tax creditPTC is based on a statutory formula and varies from person to person. It is designed to provide larger credit amounts to individuals with lower incomes compared to those with higher incomes.
The premium credit is refundable, so individuals may claim the full credit amount when filing their taxes, even if they have little or no federal income tax liability. The credit also is advanceable, so instead of waiting until they file taxes, individuals may choose to receive the credit on a monthly basisAlthough the amount of the PTC is based on the second-lowest-cost silver plan in a consumer’s local area, consumers may apply the credit to any
bronze- or higher-metal level plan available to them on their state’s exchange.
Individuals who receive PTCs also may be eligible for subsidies that reduce cost-sharing expenses.55 These cost-sharing subsidies (also cal ed CSRs) are applied in two ways. First, an insurer must reduce the annual OOP limit that otherwise would apply to an eligible individual’s
exchange plan. Second, the insurer must effectively raise the actuarial value of the eligible individual’s plan, for example by reducing other cost-sharing requirements beyond the lowered OOP cap. Among other eligibility requirements, CSRs general y are available to consumers who are eligible for PTCs and have incomes between 100% and 250% of the FPL. Although a PTC
can be applied to any metal level plan, CSRs are applicable only to silver plans.
Table 4 summarizes nationwide data on premiums, advance premium tax credit (APTC) 56, and CSRs by year, as available in relevant HHS reports on effectuated enrollment.57 The average premium and APTC amounts shown in the table may obscure wide variations in actual amounts
per consumer, depending on the plan and metal level an individual chooses and/or the factors by which an insurer is able to vary premiums, discussed below.58 Premium and cost-sharing data on al plans offered in the exchanges, as opposed to such data for plans selected, also are available,
including for PY2021.59
55 T he ACA requires the HHS Secretary to provide full reimbursements to insurers that provide these cost -sharing subsidies to their enrollees. However, the ACA did not appropriate funds for such payments. In October 2017, the T rump Administration halt ed these payments, effective immediately, until Congress appropriates funds. I nsurers still must provide the subsidies to eligible consumers, but insurers are not reimbursed. See HHS, “ Payments to Issuers for Cost-Sharing Reductions,” October 12, 2017, at https://www.hhs.gov/sites/default/files/csr-payment -memo.pdf. 56 Consumers may choose to receive the credit on a monthly basis, in advance of filing taxes, to coincide with the payment of insurance premiums (technically, these advance payments go directly to issuersinsurers). Advance payments automatically reduce monthly premiums by the credit amount. T his option is called the advance premium tax credit, or APT C. Consumers may instead claim the full credit amount of the PT C when filing their taxes, even if they have little or no federal income tax liability.
57 In the reports cited in Table 4, certain of these data are also available at the state level. In these HHS reports, and in other HHS reports (e.g., on pre-effectuated enrollment) some data may also be available on demographics and/or metal levels of plans. For more information, see CRS Report R46638, Health Insurance Exchanges: Sources for Statistics. 58 In addition, the APT C data in the table are not necessarily final, because when an individual receiving an APT C files his or her tax return for a given year, the total amount of advance payments he or she received in that tax year is reconciled with the amount he or she should have received based on the individual’s actual income over the course of the tax year.
59 For example, an October 2020 CMS report discusses premiums and cost sharing on plans that will be available in HealthCare.gov exchanges (FFEs and SBE-FPs) in PY2021: CMS, CCIIO, Plan Year 2021 Qualified Health Plan Choice and Prem ium s in HealthCare.gov States, October 2020, at https://www.cms.gov/CCIIO/Resources/Data-Resources/QHP-Choice-Premiums. Also see KFF, Average Marketplace Premiums by Metal T ier, 2018-2021, at https://www.kff.org/health-reform/state-indicator/average-marketplace-premiums-by-metal-tier/; and KFF, Cost -Sharing for Plans Offered in the Federal Marketplace, 2014 -2021, at https://www.kff.org/slideshow/cost -sharing-for-plans-offered-in-the-federal-marketplace/.
Congressional Research Service
15
link to page 20 link to page 20 link to page 20 link to page 20 link to page 20 link to page 20 link to page 20 link to page 20 link to page 21 link to page 21 link to page 21 link to page 16 Overview of Health Insurance Exchanges
Table 4. Data on Premiums, Advance Premium Tax Credits, and Cost-Sharing
Reductions Nationwide, by Plan Year
(data based on ef ectuated enrol ment in al individual exchanges)
Plan Year
2014a
2015b
2016b
2017c
2018d
2019e
2020f
Average total
N/A
N/A
N/A
$470.52
$597.20
$594.17
$576.16
premium per monthg
Average APTC
$276
$272
$291
$373.06
$519.89
$514.01
$491.53
per monthh
Percentage of
86%
85%
85%
84%
87%
87%
86%
enrol ees receiving APTCi
Percentage of
58%
57%
57%
57%
53%
52%
50%
enrol ees receiving CSRj
Data as of
Dec. 2014
Mar. 2015
Mar. 2016
PY2017
Feb. 2018
Feb. 2019
Feb. 2020
Sources: CRS analysis based on specified Department of Health and Human Services (HHS) reports of individual exchange enrol ment in private health insurance plans. Titles and publication dates of sources by year are listed below. These sources are ful y cited in CRS Report R46638, Health Insurance Exchanges: Sources for Statistics, in the “Point-in-Time Effectuated Enrol ment Data” section of the report. Notes: APTC = Advance premium tax credit; CSR = Cost-sharing reduction; PY = Plan year. These are types of financial assistance that effectively reduce premiums and cost sharing, respectively, for eligible consumers obtaining coverage in the individual exchanges. The average premium and APTC amounts shown above may obscure wide variations in actual amounts per consumer, depending on the metal level plan an individual chooses and/or the factors by which an insurer is able to vary premiums (see “Premiums and Cost Sharing” in this report). In addition, the APTC data in the table are not necessarily final, because when an individual receiving an APTC files his or her tax return for a given year, the total amount of advance payments he or she received in that tax year is reconciled with the amount he or she should have received. a. Relevant data for PY2014 are available only as of December 2014. These numbers are provided to al ow for
approximate comparison within the table. Average premium amounts were not provided in this or the fol owing year’s report. See March 31, 2015 Effectuated Enrol ment Snapshot, June 2015.
b. Average premium amounts for PY2015 and PY2016 were not provided in those years’ or the fol owing
years’ reports. See March 31, 2015 Effectuated Enrol ment Snapshot, June 2015 and March 31, 2016 Effectuated Enrol ment Snapshot, June 2016, respectively.
c. The June 2017 report provided average APTC data but not average premium data for February 2017.
However, the July 2018 report provided average monthly premium and APTC data for the 2017 plan year (total amounts for the year, divided by the total number of member months). The data in this column, from the July 2018 report, are provided to al ow for approximate comparison, but they are average monthly estimates for the year rather than the average estimates for a given month as shown in this table for other years. See 2017 Effectuated Enrol ment Snapshot, June 2017 and Early 2018 Effectuated Enrol ment Snapshot, July 2018.
d. See Early 2018 Effectuated Enrol ment Snapshot, July 2018. e. See Early 2019 Effectuated Enrol ment Snapshot, August 2019. f.
See Early 2020 Effectuated Enrol ment Snapshot, July 2020.
g. This definition, or a non-substantive variation of it, appears in one or more reports: “Average total premium
per month is the total premium (including APTC and any premium paid by the policyholder) for the mon th, divided by the number of individuals who had an active policy for the month.”
Congressional Research Service
16
link to page 10 link to page 21
Overview of Health Insurance Exchanges
h. This definition, or a non-substantive variation of it, appears in one or more reports: “Average APTC per
month is the total amount of APTC for the month for al individuals who received APTC, divided by the number of individuals who received APTC.”
i.
This definition, or a non-substantive variation of it, appears in one or more reports: “APTC enrol ment is the total number of individuals who had an active policy in February 2017 , who paid their premium (thus becoming effectuated), and who received an APTC subsidy.”
j.
This definition, or a non-substantive variation of it, appears in one or more reports: “CSR enrol ment is the total number of individuals who had an active policy in February 2017, who paid their premium (thus effectuating their coverage), and received CSRs.”
Insurer Participation As stated earlier (see “Qualified Health Plans”), insurers are not required to participate in the
exchanges, but they must meet certain requirements if they do want to offer plans in an exchange.
For each plan year to date, at least one insurer has offered an individual exchange plan in each
county in al states. See Figure 2 for projected insurer participation in PY2021.60 However, there have been concerns about “bare counties” in one or more plan years, particularly as insurers were
making their decisions in 2017 about offering coverage for PY2018.61
Figure 2. Plan Year 2021 Insurer Participation in the Individual Exchanges, by County
(CMS map of projected participation as of October 2, 2020)
Source: CMS, CCIIO, “County by County Plan Year 2021 Projected Insurer Participation in Health Insurance Exchanges,” published October 16, 2020 at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/Health-Insurance-Exchange-Coverage-Maps. This page also has insurer participation maps for PYs 2018 to 2020. Notes: CCIIO = Center for Consumer Information and Insurance Oversight; CMS = Centers for Medicare & Medicaid Services; PY = plan year. CMS notes on map: “Values may not add to 100% due to rounding. Federal y-Facilitated Exchange (FFE) data
60 In addition, insurer participation maps for PYs 2018 to 2020 are at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/Health-Insurance-Exchange-Coverage-Maps.html. A Kaiser Family Foundation analysis of insurer participation from 2014 to 2020 is discussed later in this section. 61 See, for example, T eichert, Erica, “Last ‘bare’ county in the U.S. scores ACA exchange coverage,” Modern Healthcare, August 24, 2017, at https://www.modernhealthcare.com/article/20170824/NEWS/170829941/last-bare-county-in-the-u-s-scores-aca-exchange-coverage.
Congressional Research Service
17
link to page 18 link to page 33 Overview of Health Insurance Exchanges
reflected on this map are point in time as of 10/02/2020. State-Based Exchange (SBE) data are preliminary and self-reported from the Exchanges to CMS. These data are point in time as of 10/09/2020 for CO, CT, DC, ID, MA, MD, MN, NV, RI, VT, and WA, and 08/30/2020 for NJ and PA. County-level information for the fol owing SBE states (CA and NY) is representative of PY2020 participation as PY2021 participation has not yet been provided by the Exchanges to CMS.”
An insurer might choose to begin, continue, or stop offering coverage in a state or locality, on and/or off an exchange, for various reasons. Fundamental y, insurers make decisions based on their assessment of their risk, or likelihood and potential magnitude of loss. Individuals differ in their health insurance risk based on their health status, with sicker individuals considered high
risk and expected to have greater health care costs than healthier individuals (i.e., low -risk individuals). Other factors that may affect insurers’ risk assessments and decisionmaking regarding market participation include federal and state policies, provider and insurer market competition, and consumer behavior, as wel as the potential for uncertainty regarding any of
these factors (e.g., the potential for unexpected federal or state policy changes affecting insurers).
In January 2019, the Government Accountability Office (GAO) released a report on insurer participation and related issues in the individual exchanges.62 The report provided background on a range of potential contributing factors, including the federal requirements imposed by the ACA
on plans sold in the individual market, including the exchanges63; the consumer financial assistance available only in the exchanges64; the three ACA programs—risk corridors, reinsurance, and risk adjustment—meant to mitigate insurers’ financial risk in the individual and smal -group markets, including in the exchanges65; federal policy changes in the years since the enactment of the ACA66; and state-level requirements. These and other factors, such as the health of the populations enrolling in exchange plans, had varying impacts on claims costs (the costs
insurers pay for their enrollees’ health benefits), which in turn impacted insurer participation, as wel as insurers’ decisions about premium amounts and plan designs (e.g., covered benefits, cost
sharing, and provider networks).
Insurer participation general y increased in PY2021 over PY2020. According to an October 2020
CMS report (on FFE and SBE-FP states only),
62 Government Accountability Office (GAO), Health Insurance Exchanges: Claims Costs and Federal and State Policies Drove Issuer Participation, Prem ium s, and Plan Design, January 2019, at https://www.gao.gov/products/GAO-19-215. 63 Several provisions of the ACA, such as guaranteed issue of health insurance, generally have increased higher -risk individuals’ ability to purchase insurance and restricted insurers’ ability to deny or limit coverage to such individuals. T he ACA created some new requirements and expanded some existing requirements, including by applying requirements on the individual market that previously existed in one or more segments of the group market. See the appendix of CRS Report R45146, Federal Requirem ents on Private Health Insurance Plans.
64 See “Premium T ax Credits and Cost -Sharing Reductions” in this report. One of the factors cited in the GAO report as affecting insurers’ participation was “federal funding changes,” including the ending of federal payments for cost -sharing reduction subsidies in October 2017. 65 Of the three ACA risk-mitigation programs—risk corridors, reinsurance, and risk adjustment —one was designed to be permanent. T he risk corridors and reinsurance programs were in effect from 2014 to 2016; the risk adjustment program also began in 2014 and is still in effect. It assesses charges on applicable private health insurance plans with relatively healthier enrollees and uses collected charges to make payments to private health plans in the same state that have relatively sicker enrollees. See “ Other Federal Funding Sources” in this report regarding the charges assessed on insurers via the risk adjustment program. T he phaseouts of the other two programs are cited among “ federal funding changes” affecting insurers’ participation decisions. For descriptions of all three programs and their different approaches, see T able 1 in CRS Report R45334, The Patient Protection and Affordable Care Act’s (ACA’s) Risk Adjustm ent Program : Frequently Asked Questions.
66 See Figure 1 in the GAO report discussed in this section.
Congressional Research Service
18
link to page 35 Overview of Health Insurance Exchanges
Out of the 36 PY21 HealthCare.gov states, 16 states have more QHP issuers participating in PY21 than PY20, and 27 states have counties with more QHP issuers in PY21 than PY20 due to new issuers entering and existing issuers expanding service areas. Only one state (Delaware) has a single QHP issuer in PY21, compared to two states in PY20.67
A November 2020 Kaiser Family Foundation analysis of insurer participation in al states’ individual exchanges from 2014 to 2021 also indicates such participation is rising for the third consecutive year and “there wil be an average of 5.0 insurers per state in 2021, up from a low of
3.5 in 2018 but stil below the peak of 6.0 in 2015.”68
SHOP Exchanges
Eligibility and Enrollment Certain smal businesses are eligible to use the SHOP exchanges. For purposes of SHOP eligibility, a smal business, or small employer, is general y an employer with not more than 50 employees.69 States also may define small employer as having not more than 100 employees–four states do.70 As of 2017, al states have the option to al ow large employers to use SHOP
exchanges, as wel , but no states have done so.71
SHOP eligibility also depends on an employer having at least at least one common-law employee.72 This means, for example, that a person who is self-employed and who has no
employees would not be eligible for the SHOP exchange (although they could purchase coverage in the individual exchange, if they meet the other eligibility requirements). In addition, per the definition of common-law employee, neither the business owner nor their business partner(s) nor their spouse or family members (even if involved in the business) count as an employee for
purposes of SHOP eligibility.
To participate in a SHOP exchange, a smal business must offer coverage to al of its full-time employees, which, for purposes of SHOP eligibility, means those employeesautomatically reduce monthly premiums by the credit amount. Therefore, the direct cost of insurance to a consumer eligible for premium credits generally will be lower than the advertised cost for a given exchange plan.
In addition to premium tax credits, certain consumers also may be eligible to receive cost-sharing reductions that reduce out-of-pocket expenses.19 There are two forms of cost-sharing reductions, and individuals may receive both if they meet the applicable eligibility requirements.20
The first form of cost-sharing assistance reduces the annual out-of-pocket limit applicable to an individual's exchange plan. Annual out-of-pocket limits apply to all plans in the exchanges and to other plans under the ACA. In 2018, the annual out-of-pocket limit is $7,350 for a self-only plan and $14,700 for coverage other than self-only (e.g., a family plan). In 2019, those limits will be $7,900 and $15,800, respectively.21 This form of cost-sharing assistance further lowers the spending cap for eligible consumers.- The second form reduces cost-sharing requirements applicable to an individual's exchange plan. All exchange plans must meet certain requirements related to actuarial value, or the percentage of allowed health care expenses that issuers will cover. This form of cost-sharing assistance reduces the percentage of costs that the individual is responsible for, effectively raising the actuarial value of the plan.22
SHOP Exchanges
Eligibility and Enrollment Process
Certain small businesses are eligible to use the SHOP exchanges. For the purposes of SHOP exchange participation, states may define small employers (or small businesses) as employers that have 50 or fewer full-time employees or employers that have 100 or fewer full-time employees.23 A majority of states define small as having 50 or fewer employees, and only four states employ the 100-or-fewer-employee definition for their SHOP exchanges.24 As of 2017, all states have the option to allow large businesses to use SHOP exchanges, as well, but no states have taken that option.25
To participate in a SHOP exchange, a small business must offer coverage to all of its full-time employees, meaning those working 30 or more hours per week on average.2673 The business may, but is not required to, offer coverage to part-time or other employees. Employees must meet the same citizenship and other eligibility requirements that apply in the individual exchanges.
67 CMS, CCIIO, Plan Year 2021 Qualified Health Plan Choice and Premiums in HealthCare.gov States, October 2020, at the webpage “Qualified Health Plan Choice and Premiums in HealthCare.gov States,” at https://www.cms.gov/CCIIO/Resources/Data-Resources/QHP-Choice-Premiums. T he corresponding CMS report from October 2019, posted on the same webpage, also showed increasing insurer participation for PY2020 over PY2019.
68 Rachel Fehr et al., “Insurer Participation on the ACA Marketplaces, 2014-2021,” Kaiser Family Foundation, November 2020, at https://www.kff.org/private-insurance/issue-brief/insurer-participation-on-the-aca-marketplaces-2014-2021/. 69 For purposes of SHOP eligibility, the number of employees is determined using the “full-time equivalent” (FT E) employees calculation method. See 45 C.F.R. §155.20, “ Small employer,” which references 26 U.S.C. §4980H. Also see CRS Report R45455, The Affordable Care Act’s (ACA’s) Em ployer Shared Responsibility Provisions (ESRP) for discussion of FT E calculations.
70 California, Colorado, New York, and Vermont are the only states that define small businesses as having 100 or fewer employees for the purpose of participation in the SHOP exchanges. See Table A-1. 71 42 U.S.C. §18032(f)(2)(B). No states have allowed large employers (as defined by the state) use of their SHOP exchanges.
72 For discussion of the SHOP eligibility requirement to have at least one common-law employee, see HHS, “ Patient Protection and Affordable Care Act; Establishment of Exchanges and Qualified Health Plans; Exchange Standards for Employers,” March 27, 2012, 77 Federal Register 18309, page 18399. 73 For purposes of SHOP eligibility, the definition of full-time employee is at 45 C.F.R. §155.20.
Congressional Research Service
19
link to page 7 Overview of Health Insurance Exchanges
or other employees, and/or to the spouses and dependents of any employees offered coverage.74 Employees and their enrolling family members must meet the same citizenship and other
eligibility requirements that apply in the individual exchanges.
Enrollment Periods
Enrollment in a SHOP exchange is not limited to a specified OEP, except in certain
circumstances.75 Such circumstances aside, a SHOP exchange must al ow employers to enroll any time during a year, and the employer’s plan year must consist of the 12-month period beginning with the employer’s effective date of coverage.76 Whereas plans sold in the individual exchanges general y align with the calendar year, plans sold in the SHOP exchanges need not (thus, statutory or regulatory provisions affecting the SHOP exchanges may refer to “plan years beginning in” a
given year).
There are special enrollment periods for SHOP exchange coverage. Some of the special
enrollment periods for the SHOP exchanges are the same as in the individual exchanges.77
Online Enrollment versus Direct Enrollment
For an employee to obtain coverage through a SHOP exchange, a SHOP-eligible employer must select one or more plan options on the SHOP exchange for its employees to choose from.2778 Then, employees compare their employer’s plan options and enroll if they choose. The process of
comparing and enrolling in coverage depends partial y on the type of SHOP exchange a state has:
In states with FF-SHOPs (i.e., states with SHOP exchanges using the federal
HealthCare.gov platform), employers and employees are able to browse and compare plan options on HealthCare.gov, but they need to work directlyemployees can visit the SHOP exchange website to compare their employer's plan options and to enroll. Employers and their employees also can work with a SHOP-registered broker or directly with a plan issuer instead of going through their SHOP exchange's web portal (or if their SHOP exchange does not offer a web portal with enrollment functionality, as discussed below).
Small employers that want to offer more than one plan option to their employees generally are able to do so. Via the employee choice method, also called horizontal choice, the employer can allow its employees to select any plan at a certain coverage and value tier (e.g., a certain metal level of actuarial value).28 As of 2017, there is also a vertical choice method, under which employers can allow their employees to select any plan "across all available actuarial value levels of coverage from a single issuer."29
Changes in SHOP Exchange Web Portal Functionality
Citing early difficulties in getting some SHOP exchange websites online, CMS issued guidance in March 2014 that exchanges still developing their SB-SHOP websites could use a direct enrollment approach for plan year 2014, meaning small businesses and their employees would work directly with agents, brokers, or issuers to compare and purchase coverage rather than enrolling online.30 In subsequent guidance, CMS extended that policy for plan years beginning in 2015-2019, still for SB-SHOPs only. As of April 2016, CMS indicated that SB-SHOPs would need to implement online portals in time for plan years beginning in 2019 and with a
SHOP-registered agent, broker, or insurer to purchase coverage.79 This is cal ed direct enrollment, and it has been the only option in such states since plan years beginning in 2018.80 Previously, employers and employees could purchase coverage on HealthCare.gov or via direct enrollment.
74 45 C.F.R. §155.710(e). 75 It is possible for SHOP exchanges to establish minimum participation rates and minimum contribution rates. Businesses that do not comply with established rates cannot be prohibited from obtaining coverage through SHOP exchanges; rather, health insurance plans may limit the availability of coverage for any employer that does not meet an allowed minimum participation or contribution rate to an annual enrollment period—November 15 through December 15 of each year. 76 45 C.F.R. §155.726(b). 77 45 C.F.R. §155.726(c). See also Section 3.4 of the CMS, FFE and FF-SHOP Enrollment Manual, which notes that SHOP exchange SEPs “cross-referenc[e] most, but not all, of the qualifying events listed at 155.420(d) [which lists SEPs for the individual exchanges]. Specifically, SEPs described in 45 CFR §155.420(d)(1)(ii), (3), and (6) do not apply in SHOPs.” 78 A business with locations or employees in multiple states has options for offering SHOP coverage to all its eligible employees. See 45 C.F.R. §155.710 and HealthCare.gov, “ SHOP Coverage for Multiple Locations and Businesses,” at https://www.healthcare.gov/small-businesses/provide-shop-coverage/business-in-more-than-one-state/.
79 HealthCare.gov, “Overview of SHOP: Health insurance for small businesses,” at https://www.healthcare.gov/small-businesses/choose-and-enroll/shop-marketplace-overview/.
80 HHS finalized this change in the 2019 Payment Notice (page 16996), citing generally low employer participation in the SHOP exchanges and decreasing insurer participation (both discussed elsewhere in the SHOP section of this report). HHS also confirmed in the 2019 Payment Notice that because of these reductions in federal SHOP we b portal functionality, state-based SHOP exchanges would no longer be able to use the federal IT platform. In other words, HHS eliminated the SB-FP-SHOP option (discussed in “ State-Based and Federally Facilitated Exchanges”). T he two
Congressional Research Service
20
link to page 35 link to page 35 link to page 44 link to page 35 link to page 8 link to page 35 Overview of Health Insurance Exchanges
States administering their own SB-SHOP websites initial y were al owed to use a
direct enrollment approach, due to early difficulties some states had in getting their SHOP exchange websites online.81 As of April 2016, HHS indicated SB-SHOPs would need to implement online portals in time for plan years beginning in 2019.82 However, in the 2019 Payment Notice, when HHS transitioned HealthCare.gov SHOP exchanges to direct enrollment (see previous bullet), HHS
also announced SB-SHOPs had the option of retaining or returning to a direct enrollment approach or maintaining enrollment sites if they had created them. As of September 2020, 6 of the 15 SB-SHOP states are using a direct enrollment approach only.83
Besides exchange website enrollment versus direct enrollment options, a significant factor affecting access to SHOP plans is whether any insurers are offering plans in that state’s SHOP exchange. For PY2021, there are no insurers offering medical plans in SHOP exchanges in more than half of states.84 In such states, the federal or state SHOP webpage instructs users to work
directly with an agent, broker, or insurer to obtain coverage in the smal -group market off-
exchange.
Following is a summary of SHOP exchange plan availability and enrollment methods, by SHOP
exchange type, for PY2021. See Table A-1 for more information, including by state.
FF-SHOP, 32 states: al direct enrollment only, 9 with and 23 without SHOP
plans.
SB-SHOP, 18 states: 7 states with plans and SHOP website enrollment option, 6
with plans and direct enrollment only, and 5 with no SHOP plans.
No SHOP, 1 state: state received waiver al owing it not to have a SHOP.85
states that used this option at the time, Kentucky and Nevada, were allowed to continue doing so if desired, despite the reduced functionality of HealthCare.gov for SHOP. However, they have since transitioned their SHOPs to other types (see Table A-1). Citation for this rule is in Table D-1.
81 For iterations of guidance on this topic issued between 2014 and 2016 , see CMS, CCIIO, “Extension of State-Based SHOP Direct Enrollment T ransition,” April 18, 2016, at https://www.cms.gov/CCIIO/Resources/Regulations-and-Guidance/Downloads/1332-and-SHOP-Guidance-508-FINAL.PDF. 82 Ibid. In April 2016, CMS also outlined different options for those states to consider, including transitioning to the federal IT platform (becoming an SB-FP-SHOP) or applying for an ACA Section 1332 waiver to obtain an exception to the requirement to have a SHOP exchange at all. For more information about ACA Section 1332 waivers, see CRS Report R44760, State Innovation Waivers: Frequently Asked Questions.
83 See Table A-1. 84 T he number of states with no insurers offering plans in SHOP exchanges in 2021 is based on CRS analysis of the 2021 “Business Rules” public use file at CMS, “ Health Insurance Exchange Public Use Files (Exchange PUFs),” at https://www.cms.gov/CCIIO/Resources/Data-Resources/marketplace-puf, as well as information available on HealthCare.gov and state exchange websites. Comparable information about insurer participation in SHOP exchanges in prior years may not be consistently available. However, a 2019 GAO report indicates that in 2015-2017, there was at least one insurer participating in each of the 46 of 51 states for which it had such data for all three of those years. See T able 7 in GAO, Private Health Insurance: Enrollm ent Rem ains Concentrated Am ong Few Issuers, Including in Exchanges, March 21, 2019, at https://www.gao.gov/products/GAO-19-306. Hereinafter referred to as “ GAO Enrollment Report, March 2019.”
85 See footnote 18. See Table A-1 for details and citations.
Congressional Research Service
21
link to page 18 link to page 18 link to page 16 Overview of Health Insurance Exchanges
Enrollment Estimates
Unlike individual exchange enrollment data, SHOP exchange enrollment data are not released annual y. However, CMS estimated that there were approximately 27,000 smal employers and 233,000 employees using the SHOP exchanges across the country in January 2017.86 CMS previously estimated 10,700 active smal employers and 85,000 employees in the SHOP
exchanges as of May 2015.87
According to a 2019 GAO report that included 2016 SHOP exchange enrollment data for 46
states,
As a proportion of the overall small group market, SHOP exchanges in most states had little enrollment—that is, typically less than 1 percent of the overall small group market .. The District of Columbia, Rhode Island, and Vermont were the only states where the SHOP exchange was more than 3 percent of the overall small group market. The District of Columbia and Vermont require all small group plans to be purchased through the state’s SHOP exchange.88
In addition, District of Columbia SHOP enrollment includes congressional Members and staff, as
discussed below.
Congressional Member and Staff Enrollment via the D.C. SHOP Exchange
Per the ACA, Members of Congress and their staff general y are required to obtain their health insurance through the exchanges in order to receive a government contribution (i.e., their employer’s contribution) for their coverage.89 As implemented, they purchase coverage through
the District of Columbia’s SHOP exchange. Congressional offices are not eligible for the smal business tax credit (discussed below), and congressional Members and staff obtaining coverage through the SHOP are not eligible for the PTC and CSRs that are available to individuals who enroll in coverage offered on the individual exchanges (see “Premium Tax Credits and Cost-
Sharing Reductions”).
Premiums and Cost Sharing The section earlier in this report on “Premiums and Cost Sharing” in the individual exchanges,
including certain federal requirements that apply to premiums and cost sharing, general y applies in the SHOP exchanges, as wel . See CRS Report R45146, Federal Requirements on Private Health Insurance Plans for other requirements applicable to the individual and smal -group
markets, on and off the exchanges.
86 T his estimate excludes Hawaii, as Hawaii’s SHOP exchange was no longer operatio nal in 2017 due to the state’s receipt of a 1332 waiver. See CMS, CCIIO, “ SHOP Marketplace Enrollment as of January 2017,” May 15, 2017, at https://www.cms.gov/CCIIO/Resources/Data-Resources/Downloads/ SHOP -Marketplace-Enrollment -Data.pdf.
87 T his estimate excludes Vermont and Idaho; these states had not reported 2015 enrollment data to CMS. See CMS, “Update on SHOP Marketplaces for Small Businesses,” July 2, 2015, archived at http://wayback.archive-it.org/2744/20170118124128/https:/blog.cms.gov/2015/07/. 88 See page 24 and Appendix III of the GAO Enrollment Report, March 2019. 89 Other federal employees may obtain coverage through the Federal Employees Health Benefits Program (FEHB). Like many other employers, the federal government contributes to the cost of its employees’ premiums. T his is also true for the Congressional Members and staff who obtain coverage through the SHOP. Certain congressional staff may not be required to obtain their coverage through the SHOP, and may be able to otherwise obtain coverage through FEHB. See Office of Personnel Management, “ Members of Congress and Designated Staff – General,” at https://www.opm.gov/healthcare-insurance/changes-in-health-coverage/changes-in-health-coverage-faqs/.
Congressional Research Service
22
link to page 18 link to page 23 Overview of Health Insurance Exchanges
Employers who offer coverage through the SHOP exchange, like employers who offer coverage otherwise, may choose to subsidize their employees’ premiums. This means the employer pays
for part of their employees’ premiums.
CRS is not aware of HHS or other reports on premium or cost-sharing data specific to the SHOP
exchanges.
exchange at all.31
Via the "2019 Notice of Benefit and Payment Parameters" (2019 Payment Notice) finalized in April 2018, HHS signaled a new policy direction, citing generally low employer participation in the SHOP exchanges and decreasing issuer participation.32 For plan years beginning in 2018, the direct enrollment approach is not just a transitional option for SB-SHOP states: it is the only option in FF-SHOP and SB-FP-SHOP states.33 Although small businesses using the SHOP exchange in those states still will be able to use the Healthcare.gov portal to browse plans and determine their eligibility for small business tax credits (discussed below), they will not be able to enroll in a plan through the SHOP web portal. States with SB-SHOPs also can choose to maintain or return to a direct enrollment approach or to maintain online enrollment, if they have it.
HHS also confirmed in the 2019 Payment Notice that because of these reductions in federal SHOP web portal functionality, going forward, state-based SHOP exchanges will not be able to use the federal IT platform. In other words, HHS is eliminating the SB-FP-SHOP option (discussed above in "Types of Exchanges"). The two states that currently use this option, Kentucky and Nevada, may continue to do so if desired, knowing that the Healthcare.gov functionality is to be diminished.
As of June 2018, three SB-SHOP states still use their initial direct enrollment approaches and five other SB-SHOPs are transitioning to this approach and/or are instructing small businesses to enroll directly with issuers off the exchange because no issuers are offering plans in their SHOP exchange in 2018.34 For FF-SHOP and SB-FP-SHOP exchange states, Healthcare.gov instructs users of the new direct enrollment approach.35
Enrollment Periods and Enrollment Estimates
Enrollment in a SHOP exchange is not limited to a specified OEP, except in certain circumstances.36 Specific circumstances aside, a SHOP exchange must allow employers to enroll any time during a year, and the employer's plan year must consist of the 12-month period beginning with the employer's effective date of coverage.
Unlike individual exchange enrollment data, SHOP exchange enrollment data are not released annually. However, CMS estimated that there were approximately 27,000 small employers and 233,000 employees using the SHOP exchanges across the country in January 2017.37 CMS previously estimated 10,700 active small employers and 85,000 employees in the SHOP exchanges as of May 2015.38
Small Business Health Care Tax Credit
Certain small Small Business Health Care Tax Credit
Certain smal businesses are eligible for small for the smal business health care tax credits.39credit (SBTC).90 In general, these credits arethis credit is available only to small businesses that purchase coverage through SHOP exchanges and subsidize their employees' premiums. The intent of the credit is to assist small only to smal employers with 25 or fewer full-time-equivalent
(FTE) employees that purchase coverage through SHOP exchanges and contribute at least 50% of premium costs for their full-time employees.91 (For the purpose of this tax credit, full-time employees are those who work an average of 40 hours per week, whereas for the purpose of SHOP eligibility, full-time employees are those who work an average of 30 hours per week.92) The intent of the credit is to assist smal employers with the cost of providing health insurance
employers with the cost of providing health insurance coverage to employees. The credits arecredit is available to eligible small smal businesses for two consecutive tax years (beginning with the first year the small smal employer purchases coverage through a SHOP
exchange).
The maximum credit is 50% of an employer'
In states with no insurers offering plans through the SHOP exchange (see discussion above), certain eligible employers stil may be able to receive the credit. If they received their first year’s credit by offering coverage through the SHOP exchange and there were no SHOP plans available the next year, they may receive their second consecutive year’s credit with a plan purchased off-
exchange.93
The maximum credit is 50% of an employer’s contribution toward premiums for for-profit employers and 35% of employer contributions for nonprofit organizations. The full credit is available available to employers that have 10 or fewer full-time equivalent (FTE)FTE employees who have average taxable wages of $26,600
$27,800 or less (in 2018).402021).94 In general, the credit is phased out as the number of FTE employees increases from 10 to 25 and as average employee compensation increases to a maximum of two
times the limit for the full credit.41
95
Employees who enroll in a SHOP plan do not receive this tax credit, nor are they eligible for the premium tax credit or cost-sharing reductions for the financial assistance available to certain consumers who purchase coverage on the individual
market (see “market (discussed in this report in "Premium Tax Credits and Cost-Sharing Reductions").
Individual and SHOP Exchange Enrollment Assistance
Statute and regulations require that exchanges—both individual and SHOP—carry out certain consumer-assistance functions.42 Exchanges (both federally facilitated and state-based) must establish Navigator programs and certified application counselor (CAC) programs.43 Under these programs, individuals are trained to conduct public outreach and education activities; help consumers make informed decisions about their insurance options; and help consumers access individual and SHOP exchange coverage and cost-sharing assistance or public program coverage (e.g., Medicaid or CHIP) if they qualify. Although consumer assistance personnel (including Navigators and CACs) can help consumers and small employers understand their options, the assistors may not advise them on which plan to select. Once consumers or small employers choose a plan, assisters may help them enroll in coverage. Neither Navigators nor CACs may be health issuers or take compensation from issuers or consumers for selling health policies.44
Pursuant to state law, exchanges also may allow insurance agents and brokers, including web-based brokers, to help consumers and small employers obtain coverage through exchanges.45 Brokers and agents are licensed by the states and generally are paid on a commission basis by insurance companies.
Besides facilitating in-person assistance, exchanges also must provide for the operation of a call center and maintain a website that meets certain informational requirements.46 Overall, exchanges' consumer outreach efforts and materials must meet certain standards regarding accessibility for individuals with disabilities or with limited English proficiency.47
Administering the Exchanges
In addition to carrying out their consumer-facing activities that facilitate the purchase of coverage, exchanges are responsible for several administrative functions, including certifying the plans that will participate in their marketplaces.48 SBEs, SBE-FPs, and state entities in some FFEs (where states have chosen to perform some plan-management functions) are each responsible for annually certifying or recertifying plans to be sold in their exchanges as qualified health plans (QHPs, see "Qualified Health Plans," below). In FFEs in which HHS oversees all plan-related functions, CMS does this for each state.
QHP certification involves a review of various factors, including the benefits a plan will cover, the network of providers it will include, its premium rates, its marketing practices, and its adherence to quality-of-care standards.49 The QHP certification process is to be completed each year in time for issuers to advertise their plans and rates during the exchanges' annual OEP.
Exchanges' other administrative activities include collecting enrollment and other data, reporting data to and otherwise interacting with the Departments of HHS and the Treasury, and working with state insurance departments and federal regulators to conduct ongoing oversight of plans.
Qualified Health Plans
In general, health insurance plans offered through exchanges must be QHPs.50A QHP is a plan that is offered by a state-licensed issuer that meets specified requirements, is certified by an exchange, and covers the essential health benefits (EHB) package.51 The EHB package requires plans to cover 10 broad categories of benefits and services, comply with limits on consumer cost sharing on the EHB, and meet certain generosity requirements.52
QHPs must comply with the same state and federal requirements that apply to health plans offered outside of exchanges.53 A QHP offered through an individual exchange must comply with state and federal requirements applicable to individual market plans; a QHP offered through a SHOP exchange must comply with state and federal requirements applicable to plans offered in the small-group market. For example, QHPs offered through individual and SHOP exchanges must cover specified preventive services without imposing cost sharing, just like plans offered in the individual and small-group markets outside of exchanges.
A QHP is the only type of comprehensive health plan an exchange may offer, but QHPs may be offered outside of exchanges, as well.
Types of QHPs and Other Plans Offered Through Exchanges
Most plans offered in the exchanges are QHPs, including child-only plans, catastrophic plans, consumer operated and oriented plans (CO-OPs), and multi-state plans (MSPs). Stand-alone dental plans are the only non-QHPs offered in the exchanges. Some plans that are available in the exchanges also are available off the exchanges.
The types of plans that may be available through exchanges are summarized in Table B-1.
Exchange Funding
The ACA provided an indefinite ” above).
90 See 26 U.S.C. §45R for eligibility for the Small Business Health Care T ax Credit (SBT C) and credit amount details described in this section.
91 See the SHOP “ Eligibility and Enrollment ” section of this report for discussion of full-time equivalent employees. 92 Regarding SHOP eligibility, see 26 U.S.C. §4980H, 26 CFR §54.4980H-1(a)(21), and 45 CFR §155.20. Regarding the SBT C, see 26 U.S.C. §45R. 93 Internal Revenue Service (IRS), Small Business Health Care Tax Credit Questions and Answers: Who Gets the Tax Credit, Question 6D, updated September 2020, at https://www.irs.gov/newsroom/small-business-health-care-tax-credit -questions-and-answers-who-gets-the-tax-credit.
94 IRS, Rev. Proc. 2020-45, Section 3.11, at https://www.irs.gov/pub/irs-drop/rp-20-45.pdf, referring to 26 U.S.C. §45R(d)(3)(B).
95 26 U.S.C. §45R(d)(1)(B).
Congressional Research Service
23
link to page 21 link to page 21 link to page 24 link to page 44 Overview of Health Insurance Exchanges
The IRS has published information on the number of SBTCs filed in tax years 2010-2016.96 For 2016, the IRS indicates that 6,952 employers claimed the SBTC.97
Insurer Participation As stated above, as of PY2020, there are no insurers offering SHOP plans in more than half of
states.98
Some of the factors affecting insurer participation in the individual exchanges (see “Insurer Participation” in the Individual Exchanges section above) also may affect insurer participation in the SHOP exchanges. For example, just as in the individual market, there were new federal requirements imposed by the ACA on plans sold in the smal -group market (including the SHOP exchanges), and insurers in the smal -group market were or are participating in risk-mitigation
programs.
There are also factors unique to the SHOP exchanges that may have affected insurer participation.
For example, in December 2016, effective January 2018, HHS removed a requirement that in order to participate in a federal y facilitated individual exchange, an insurer with more than 20% of the smal -group market in that state also would have to participate in that SHOP exchange. In the rule, HHS acknowledged the elimination of this requirement likely would reduce insurer participation, and thus employer and employee participation, in affected SHOP exchanges.99 Other issues also have been discussed as affecting employer and/or insurer participation in the
SHOP exchanges, such as delays in setting up online enrollment capabilities when the SHOPs were being established and the limited duration and administrative complexity of the smal
business tax credit.100
Exchange Enrollment Assistance
Navigators and Other Exchange-Based Enrollment Assistance Federal statute and regulations require exchanges to carry out certain consumer outreach and assistance functions. These functions general y include in-person and other forms of outreach and
assistance.101
Each exchange must have a Navigator program.102 Navigators are entities whose employees and/or volunteers conduct public outreach and education activities about the exchanges and
96 IRS, SOI Tax Stats - Affordable Care Act (ACA) Statistics: Credit for Small Employer Health Insurance, “Premiums,” page updated Sept. 2020, at https://www.irs.gov/statistics/soi-tax-stats-affordable-care-act-aca-statistics-credit-for-small-employer-health-insurance-premiums. 97 Ibid. See excel file, “ Small Business Health Care T ax Credits Filed in T ax Years 2010–2016,” linked on this webpage.
98 See “Online Enrollment versus Direct Enrollment 99 2018 Payment Notice, page 94144. Citation for this rule is at Table D-1. 100 See GAO, Small Business Health Insurance Exchanges: Low Initial Enrollment Likely due to Multiple, Evolving Factors, November 2014, at https://www.gao.gov/products/GAO-15-58. Also see Jost, T imothy, “ CMS Announces Plans T o Effectively End T he SHOP Exchange,” Health Affairs Blog, May 15, 2017, at https://www.healthaffairs.org/do/10.1377/hblog20170515.060112/full/.
101 For example, see 42 U.S.C. §18031(i), 45 C.F.R. §155.205, 45 C.F.R. §155.210, and 45 C.F.R. §155.225. 102 Ibid. Specifically, for the requirement to implement Navigator programs, see 45 C.F.R. §155.210.
Congressional Research Service
24
link to page 44 Overview of Health Insurance Exchanges
QHPs; provide impartial information to consumers (including smal employers and their employees) about their insurance options; help consumers access individual and SHOP exchange coverage, exchange financial assistance, and/or public program coverage (e.g., Medicaid or CHIP) if they qualify; and refer consumers to any applicable consumer assistance programs as needed, such as state agencies that assist consumers with questions or complaints about their plans. Navigators also may, but are not federal y required to, provide other assistance, such as
information or referrals regarding reconciliation of consumers’ PTCs via their annual income tax filing.103 States may impose additional Navigator requirements, as long as “such standards do not
prevent the application of the provisions of title I of the Affordable Care Act.”104
Navigators are funded by the exchanges, via grants (federal or state, depending on exchange type) provided to qualifying organizations. Information on current and prior-year Navigator grantees in FFE states is available on the CMS website.105 For FFE states, certain eligibility requirements changed in 2018 and 2019. For example, Navigator entities are no longer required to maintain a
physical presence in their exchange service area.106
Exchanges also must have a Certified Application Counselor (CAC) program.107 CAC staff and/or volunteers also provide impartial information to consumers about their insurance options
and can assist them in applying for individual and SHOP exchange coverage, exchange financial assistance, and/or public program coverage (e.g., Medicaid or CHIP) if they qualify. They do not necessarily provide public outreach and education or perform many of the other functions that Navigators do. CACs are not exchange-funded in FFE states and are not required to be exchange-
funded in other states.
Although Navigator and CAC assisters can help consumers understand their options, they may not advise them on which plan to select. Once a consumer chooses a plan, the assisters may help them enroll in coverage. Neither Navigators nor CACs may be health insurers or take
compensation for sel ing health policies from insurers or consumers.108
Besides facilitating the above assistance programs, exchanges must provide for the operation of a cal center and maintain a website (e.g., HealthCare.gov) that meets certain informational
requirements.109 Exchanges also provide consumer information and outreach via mail, radio or
television ads, and/or other methods.
103 Some functions that were previously required are now optional for federally -funded Navigator grantees. See 45 C.F.R. §155.210(e)(9).
104 45 C.F.R. §155.210(c)(1)(iii). 105 For information on FFE Navigator grants, see CMS, “ In-Person Assistance in the Health Insurance Marketplaces,” at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/assistance. Per the list of 2020 grantees, there were no eligible applicants in FFE states South Carolina and Utah. CRS is not aware of a compilation of information about Navigator grants in states that administer these programs (those with SBEs and SBE-FPs).
106 T he eligibility requirement changes were made via the 2019 and 2020 Payment Notices (cited in Table D-1). T he changes, and existing eligibility requirements, are summarized in the 2019 Navigator funding opportunity announcement, Cooperative Agreem ent to Support Navigators in Federally-facilitated Exchanges, at https://www.grants.gov/web/grants/search-grants.html?keywords=CA-NAV-19-001 (select “ archived” option under “opportunity status”). 107 For the requirement to implement certified application counselor programs, see 45 C.F.R. §155.225. 108 45 C.F.R. §155.215. 109 45 C.F.R. §155.205.
Congressional Research Service
25
link to page 23 Overview of Health Insurance Exchanges
Overal , exchanges’ consumer outreach efforts and materials must meet certain standards
regarding accessibility for individuals with disabilities or with limited English proficiency.110
Brokers, Agents, and Other Third-Party Assistance Entities Pursuant to state law, exchanges also may certify insurance agents, brokers, and/or web-brokers
to help consumers obtain coverage through exchanges.111
An agent or broker is “a person or entity licensed by the State as an agent, broker
or insurance producer.”112 They may be individuals or entities that sel plans for different insurance companies, general y receiving a commission from those companies for doing so; or they may be employees of an insurance company who help people enroll in that company’s plans.
A web-broker is an exchange-certified individual or group of agent(s) or
broker(s), or other business entity (including a “direct enrollment technology provider”), “that develops and hosts a non-Exchange website that interfaces with an Exchange to assist consumers with direct enrollment in qualified health plans
offered through the Exchange.”113 In other words, they offer privately owned and operated websites that may be similar in concept to the ACA exchange websites, in that they al ow for comparison of purchase of different plans.
If certified to sel exchange plans, any of these “third party” entities must follow rules about providing information and access to al plans that would be available to a consumer on the actual exchange website.114 Unlike the exchange websites and exchange assistors, however, they may
also assist consumers with enrolling in plans that are not available on the exchanges.
In states where SHOP exchanges only offer direct enrollment (i.e., consumers cannot purchase SHOP plans via the exchange website), or in states where there are no insurers offering SHOP plans, the SHOP exchange websites direct consumers to these third party assisters, who can help
them enroll in SHOP plans and/or smal -group plans available off-exchange.115
Exchange Spending and Funding
Initial Grants for Exchange Planning and Establishment The ACA provided an indefinite (i.e., unspecified) appropriation for HHS grants to states to support the planning and establishment of exchanges.54116 For each fiscal year between (FY) between
FY2011 and FY2014, the HHS Secretary determined the total amount that was made available to
110 45 C.F.R. §155.205. 111 45 C.F.R. §155.220. Definitions of terms discussed in this section, and of other related terms such as direct enrollm ent entity, are at 45 C.F.R. §155.20.
112 Ibid. 113 Ibid. See 45 C.F.R. §155.20 for full definition of this term. 114 45 C.F.R. §155.220. 115 See “Eligibility and Enrollment ” in the SHOP section of this report for more information about SHOP exchange enrollment options and plan availability.
116 42 U.S.C. §18031(a).
Congressional Research Service
26
link to page 42 link to page 44 Overview of Health Insurance Exchanges
each state for exchange grants. However, none of these exchange grants could be awarded after
January 1, 2015, and exchanges were expected to be self-sustaining beginning in 2015.
117
Ongoing Federal Spending on Exchange Operation The federal government spent an estimated $1.8 bil ion on operating the exchanges in FY2020, and it projected $1.2 bil ion in spending for FY2021.118 See Figure C-1, which includes these numbers as wel as estimated and prior year federal spending on the exchanges by activity (e.g., information technology, Navigator grants), in a table that is included by CMS in its annual budget
justification to Congress.
In general, this federal spending is specific to FFEs. For example, the federal government funds the Navigator program only in states with FFEs. Some of the federal spending, particularly in
terms of information technology and the cal center, also is applicable to SBE-FPs, because these state-based exchanges use the federal HealthCare.gov platform. CMS performs and funds ae some functions for al exchanges, including SBEs, such as “verifying consumers’ eligibility data for financial assistance through the Exchange or other health insurance programs, including
Medicaid and the Children’s Health Insurance Program (CHIP).”119
The costs of the plans themselves are covered by enrollees’ premiums and in some cases are subsidized by the federal government (i.e., via PTCs). The costs of the PTCs are financed through a permanent appropriation through the tax code.120 These tax credit costs are beyond the scope of
this report and are not included in the funding totals discussed in this section.
Funding Sources for Federal Exchange Spending
User Fees Collected from Participating Insurers
Exchanges may generate funding to sustain their operations, including by assessing fees on
Exchanges may generate funding to sustain their operations, including by assessing fees on participating health insurance plans.55121 To raise funds for the exchanges it overseesadministers and/or for which it provides a web platform, HHS assesses a monthly fee on each health insurance issuer that offers plans through an FFE or SBE-FP. The fee is a percentage of the value of the monthly premiums that the issuer collects on exchange plans in a given state, and HHS updates the percentage each year through rulemaking. (See Table 2.) Currently, these user fees are the primary source of funding for FFEs; they are estimated to account for 70% of all FFE funding in FY2018.56
Most SBEs also assess user fees on issuers participating in their exchanges, often 1%-3% of premiums or a monthly flat fee.57 States also can use other state funding to support their exchanges, and some have become FFEs or moved to the federal IT platform due to challenges and/or costs of maintaining their exchanges.58
User fees also have been assessed on issuers participating in SHOP exchanges. However, in the 2019 Payment Notice, HHS announced that the fees won't be assessed for issuers selling plans under the new model of reduced federal IT support (see "Changes in SHOP Exchange Web Portal Functionality" in this report).
Table 2. "User Fee" Assessed Monthly on Issuers Participating in Exchanges, by Year
(fee is the stated percentage of the value of monthly premiums collected by issuer FFE or SBE-FP. The user fee amounts are al owed to fund only federal activities or functions specific to these exchanges; the user fees cannot fund federal activities that serve al exchanges (including SBEs).122 The fees are lower for insurers in SBE-FP
states because the federal government performs fewer functions for those exchanges than for
FFEs, but those insurers also may be subject to exchange participation fees levied by the states.
117 42 U.S.C. §18031(a)(4)(B) specifies that no grant shall be awarded under this subsection after January 1, 2015. See CRS Report R43066, Federal Funding for Health Insurance Exchanges (last updated in October 2014) for more information about these planning and establishment grants. 118 Department of Health and Human Services, Centers for Medicare & Medicaid Services, Justification of Estimates for Appropriations Com m ittees, Fiscal Year 2021, March 3, 2020, at https://www.cms.gov/About -CMS/Agency-Information/PerformanceBudget/FY2021-CJ-Final.pdf. See “ Federal Exchanges” table and narrative, page 195 -200, and “Health Insurance Exchange T ransparency Table,” page 241. T he HHS FY2020 spending estimate was as of January 2020. Hereinafter referred to as “ CMS Budget Justification, FY 2021.”
119 Page 196 of the CMS Budget Justification, FY2021. 120 31 U.S.C. §1324(b). 121 42 U.S.C. §18031(d)(5)(A). 122 For further discussion, see 2020 Payment Notice (cited in Table D-1), Section E.2., page 29216. Also see discussion of CMS activities conducted on behalf of certain versus all exchanges at CMS Budget Justification, FY2021, page 196.
Congressional Research Service
27
link to page 32 link to page 32 link to page 44 link to page 6 link to page 44 link to page 24 link to page 43
Overview of Health Insurance Exchanges
The fee is a percentage of the value of the monthly premiums the insurer collects on exchange plans in a given state, and HHS updates the percentage each year through rulemaking. See Figure
3.
User fees also have been assessed on insurers participating in SHOP exchanges. However, HHS announced in the 2019 Payment Notice that as of plan years beginning on or after January 1, 2018, the fees would no longer be assessed on insurers participating in FF-SHOPs and SB-FP-SHOPs, due to the reduced functionality of the federal SHOP website also announced in that
rule.123
Figure 3. Federal User Fee for Insurers Participating in Specified Types of Individual
Exchanges, by Plan Year
(fee is the stated percentage of the value of monthly premiums col ected by insurer on exchange plans)
Source: CRS analysis of annual “Payment Notice” federal rules cited in Table D-1, as wel as Internal Revenue Service, “Rev. Proc. 2013-25,” May 2, 2013, at http://www.irs.gov/pub/irs-drop/rp-13-25.pdf. Notes: FFE = federal y-facilitated exchange. SBE = state-based exchange. SBE-FP = state-based exchange using the federal information technology (IT) platform. See “Types and Administration of Exchanges” for discussion of exchange types. Although some SBE-FPs existed prior to plan year 2017, HHS did not begin assessing a user fee on insurers in those states until then. SBEs’ assessment of user fees, if any, varies, as discussed in this section of the report.
Most of the total federal spending on exchange operations is funded by these user fees. In FY2018-FY2020, user fees funded between 65.3% and 78.8% of this federal spending.124 As stated above, the user fees only fund activities specific to FFEs and certain activities for SBE-FPs. Funding sources for federal activities applicable also to SBEs are discussed in the next
section.
123 2019 Payment Notice (cited in Table D-1), page 17007. See “ Online Enrollment versus Direct Enrollment” regarding the reduced functionality of federal SHOP websites.
124 Based on CRS analysis of data provided in CMS Budget Justifications for FY2021 and FY2020 (see Table C-1). Comparable data not found in prior years’ budget justifications.
Congressional Research Service
28
link to page 31 link to page 43 link to page 21 link to page 43 Overview of Health Insurance Exchanges
For FY2021, CMS proposed that $1.12 bil ion, or 93.6%, of its overal estimated FY2021 exchange spending would come from anticipated user-fee collections.125 However, this higher percentage of spending sourced from user fees likely would depend on enactment of a legislative proposal included by CMS in its FY2021 budget. The proposal would “al ow user fees collected for FFE operations to be available for any federal administrative Exchange-related operating activity.”126 This means CMS could use the user fees to fund its activities performed for al
exchanges, not just for its activities that are specific to FFE and SBE-FP exchanges. If this proposal is not enacted, CMS must continue to use other funding sources for the activities it performs on behalf of al exchanges. See “Ongoing Federal Spending on Exchange Operation”
for examples of these different types of activities.
Other Federal Funding Sources
Besides the user fees collected from participating insurers, federal funding for the exchanges (including for federal activities related to al exchanges, including SBEs) largely comes from discretionary appropriations for program management and program integrity. There is also a risk-adjustment user fee, related to the risk-mitigation program briefly mentioned earlier in this report.127 There is currently no mandatory HHS appropriation for exchange activities.128 An
overview of recent and currently proposed funding sources is in Table C-1.
State Financing of the Exchanges States with SBEs finance their own exchange administration. States with SBE-FPs also finance the costs associated with the exchange functions they administer (whereas the federal user fee is assessed on insurers in such states to finance federal y run functions such as the IT platform, as discussed above). States may finance their exchanges by collecting user fees from participating insurers, as the federal government does. In addition, states may use other state funding to support
their exchanges. CRS is not aware of an estimate of total or state-level spending on, or financing
sources for, SBE and SBE-FP exchanges.
125 Ibid. 126 CMS Budget Justification, FY2021, page 199. 127 See “Insurer Participation” in the Individual Exchanges section of the report. 128 According to the “Federal Exchanges” table in the FY2020 CMS CJ, a portion of the mandatory Health Care Fraud and Abuse Control (HCFAC) appropriation went to the exchanges in FY2018 and FY2019. However, that ta ble in the FY2021 CJ does not show this for FY2019. See Table C -1 for citations.
Congressional Research Service
29
link to page 28 link to page 35 link to page 24 Overview of Health Insurance Exchanges
Appendix A. Exchange Information by State As discussed in this report, the major types of exchanges in terms of state versus federal administration are state-based exchanges (SBEs), federal y facilitated exchanges (FFEs), and state-based exchanges using a federal platform (SBE-FPs). For plan year (PY) 2021, there are 30
FFEs, 15 SBEs, and 6 SBE-FPs.
A few states have changed approaches one or more times (e.g., initial y worked to create an SBE but then switched to an SBE-FP or FFE model). Changes in the first few years varied in terms of whether the state moved toward more or less federal involvement, but in several cases, a state transitioned from a fully state-based approach to an SBE-FP (i.e., transitioned toward more
federal involvement). Recent and ongoing transitions general y are in the direction of less federal involvement. There were three changes for PY2015, one for PY2016, three for PY2017, none for PY2018 or PY2019, three for PY2020, and four for PY2021. As of the publication of this report,
five states are known to be transitioning or considering transitions for PY2022 or beyond.
SHOP exchanges may be federal y facilitated (FF-SHOP) or state-based (SB-SHOP).129 For PY2021, there are 32 FF-SHOPs and 18 SB-SHOPs. However, in more than half of states, no insurers are offering medical plans in the SHOP exchange, meaning there is effectively no SHOP exchange there. See “Insurer Participation” in the SHOP Exchanges section of this report for
more information. One state is exempted from operating a SHOP exchange.
For PY2021 plan, most states’ individual and SHOP exchanges are administered in the same way
(i.e., both state based or both federal y facilitated). However, a handful of states have different approaches for their individual and SHOP exchanges. Some resources refer to this as a bifurcated
approach.
Table A-1 shows individual exchange types by state, with information on past changes in individual exchange types and changes underway or planned. It also shows SHOP exchange types
by state and provides details on SHOP plan availability and enrollment method.
129 As of June 2018, states can no longer select the state-based using the federal IT platform (SB-FP-SHOP) approach, except that the two states with that model at that time (Nevada and Kentucky) could maintain it . According to CMS, those states no longer use that model. For more information, see “ Online Enrollment versus Direct Enrollment” in the “SHOP Exchanges” section of this report.
Congressional Research Service
30
link to page 37 link to page 37 link to page 37 link to page 37 link to page 37 link to page 37 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 37 link to page 37 link to page 38 link to page 37 link to page 38 link to page 37 link to page 38 link to page 37 link to page 38 link to page 38 link to page 37 link to page 37 link to page 38 link to page 37 link to page 38 link to page 37 link to page 37 link to page 37 link to page 37 link to page 38 link to page 37 link to page 37 link to page 38 link to page 38 link to page 37 link to page 38 link to page 37 Overview of Health Insurance Exchanges
Table A-1. Exchange Types and Key Details by State, Plan Year 2021
Individual Exchange Typea
SHOP Exchange Typeb
(and notes on exchange type
(with notes on plan availability and
State
Exchange Website
transitions, if applicable)
enrol ment options)
U.S. Totals
FFE: 30
FF-SHOP: 32 (23 have no plans;
SBE: 15
al are direct enrol ment only)
SBE-FP: 6
SB-SHOP: 18 (5 have no plans; 6 are direct enrol ment only)
(plans and online enrol ment available in al counties, al states)
No SHOP: 1
Alabama
HealthCare.gov
FFE
FF-SHOP, via direct enrol mentc
Alaska
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Arizona
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Arkansas
Myarinsurance.com;
SBE-FP as of PY17
SB-SHOP, but no medical plansf
HealthCare.gov
(initial y FFE)e
California
Coveredca.com
SBE
SB-SHOP (up to 100 employees) g
Colorado
Connectforhealthco.com
SBE
SB-SHOP, via direct enrol menth
(up to 100 employees)g
Connecticut
Accesshealthct.com
SBE
SB-SHOP
Delaware
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
District of
DChealthlink.com
SBE
SB-SHOP
Columbia
Florida
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Georgia
HealthCare.gov
FFE (planning to replace exchange
FF-SHOP, via direct enrol mentc
with alternate approach as of PY23) j
Hawai
HealthCare.gov
FFE as of PY17 i (initial y SBE, then
No SHOP exchangek
SBE-FP for PY16)e
Idaho
Yourhealthidaho.org
SBE as of PY15
SB-SHOP, via direct enrol menth
(initial y SBE-FP)e
Il inois
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Indiana
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Iowa
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Kansas
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Kentucky
Healthbenefitexchange.ky.
SBE-FP as of PY17 (initial y SBE)
FF-SHOP, but no medical plansd
gov; HealthCare.gov
Planning for SBE as of PY22e
Louisiana
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Maine
Enrol 207.com;
SBE-FP as of PY21 (initial y FFE)i
FF-SHOP, via direct enrol mentc
HealthCare.gov
Considering SBEe
Maryland
Marylandhealthconnection.
SBE
SB-SHOP, via direct enrol menth
gov
Massachusetts
Mahealthconnector.org
SBE
SB-SHOP
Michigan
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Minnesota
Mnsure.org
SBE
SB-SHOP, but no medical plansf
Mississippi
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Congressional Research Service
31
link to page 37 link to page 37 link to page 37 link to page 38 link to page 37 link to page 38 link to page 37 link to page 37 link to page 38 link to page 38 link to page 37 link to page 37 link to page 37 link to page 38 link to page 38 link to page 37 link to page 37 link to page 38 link to page 37 link to page 37 link to page 37 link to page 38 link to page 37 link to page 38 link to page 37 link to page 38 link to page 37 link to page 37 link to page 37 link to page 38 link to page 37 link to page 38 link to page 38 link to page 38 link to page 37 link to page 37 link to page 38 link to page 38 link to page 37 link to page 37 link to page 37 Overview of Health Insurance Exchanges
Individual Exchange Typea
SHOP Exchange Typeb
(and notes on exchange type
(with notes on plan availability and
State
Exchange Website
transitions, if applicable)
enrol ment options)
Missouri
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Montana
HealthCare.gov
FFEi
FF-SHOP, via direct enrol mentc
Nebraska
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Nevada
Nevadahealthlink.com
SBE as of PY20 (initial y SBE, then
SB-SHOP, but no medical plansf
SBE-FP as of PY15)e
New
HealthCare.gov
FFEi
FF-SHOP, via direct enrol mentc
Hampshire
New Jersey
Nj.gov/getcoverednj/
SBE as of PY21 (initial y FFE, then
SB-SHOP
SBE-FP as of PY20)e
New Mexico
Bewel nm.com;
SBE-FP
SB-SHOP
HealthCare.gov
Planning for SBE as of PY22e
New York
Nystateofhealth.ny.gov
SBE
SB-SHOP, via direct enrol menth
(up to 100 employees)g
North
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Carolina
North Dakota
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Ohio
HealthCare.gov
FFEi
FF-SHOP, via direct enrol mentc
Oklahoma
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Oregon
Healthcare.oregon.gov/
SBE-FP as of PY15 (initial y SBE)
SB-SHOP, via direct enrol menth
marketplace; HealthCare.gov
Considering SB e
Pennsylvania
Pennie.com
SBE as of PY21 (initial y FFE, then
SB-SHOP, but no medical plansf
SBE-FP as of PY20)e
Rhode Island
Healthsourceri.com
SBE
SB-SHOP
South
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Carolina
South Dakota
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Tennessee
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Texas
HealthCare.gov
FFE
FF-SHOP, but no medical plansd
Utah
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Vermont
Healthconnect.vermont.
SBE
SB-SHOP, via direct enrol menth
gov
(up to 100 employees)g
Virginia
Coverva.org/marketplace;
SBE-FP as of PY21 (initial y FFE i)
FF-SHOP, via direct enrol mentc
HealthCare.gov
Planning for SBE as of PY23e
Washington
Wahealthplanfinder.org
SBE
SB-SHOP, but no medical plansf
West Virginia
HealthCare.gov
FFEi
FF-SHOP, but no medical plansd
Wisconsin
HealthCare.gov
FFE
FF-SHOP, via direct enrol mentc
Wyoming
HealthCare.gov
FFE
FF-SHOP, via direct enrol mentc
Sources: Congressional Research Service (CRS) analysis of data at the sources indicated in notes section below. Notes: SHOP = Smal business health options program. FFE and FF-SHOP = Federal y facilitated individual exchange; federal y facilitated SHOP exchange.
Congressional Research Service
32
link to page 6 link to page 9 link to page 24 Overview of Health Insurance Exchanges
SBE and SB-SHOP = State-based individual exchange; state-based SHOP exchange. SBE-FP = State-based individual exchange using the federal information technology (IT) platform; state-based SHOP exchange using the federal IT platform. Counts of “states” include the District of Columbia. In the individual exchanges, “plan year” is general y that calendar year, but group coverage plan years, including in the SHOP exchanges, may start at any time during a calendar year. See report “Overview” for discussion of exchange types; see Figure 1 in this report for the 2021 exchange types by state in map form. a. 2021 individual exchange types: SBEs and SBE-FPs are listed at Centers for Medicare & Medicaid
Services (CMS), Center for Consumer Information and Insurance Oversight (CCIIO), “State-based Exchanges,” updated November 1, 2019, at https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/state-marketplaces. Remaining states have FFEs. Cross-referenced at Kaiser Family Foundation, “State Health Insurance Marketplace Types, 2021,” at https://www.kff.org/health-reform/state-indicator/state- on exchange plans)
|
PY 2014 |
PY 2015 |
PY 2016 |
PY 2017 |
PY 2018 |
PY 2019 |
|
|
FFE Issuers |
3.5% |
3.5% |
3.5% |
3.5% |
3.5% |
3.5% |
|
SBE-FP Issuers |
n/a |
n/a |
n/a |
1.5% |
2% |
3% |
Sources: CRS analysis of federal regulations: HHS, "Patient Protection and Affordable Care Act; HHS Notice of Benefit and Payment Parameters for 2017 [2017 Payment Notice]," Final Rule, 81 Federal Register 12203, March 8, 2016. See pages 12293-12295.HHS, "Patient Protection and Affordable Care Act; HHS Notice of Benefit and Payment Parameters for 2018; Amendments to Special Enrollment Periods and the Consumer Operated and Oriented Plan Program [2018 Payment Notice]," Final Rule, 81 Federal Register 94058, December 22, 2016. See pages 94138-94139.HHS, "Patient Protection and Affordable Care Act; HHS Notice of Benefit and Payment Parameters for 2019 [2019 Payment Notice]," Final Rule, 83 Federal Register 16930, April 17, 2018. See pages 17006-17007.
Notes: PY = plan year. FFE = federally-facilitated exchange. SBE = state-based exchange. SBE-FP = state-based exchange using the federal information technology (IT) platform. See "Types of Exchanges" in this report for a description of exchange types. n/a = Although some SBE-FPs existed prior to plan year 2017, HHS did not begin assessing a user fee on issuers in those states until then.SBEs' assessment of user fees, if any, varies, as discussed in this section of the report.
Further Reading
For more information about certain issues addressed in or relevant to this report, see the following CRS reports:
- CRS Report R45146, Federal Requirements on Private Health Insurance Plans
- CRS Report R44425, Health Insurance Premium Tax Credits and Cost-Sharing Subsidies
- CRS Report R44438, The Individual Mandate for Health Insurance Coverage: In Brief
Appendix A.
Exchange Types by State
|
State |
Individual Exchange |
SHOP Exchange |
Are the State's Individual and SHOP Exchanges the Same Type? |
|
Alabama |
FFE |
FF-SHOP |
Yes |
|
Alaska |
FFE |
FF-SHOP |
Yes |
|
Arizona |
FFE |
FF-SHOP |
Yes |
|
Arkansas |
SBE-FP |
|
No |
|
California |
SBE |
SB-SHOP |
Yes |
|
Colorado |
SBE |
|
Yes |
|
Connecticut |
SBE |
SB-SHOP |
Yes |
|
Delaware |
|
FF-SHOP |
Yes |
|
District of Columbia |
SBE |
SB-SHOP |
Yes |
|
Florida |
FFE |
FF-SHOP |
Yes |
|
Georgia |
FFE |
FF-SHOP |
Yes |
|
Hawaii |
FFE |
|
No |
|
Idaho |
SBE |
|
Yes |
|
Illinois |
|
FF-SHOP |
Yes |
|
Indiana |
FFE |
FF-SHOP |
Yes |
|
Iowa |
|
FF-SHOP |
Yes |
|
Kansas |
FFE |
FF-SHOP |
Yes |
|
Kentucky |
SBE-FP |
SB-FP-SHOP |
Yes |
|
Louisiana |
FFE |
FF-SHOP |
Yes |
|
Maine |
FFE |
FF-SHOP |
Yes |
|
Maryland |
SBE |
SB-SHOP |
Yes |
|
Massachusetts |
SBE |
SB-SHOP |
Yes |
|
Michigan |
|
FF-SHOP |
Yes |
|
Minnesota |
SBE |
|
Yes |
|
Mississippi |
FFE |
SB-SHOP |
No |
|
Missouri |
FFE |
FF-SHOP |
Yes |
|
Montana |
FFE |
FF-SHOP |
Yes |
|
Nebraska |
FFE |
FF-SHOP |
Yes |
|
Nevada |
|
SB-FP-SHOP |
Yes |
|
New Hampshire |
|
FF-SHOP |
Yes |
|
New Jersey |
FFE |
FF-SHOP |
Yes |
|
New Mexico |
SBE-FP |
SB-SHOP |
No |
|
New York |
SBE |
|
Yes |
|
North Carolina |
FFE |
FF-SHOP |
Yes |
|
North Dakota |
FFE |
FF-SHOP |
Yes |
|
Ohio |
FFE |
FF-SHOP |
Yes |
|
Oklahoma |
FFE |
FF-SHOP |
Yes |
|
Oregon |
SBE-FP |
|
No |
|
Pennsylvania |
FFE |
FF-SHOP |
Yes |
|
Rhode Island |
SBE |
SB-SHOP |
Yes |
|
South Carolina |
FFE |
FF-SHOP |
Yes |
|
South Dakota |
FFE |
FF-SHOP |
Yes |
|
Tennessee |
FFE |
FF-SHOP |
Yes |
|
Texas |
FFE |
FF-SHOP |
Yes |
|
Utah |
FFE |
|
Yes |
|
Vermont |
SBE |
|
Yes |
|
Virginia |
FFE |
FF-SHOP |
Yes |
|
Washington |
SBE |
|
Yes |
|
West Virginia |
|
FF-SHOP |
Yes |
|
Wisconsin |
FFE |
FF-SHOP |
Yes |
|
Wyoming |
FFE |
FF-SHOP |
Yes |
|
TOTAL: 51 |
FFE: 34 SBE: 12 SBE-FP: 5 |
FF-SHOP: 32 SB-SHOP: 16 SB-FP-SHOP: 2 No SHOP: 1 |
Yes: 46 No: 5 |
Sources: Congressional Research Service (CRS) illustration based on data from the following sources: Individual exchange types: Centers for Medicare & Medicaid Services (CMS), "2018 Marketplace Open Enrollment Period Public Use Files: 2018 OEP State-Level Public Use File," April 18, 2018, at https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Marketplace-Products/Downloads/2018_OE_State.zip. SHOP exchange types: Kaiser Family Foundation, "State Health Insurance Marketplace Types, 2018," at https://www.kff.org/health-reform/state-indicator/state-health-insurance-marketplace-types/; verified at Healthcare.gov at health-insurance-marketplace-types/, and at state exchange websites as needed.
b. 2021 SHOP exchange types: HealthCare.gov, “Select your state,” at https://www.healthcare.gov/smal -
https://www.healthcare.gov/small-businesses/employers/.
Notes: SHOP = Small business health options program. FFE and FF-SHOP = Federally facilitated individual exchange; federally facilitated SHOP exchange. SBE and SB-SHOP = State-based individual exchange; state-based SHOP exchange. SBE-FP and SB-FP-SHOP = State-based individual exchange using the federal information technology (IT) platform; state-based SHOP exchange using the federal IT platform. Counts of "states" include the District of Columbia. In the individual exchanges, "plan year" is generally that calendar year, but group coverage plan years, including in the SHOP exchanges, may start at any time during a calendar year. See "Types of Exchanges" in this report for discussion of the different exchanges. See Figure 1in this report for the exchange types by state in map form.
a. In these SB-SHOP states, the SHOP web portal is using or transitioning to a direct enrollment approach: it does not offer online enrollment but instead instructs users to connect with agents or brokers offering plans through the state's SHOP exchange, or outside of it if there are no plans offered in the state's SHOP exchange. Idaho, Oregon, and Vermont have only or primarily used a direct enrollment approach. New York and Connecticut do not appear to have an online enrollment portal but do allow small businesses to compare plans online and either mail in an enrollment form or enroll with an agent or broker. The SHOP webpages of Arkansas, Minnesota, and Washington report that because no issuers have offered SHOP plans in 2018, they will transition current SHOP plan holders to direct relationships with agents or brokers to discuss renewal in off-exchange coverage. Contact report author for sources.
b. In many FFE states, the federal government performs all employers/, cross-referenced at state exchange websites or otherwise as needed. Kentucky and Nevada both had SB-FP-SHOPs, but according to communication with CMS, their SHOP types are now as shown in the table. States with no medical plans available in their SHOP exchanges are indicated. In states that do have plans available in their SHOP exchanges, there may or may not be plans available in al areas.
c. All FF-SHOPs are now using a direct enrollment approach only. They do not offer online
enrol ment but instead instruct users to connect with agents or brokers offering plans through the state’s SHOP exchange. See “Online Enrol ment versus Direct Enrol ment” in this report for more information.
d. No insurers are currently offering medical plans in these FF-SHOPs. (Some may be offering dental
plans, however.) See CMS, Health Insurance Exchange Public Use Files, 2021: Business Rules PUF, at https://www.cms.gov/CCIIO/Resources/Data-Resources/ma rketplace-puf. Contact report author for further information.
e. While most states have maintained the same type of individual exchange they initial y opted for, some have
transitioned to different exchange types, or are planning to do so. For transitions to date 2014 exchange types: https://aspe.hhs.gov/pdf-report/addendum-health-insurance-marketplace-summary-enrol ment-report 2015 exchange types: FN 3 of https://www.cms.gov/newsroom/fact-sheets/march-31-2015-effectuated-enrol ment-snapshot 2016 exchange types: FN 3 of https://www.cms.gov/newsroom/fact-sheets/march-31-2016-effectuated-enrol ment-snapshot 2017-2020 exchange types: State level public use files for each year, https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Marketplace-Products. 2021 and future transitions: See table note (a) regarding 2021 exchange types. Two CMS resources also note PY2020 and PY2021 transitions, as referenced where relevant by state below: “CMS PY2021 QHP report” (CMS, CCIIO, Plan Year 2021 Qualified Health Plan Choice and Premiums in HealthCare.gov States, October 2020, at https://www.cms.gov/CCIIO/Resources/Data-Resources/QHP-Choice-Premiums); and “2020 CMS Navigator Recipients” (CMS, 2020 CMS Navigator Cooperative Agreement Recipients, August 30, 2020, at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/assistance). Kentucky: https://kentucky.gov/Pages/Activity-stream.aspx?n=GovernorBeshear&prId=218 Maine: https://www.maine.gov/dhhs/blog/maine-progresses-toward-state-based-health-insurance-marketplace-2020-08-06. Also see 2020 CMS Navigator Recipients. New Jersey: https://nj.gov/governor/news/news/562019/approved/20190322a.shtml. Also see CMS PY2021 QHP report. New Mexico: https://www.bewel nm.com/Special-Enrol ment-(1)/partner-resources/State-Based-Exchange-Transition. Oregon: https://healthcare.oregon.gov/marketplace/gov/Pages/tech-consumer-assistance.aspx. Pennsylvania: https://www.insurance.pa.gov/Coverage/Pages/State-Based-Exchange.aspx. Also see CMS PY2021 QHP report. Virginia: https://www.governor.virginia.gov/newsroom/all-releases/2020/august/headline-860017-en.html. Also see 2020 CMS Navigator Recipients. Also see Sabrina Corlette et al., States Seek Greater Control, Cost-Savings by Converting to State-Based Marketplaces, Robert Wood Johnson Foundation, October 2019, at https://www.rwjf.org/en/library/research/2019/10/states-seek-greater-control-cost-savings-by-converting-to-state-based-marketplaces.html.
Congressional Research Service
33
link to page 23 link to page 23 Overview of Health Insurance Exchanges
f.
No insurers are currently offering medical plans in these SB-SHOPs. (Some may be offering dental plans, however.) The SHOP website suggests that smal businesses contact agents, brokers, and/or insurers directly to learn about coverage options outside of the SHOP. See Arkansas: https://myarinsurance.com/pages/manage-shop/ Minnesota: https://www.mnsure.org/employer-employees/index.jsp Nevada: https://www.nevadahealthlink.com/overview/ Pennsylvania: Confirmed via state officials Washington: Confirmed via state officials
g. For the purposes of SHOP exchange participation, states may define smal employers (or smal businesses) as
employers that have not more than 50 or not more than 100 employees. See SHOP “Eligibility and Enrol ment” in this report. Only four states use the threshold of 100. See California: https://www.coveredca.com/forsmal business/eligible/ Colorado: https://connectforhealthco.com/get-started/options-for-smal -business-owners/, “Employer application” New York: https://nystateofhealth.ny.gov/employer Vermont: https://info.healthconnect.vermont.gov/smal business_faq
h. These SB-SHOPs are using a direct enrollment approach only: They do not offer online
enrol ment but instead instruct users to connect with agents or brokers offering plans through the state’s SHOP exchange. See Colorado: https://connectforhealthco.com/get-started/options-for-smal -business-owners/ Idaho: https://www.yourhealthidaho.org/smal -business-insurance/ Maryland: https://mhcsmal biz.marylandhealthconnection.gov/anonymous-web/#/quote-engine/enrol New York: https://nystateofhealth.ny.gov/employer Oregon: https://healthcare.oregon.gov/marketplace/employers/Pages/employers.aspx Vermont: https://info.healthconnect.vermont.gov/SB
i.
In some FFE states, the federal government performs al functions. But in these FFE states, the state partners with the federal government to perform some functions. CMS data do not identify these "partnership"general y identify these “partnership” variations, but the Kaiser Family Family Foundation tracks them at the site linked in table note (a).
j.
Georgia received approval through the Section 1332 state innovation waiver process to shift to its own “Georgia Access Model,” essential y a direct enrol ment approach, beginning in PY2023. This 1332 process al ows states to waive specified ACA provisions, including provisions related to the establishment of health insurance exchanges and related activities. See CRS Report R44760, State Innovation Foundation tracks them at the site linked above.
c. Hawaii received an ACA Section 1332 waiver allowing it not to operate a SHOP exchange. See State of Hawaii, Department of Labor and Industrial Relations, "ACA Small-Business Health Options Program (SHOP)—Waiver Approved on 12/30/2016," at http://labor.hawaii.gov/aca-smallbiz/. For more information on Section 1332 waivers, see CRS Report R44760, State Innovation Waivers: Frequently Asked Questions for background on 1332 waivers and for more information about Georgia’s waiver.
k. Hawai received a Section 1332 waiver exempting it from having SHOP exchange for PYs 2017-2021. This
was related to the state’s pre-existing program and requirements related to employment-based coverage. See the report cited in table note (j) for more information about Hawai ’s waiver.
Congressional Research Service
34
link to page 10 link to page 40 link to page 40 link to page 40 Overview of Health Insurance Exchanges
Appendix B. Types of Plans Offered Through the Exchanges In general, health insurance plans offered through exchanges must be qualified health plans (QHPs).130 See “Qualified Health Plans” in this report for requirements QHPs must meet to be
sold in the exchanges.
A QHP is the only type of comprehensive health plan an exchange may offer, but QHPs may be
offered outside of exchanges, as wel . Besides standard QHPs, there may be other types of plans available in a given exchange, including child-only plans, catastrophic plans, consumer operated and oriented plans (CO-OPs), and multi-state plans (MSPs). Technical y, these are al also QHPs.
Stand-alone dental plans (SADPs) are the only non-QHPs offered in the exchanges.
Table B-1. Types of Plans Offered Through the Exchanges
Can Be
PTC and
Offered
CSR
Outside
Summary
Eligible?
Exchanges?
Qualified
A plan that is offered by a state-licensed insurerAsked Questions.
d. However, Nevada appears to be transitioning from an SBE-FP to an SBE. See National Association for State Health Policy, "Nevada's Insurance Exchange Director Talks about Transitioning to a State-Based Marketplace and Saving Millions," April 24, 2018, at https://nashp.org/nevadas-insurance-exchange-director-heather-korbulic-talks-about-transitioning-to-a-state-based-marketplace/.
e. Effective 2018, Utah has transitioned from an SB-SHOP to an FF-SHOP. See Utah Governor's Office of Economic Development, Avenue H Health Insurance Exchange, "Small Businesses," at https://avenueh.com/businesses, accessed June 1, 2018.
Appendix B.
Types of Plans Offered Through the Exchanges
|
Summary |
Can Use Premium Tax Credits or Cost-Sharing Reductions? |
Can Be Offered Outside Exchanges? |
||
|
Qualified Health Plan (QHP) |
|
Yes |
Yes |
|
|
QHP Variations |
||||
|
Child-Only Health Insurance Plan |
A plan in which only individuals under the age of 21 may |
Yes |
Yes |
|
|
Catastrophic Plan |
Catastrophic
A plan that provides |
No |
Yes |
|
|
Consumer Operated and Oriented Plan (CO-OP) |
|
Yes |
Yes |
|
|
Multi-state Plan (MSP) |
, as amended) program. b
(CO-OP)
Multi-state
A plan sold in the exchanges under contract with the federal
Yes
No
Plan (MSP)
Office of Personnel Management (OPM).c
Non-QHPs
Dental-Only
|
Yes |
No |
|
|
Non-QHPs |
||||
|
Dental-Only Plan |
Coverage for dental care. May be offered either |
Yes, in certain circumstances. |
Yes |
|
Sources: CRS analysis of statute and regulation. QHP definition: 42 U.S.C. §18021. Child-only and catastrophic plans: 42 U.S.C. §18022. CO-OPs: 42 U.S.C. §18021 and 42 U.S.C. §18042. MSPs: 42 U.S.C. §18021 and 42 U.S.C. §18054. Dental-only plans: 42 U.S.C. §18031(d)(2)(B)(iii ), 45 C.F.R. §155.1065, and 45 C.F.R. §155.705. Premium tax credits and cost-sharing reductions: 26 U.S.C. §36B(c)(3)(A) and 42 U.S.C. §18071(f)(1).
Notes:
a.
130 42 U.S.C. §18031(d)(2)(B).
Congressional Research Service
35
Overview of Health Insurance Exchanges
Notes: PTC = premium tax credit. CSR = cost-sharing reduction. a. Catastrophic plans are available only to individuals under the age of 30 and individuals who obtain hardship
or affordability exemptions from the ACA'’s individual mandate to maintain minimum essential coveragecovera ge or pay a penalty. See CRS Report R44438, The Individual Mandate for Health Insurance Coverage: In Brief.
b.
b. The HHS Secretary is required to use funds appropriated to the CO-OP program to finance start-up and
solvency loans for eligible nonprofit organizations applying to become a CO-OP. The majority of products offered by a CO-OP must be QHPs sold in the non-group and smallsmal -group markets, including through exchanges. CMS initial y awarded loans to 24 CO-OPs, but one of those 24 was dropped from the program prior to offering health plans. See CRS Report R44414, Consumer Operated and Oriented Plan (CO-OP) Program: Frequently Asked Questions. Among the remaining 23 CO-OPs, it appears that 3 remain operational—meaning they are currently offering health plans and there is no indication that they wil stop doing so in the future. The other 20 CO-OPs offered health plans at one time but have shut down or are in various stages of shutting down. See Maine: Community Health Options: https://www.healthoptions.org/ Idaho, Montana, and Wyoming: Mountain Health CO-OP: https://www.mountainhealth.coop/ Wisconsin: Common Ground Healthcare Cooperative: https://www.commongroundhealthcare.org
c. The ACA directs OPM to contract with private insurers in each state to offer at least two QHPs under the
MSP program. The term multi-state plan is meant to indicate that this program extends across the states, not that the plans themselves are necessarily interstate. There are not currently any multi-state plans available.
Congressional Research Service
36
link to page 42 link to page 43 link to page 43 link to page 30 Overview of Health Insurance Exchanges
Appendix C. Exchange Spending and Funding Details from CMS Budget Justifications The Centers for Medicare & Medicaid Services (CMS) in the U.S. Department of Health and Human Services (HHS) is the federal agency responsible for administering the health insurance
exchanges. In support of the President’s annual proposed budget, CMS, like other agencies, produces a performance budget, also cal ed a budget justification. Actual spending for the proposed budget year depends on the availability of appropriations, among other factors. However, the narratives and tables in each year’s budget document are also useful in
understanding prior-year spending.
Provisions in annual appropriations acts require CMS to provide, in its budget justification for each fiscal year, “cost information” that “details the uses of al funds used by the Centers for Medicare & Medicaid Services specifical y for Health Insurance Exchanges for each fiscal year
since the enactment of the ACA and the proposed uses for such funds [for the upcoming fiscal year]” for the categories shown in Figure C-1.131 Each budget justification also includes narrative
information about federal spending in each of the categories listed in the table.
The exchanges are largely funded by user fees assessed on the insurers who offer plans in FFE and SBE-FP exchanges. In addition to these user fees, funding comes from discretionary appropriations to the CMS Program Management account, risk-adjustment user fees, and appropriations to the Health Care Fraud and Abuse Control account, among other sources. Table
C-1 displays federal exchange spending according to these funding sources.
See “Exchange” in this report for more information. Find current and prior-year CMS budget justifications at CMS, “Performance and Budget,” at https://www.cms.gov/About-CMS/Agency-
Information/PerformanceBudget.
131 See, for example, the Further Consolidated Appropriations Act, 2020 (P.L. 116-94), Division A, T itle II, Sec. 220 and the Consolidated Appropriations Act, 2021 (P.L. 116-260), Division H, T itle II, Sec. 220.
Congressional Research Service
37
Figure C-1. Centers for Medicare & Medicaid Services “Health Insurance Exchanges Transparency Table,” FY2021
($ in thousands)
Source: Department of Health and Human Services, Centers for Medicare & Medicaid Services, Justification of Estimates for Appropriations Committees, Fiscal Year 2021, March 3, 2020, at https://www.cms.gov/About-CMS/Agency-Information/PerformanceBudget/FY2021-CJ-Final.pdf. See “Health Insurance Exchanges Transparency Table,” page 241. Discussion of spending categories is at “Federal Exchanges” table and narrative, page 195-200. Notes: FY = fiscal year.
CRS-38
link to page 43 link to page 43 link to page 43 link to page 43 link to page 43 link to page 43 link to page 43 Overview of Health Insurance Exchanges
Table C-1. CMS Federal Exchange Funding Sources for Specified Fiscal Years
($ in thousands)
FY2021
President’s
FY2021
Budget +/-
FY2018
FY2019
FY2020
President’s
FY 2020
Treasury Accounta
Actual
Finalb
Enactedb
Budgetc
Enacted
Program Management
$1,944,190
$1,636,111
$1,720,937
$1,171,728
($549,209)
Discretionary Appropriation
$618,164
$263,895
$296,533
$0
($296,533)
Program Operations (non-add)
$580,886
$229,384
$268,937
$0
($286,937)
Federal Administration (non-add)
$37,278
$34,511
$27,596
$0
($27,596)
Offsetting Col ections
$1,304,280
$1,351,893
$1,399,404
$1,171,728
($227,676)
Federal y-facilitated Exchange User
$1,272,168
$1,304,458
$1,341,039
$1,120,199
($220,840)
Fee (non-add)d
Risk Adjustment User Fee (non-add)
$32,112
$47,435
$58,365
$51,530
($6,836)
Other
$21,746
$20,323
$25,000
$0
($25,000)
Health Care Fraud and Abuse Control
$4,629
$19,256
$63,918
$25,384
($38,534)
Discretionary Appropriation
$0
$19,256
$63,918
$25,384
($38,534)
Mandatory Appropriatione
$4,629
n/a
n/a
n/a
n/a
Total, Program Level
$1,948,818
$1,655,367
$1,784,855
$1,197,112
($587,743)
Exchange User Fee Amounts as a Percentage of Program Level
65.3%
78.8%
75.1%
93.6%
n/a
Funding Sourcesf
Sources: Unless otherwise specified, data are compiled by CRS from the fol owing sources. Comparable data not found in prior years’ budget justifications. FY2019-FY2021 columns in table: Department of Health and Human Services, Centers for Medicare & Medicaid Services, Justification of Estimates for Appropriations Committees, Fiscal Year 2021, March 3, 2020, at https://www.cms.gov/About-CMS/Agency-Information/PerformanceBudget/FY2021-CJ-Final.pdf. “Federal Exchanges” table, page 195. FY2018 column in table: HHS, CMS, Justification of Estimates for Appropriations Committees, Fiscal Year 2020, March 13, 2019, at https://www.cms.gov/files/document/fy2020-cms-congressional-justification-estimates-appropriations-committees.pdf. “Federal Exchanges” table, page 178. Notes: FY = fiscal year. a. See source documents for description of Treasury Account categories. b. The FY2019 Final and FY2020 Enacted amounts were estimates as of January 2020. c. The FY2021 President’s budget amounts were the Administration’s proposals for FY2021. d. Per communication with CMS, this row is inclusive of both FFE and SBE-FP federal user fees. e. Health Care Fraud and Abuse Control (HCFAC) “Mandatory Appropriation” was listed in the FY2020 table
that included the FY2018 amounts, but not in the FY2021 table that included the other amounts. The FY2020 table also showed $5,000 in this row for “FY2019 Enacted,” but the FY2021 table did not show any such amounts for “FY2019 Final.” Per the FY2020 table, “HCFAC mandatory Wedge funding is subject to an annual al ocation process by the Attorney General and Secretary of Health and Human Services.”
f.
Calculated by CRS.
Congressional Research Service
39
link to page 45 Overview of Health Insurance Exchanges
Appendix D. Additional Resources
HHS “Notice of Benefits and Payment Parameters” (Payment Notices), Final Rule by Year The “Notice of Benefits and Payment Parameters,” also cal ed the “Payment Notice,” is a rule
published annual y by the Department of Health and Human Services (HHS). It addresses the exchanges and certain other private health insurance topics. It includes annual updates, such as changes to insurer user fee amounts, and policy changes, such as modified eligibility
requirements for the Navigator program.
The rule is titled according to the upcoming plan year that it addresses. For example, the 2021 Payment Notice was finalized in May 2020, with changes applicable to the 2021 plan year (which
is general y the calendar year).
Table D-1. HHS “Notice of Benefits and Payment Parameters,” Final Rule by Year
For Plan
Publication
Year
Title and Link
Citation
Date
2022
Patient Protection and Affordable Care Act; HHS Notice 86 Federal
January 19,
of Benefit and Payment Parameters for 2022; Updates to
Register 6138
2021
State Innovation Waiver (Section 1332 Waiver) Implementing Regulations a https://www.federalregister.gov/documents/2021/01/19/2021-01175/patient-protection-and-affordable-care-act-hhs-notice-of-benefit-and-payment-parameters-for-2022
2021
Patient Protection and Affordable Care Act; HHS Notice 85 Federal
May 14, 2020
of Benefit and Payment Parameters for 2021; Notice
Register 29164
Requirement for Non-Federal Governmental Plans https://www.federalregister.gov/documents/2020/05/14/2020-10045/patient-protection-and-affordable-care-act-hhs-notice-of-benefit-and-payment-parameters-for-2021
2020
Patient Protection and Affordable Care Act; HHS Notice 84 Federal
April 25, 2019
of Benefit and Payment Parameters for 2020
Register 17454
https://www.federalregister.gov/documents/2019/04/25/2019-08017/patient-protection-and-affordable-care-act-hhs-notice-of-benefit-and-payment-parameters-for-2020
2019
Patient Protection and Affordable Care Act; HHS Notice 83 Federal
April 17, 2018
of Benefit and Payment Parameters for 2019
Register 16930
https://www.federalregister.gov/documents/2018/04/17/2018-07355/patient-protection-and-affordable-care-act-hhs-notice-of-benefit-and-payment-parameters-for-2019
2018
Patient Protection and Affordable Care Act; HHS Notice 81 Federal
December 22,
of Benefit and Payment Parameters for 2018,
Register 94058
2016
Amendments exchanges.
c. The ACA directs OPM to contract with private issuers in each state to offer at least two QHPs under the MSP program. The term multi-state plan is meant to indicate that this program extends across the states, not that the plans themselves are necessarily interstate.
Author Contact Information
Footnotes
| 1. |
In this report, the terms consumers and individuals generally are used interchangeably, as are small businesses and small employers. |
| 2. |
The term individual exchange is used for purposes of this report. It is not defined in exchange-related statute or regulations. |
| 3. |
The individual, or non-group, market refers to insurance policies offered to individuals and families buying insurance on their own (i.e., not through an employer or other plan sponsor). |
| 4. |
Small businesses and the small-group market are defined later in this report, in "SHOP Exchanges." |
| 5. |
In tallies throughout this report, the District of Columbia (DC) is counted as a state. |
| 6. |
|
| 7. |
As of April 2018, states can no longer select the state-based using the federal IT platform (SB-FP-SHOP) approach, except that the two such current states may maintain the model. See "Changes in SHOP Exchange Web Portal Functionality" in this report for more information. |
| 8. |
Hawaii received a Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) Section 1332 waiver exempting it from operating a small business health options program (SHOP) exchange. See "Changes in SHOP Exchange Web Portal Functionality" in this report for more information. |
| 9. |
42 U.S.C. §18031(b)(1)(A). |
| 10. |
State residency may be established through a variety of means, including actual or planned residence in a state, actual or planned employment in a state, and other circumstances. See 45 C.F.R. §155.305. |
| 11. |
U.S. citizens and U.S. nationals are eligible for coverage through the exchanges. "Lawfully present" immigrants are also eligible for coverage through the exchanges. Examples of "lawfully present" immigrants include those who have "qualified non-citizen" immigration status without a waiting period, humanitarian statuses or circumstances, valid non-immigrant visas, and legal status conferred by other laws. See 45 C.F.R. §155.305 and Healthcare.gov, "Coverage for Lawfully Present Immigrants," at https://www.healthcare.gov/immigrants/lawfully-present-immigrants/. |
| 12. |
45 C.F.R. §155.410. |
| 13. |
The CMS "2018 Marketplace Open Enrollment Period Public Use Files" include a list of state-based exchange open enrollment periods that extended beyond the standard period. See https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Marketplace-Products/2018_Open_Enrollment.html. |
| 14. |
45 C.F.R. §155.420. |
| 15. |
Qualifying coverage generally means the types of minimum essential coverage (MEC) that are identified in the Internal Revenue Code (IRC) Section 5000A and its implementing regulations. Most types of comprehensive coverage are considered MEC, including public coverage (e.g., Medicaid, Medicare), as well as private insurance (e.g., employer-sponsored insurance and non-group insurance). For other types of coverage losses that can trigger a special enrollment period (SEP), see 45 C.F.R. §155.420. |
| 16. |
For example, in 2014, the Department of Health and Human Services (HHS) established an SEP due to technical problems submitting insurance applications through the federal information technology platform (i.e., HealthCare.gov). In 2015, HHS established an SEP around tax season for individuals who had not enrolled in 2015 coverage and were subject to the 2014 individual mandate penalty. For 2018 coverage, HHS established an SEP for consumers in states that were affected by the 2017 hurricanes or other severe weather events. See, for example, Healthcare.gov, "Special Enrollment Periods for Complex Issues," at https://www.healthcare.gov/sep-list/. |
| 17. |
For more information about consumer financial assistance, including applicable eligibility criteria and illustrative examples, see CRS Report R44425, Health Insurance Premium Tax Credits and Cost-Sharing Subsidies. |
| 18. |
Certain large employers could be subject to penalties if they do not offer minimum essential coverage (discussed at footnote 15) to full-time employees and their dependents. For more information, see CRS Report R43981, The Affordable Care Act's (ACA) Employer Shared Responsibility Determination and the Potential Employer Penalty. |
| 19. |
Cost sharing is the share of costs an insured individual pays for services out of pocket. The term often includes deductibles, coinsurance, and co-payments. A deductible is the amount an insured individual pays before his or her health insurance plan begins to pay for most services. Coinsurance is the share of costs, figured in percentage form, an insured individual pays for a health service. A co-payment is a fixed amount an insured individual pays for a health service. An out-of-pocket limit or maximum means that once a consumer has paid that amount in a policy year, the issuer will pay 100% of covered costs for the remainder of the policy year. |
| 20. |
The ACA requires the HHS Secretary to provide full reimbursements to issuers that provide these cost-sharing subsidies to their enrollees. However, the ACA did not appropriate funds for such payments. In October 2017, the Trump Administration halted these payments, effective immediately, until Congress appropriates funds. Issuers still must provide the subsidies to eligible consumers, but issuers are not reimbursed. See HHS, "Payments to Issuers for Cost-Sharing Reductions," October 12, 2017, at https://www.hhs.gov/sites/default/files/csr-payment-memo.pdf. |
| 21. |
HHS, "Patient Protection and Affordable Care Act; HHS Notice of Benefit and Payment Parameters for 2019 [2019 Payment Notice]," Final Rule, 83 Federal Register 16930, April 17, 2018. This rule set the cost-sharing limits for 2019 and also references the 2018 limits. |
| 22. |
The annual out-of-pocket limits and the actuarial value requirements that apply to all plans are discussed again in the section on "Qualified Health Plans." |
| 23. |
Small employer and large employer are defined at 45 C.F.R. §144.103. States' definitions of small vs. large employers apply to their small-group market operating outside of SHOP exchanges as well, and they determine the relevance of any federal requirements that apply differently to small and large employers (e.g., large group plans are not subject to the requirement to cover the essential health benefits). See CRS Report R45146, Federal Requirements on Private Health Insurance Plans. |
| 24. |
California, Colorado, New York, and Vermont are the only states that define small businesses as having 100 or fewer employees for the purpose of participation in the SHOP exchanges. See National Conference of State Legislatures, "Small and Large Business Health Insurance: State & Federal Roles," updated July 15, 2017, at http://www.ncsl.org/research/health/small-business-health-insurance.aspx. Verified by CRS report author on the SHOP website of each SB-SHOP on April 2, 2018. Contact report author for all sources. |
| 25. |
42 U.S.C. §18032(f)(2)(B). No states have allowed large employers (as defined by the state) use of their SHOP exchanges. See footnote 24 for the four states that allow participation by small employers with up to 100, instead of up to 50, eligible employees. |
| 26. |
The definition of full-time employee is at 45 C.F.R. §155.20. |
| 27. |
|
| 28. |
45 C.F.R. §155.705(b)(2). |
| 29. |
HHS, "Patient Protection and Affordable Care Act; HHS Notice of Benefit and Payment Parameters for 2017 [2017 Payment Notice]," Final Rule, 81 Federal Register 12203, March 8, 2016, page 12206, codified at 45 C.F.R. §155.705. Also see CMS, CCIIO, "Small Business Health Options Program (SHOP)," at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Health-Insurance-Marketplaces/2017-Implementation-of-Vertical-Choice.html. |
| 30. |
For the iterations of guidance mentioned in this paragraph, see CMS, CCIIO, "Extension of State-Based SHOP Direct Enrollment Transition," April 18, 2016, at https://www.cms.gov/CCIIO/Resources/Regulations-and-Guidance/Downloads/1332-and-SHOP-Guidance-508-FINAL.PDF. |
| 31. |
For more information about ACA Section 1332 waivers, see CRS Report R44760, State Innovation Waivers: Frequently Asked Questions. |
| 32. |
|
| 33. |
See 2019 Payment Notice (cited at footnote 21), pages 16996-16997. This policy change was previewed in a May 2017 agency announcement and in the November 2017 Payment Notice proposed rule, and the changes were allowed to go into effect prior to the finalization of the rule. |
| 34. |
|
| 35. |
Healthcare.gov, "What's New in SHOP for 2018," at https://www.healthcare.gov/small-businesses/provide-shop-coverage/whats-new-2018-shop/. |
| 36. |
It is possible for SHOP exchanges to establish minimum participation rates and minimum contribution rates. Businesses that do not comply with established rates cannot be prohibited from obtaining coverage through SHOP exchanges; rather, health insurance plans may limit the availability of coverage for any employer that does not meet an allowed minimum participation or contribution rate to an annual enrollment period—November 15 through December 15 of each year. |
| 37. |
This estimate excludes Hawaii, as Hawaii's SHOP exchange was no longer operational in 2017 due to the state's receipt of a 1332 waiver. See CMS, CCIIO, "SHOP Marketplace Enrollment as of January 2017," May 15, 2017, at https://www.cms.gov/CCIIO/Resources/Data-Resources/Downloads/SHOP-Marketplace-Enrollment-Data.pdf. |
| 38. |
|
| 39. |
See 26 U.S.C. §45R for small business eligibility and credit amount details described in this section. |
| 40. |
Internal Revenue Service, Rev. Proc. 2018-18, Section 3.09, at https://www.irs.gov/irb/2018-10_IRB#RP-2018-18, referring to 26 U.S.C. §45R(d)(3)(B). |
| 41. |
26 U.S.C. § 45R(d)(1)(B). |
| 42. |
For example, see 42 U.S.C. §18031(i), 45 C.F.R. §155.205, 45 C.F.R. §155.210, and 45 C.F.R. §155.225. |
| 43. |
Ibid. Specifically, for the requirement to implement Navigator programs, see 45 C.F.R. §155.210. For the requirement to implement certified application counselor programs, see 45 C.F.R. §155.225. The 2019 Payment Notice (cited at footnote 21, see page 16979) changed some Navigator program requirements. Exchanges previously were required to establish (i.e., grant) at least two Navigator entities, one of which had to be a community- and consumer-focused nonprofit group and the other from one of the categories listed at 45 C.F.R. §155.210. Going forward, exchanges are required to establish only one Navigator entity, and the entity does not need to be a community- and consumer-focused nonprofit group; it can be any of the entity types listed at 45 C.F.R. §155.210. In addition, the 2019 Payment Notice removed the requirement that all Navigator entities maintain a physical presence in their exchange service area. Certified application counselor programs were not addressed in the 2019 Payment Notice. |
| 44. |
45 C.F.R. §155.215. |
| 45. |
45 C.F.R. §155.220. |
| 46. |
45 C.F.R. §155.205. |
| 47. |
Ibid. |
| 48. |
42 U.S.C. §18031(d)(4). |
| 49. |
42 U.S.C. §18031(c)(1); 42 U.S.C. §18031(e). For more information, see, for example, CMS, CCIIO, "Addendum to 2018 Letter to Issuers in the Federally-Facilitated Marketplaces," February 17, 2017, at https://www.cms.gov/CCIIO/Resources/Regulations-and-Guidance/Downloads/Final-2018-Letter-to-Issuers-in-the-Federally-facilitated-Marketplaces-and-February-17-Addendum.pdf. |
| 50. |
42 U.S.C. §18031(d)(2)(B). |
| 51. |
42 U.S.C. §18021(a)(1). For more information about the essential health benefits (EHB), see CRS Report R44163, The Patient Protection and Affordable Care Act's Essential Health Benefits (EHB). |
| 52. |
42 U.S.C. §18022. Note that the EHB cost-sharing limits and generosity requirements are referenced briefly in this report as the annual out-of-pocket limits and actuarial-value requirements that apply to all plans in the exchanges. Some consumers are eligible for further cost-sharing assistance, which builds on these provisions. See "Premium Tax Credits and Cost-Sharing Reductions" in this report. |
| 53. |
For more information about federal requirements that apply to QHPs and plans offered outside of exchanges, see CRS Report R45146, Federal Requirements on Private Health Insurance Plans. |
| 54. |
42 U.S.C. §18031(a). |
| 55. |
42 U.S.C. §18031(d)(5)(A). |
| 56. |
CMS, Fiscal Year 2018 Justification of Estimates for Appropriations Committees, May 23, 2017, at https://www.cms.gov/About-CMS/Agency-Information/PerformanceBudget/Downloads/FY2018-CJ-Final.pdf. |
| 57. |
Erin Mershon, "State Health Exchanges Wrestle with Budgets," Roll Call, July 25, 2016, at http://www.rollcall.com/news/policy/state-health-exchanges-wrestle-budgets. |
| 58. |
U.S. Government Accountability Office, Health Insurance Marketplaces: CMS Needs to Improve Its Oversight of State IT Systems' Sustainability and Performance, GAO-17-258, August 15, 2017. Also see Justin Giovannelli and Ken Lucia, "The Experiences of State-Run Insurance Marketplaces That Use HealthCare.gov," The Commonwealth Fund, September 2015, at http://www.commonwealthfund.org/~/media/files/publications/issue-brief/2015/sep/1840_giovannelli_experiences_states_use_healthcaregov_rb_v2.pdf. |