IHS Overview
The Indian Health Service (IHS) within the Department of Health and Human Services (HHS) is the lead federal agency charged with improving the health of American Indians and Alaska Natives. IHS provides health care for approximately 2.2 million eligible American Indians/Alaska Natives through a system of programs and facilities located on or near Indian reservations, and through contractors in certain urban areas.1 IHS provides services to members of 573 federally recognized tribes.2 It provides services either directly or through facilities and programs operated by Indian tribes or tribal organizations through self-determination contracts and self-governance compacts authorized in the Indian Self-Determination and Education Assistance Act (ISDEAA).3
The Snyder Act of 19214 provides general statutory authority for IHS.5 In addition, specific IHS programs are authorized by two acts: the Indian Sanitation Facilities Act of 19596 and the Indian Health Care Improvement Act (IHCIA).7 The Indian Sanitation Facilities Act authorizes the IHS to construct sanitation facilities for Indian communities and homes. IHCIA authorizes programs such as urban health, health professions recruitment, and substance abuse and mental health treatment, and permits IHS to receive reimbursements from Medicare, Medicaid, the State Children's Health Insurance Program (CHIP), the Department of Veterans Affairs (VA), and third-party insurers. Finally, the Public Health Service Act provides funds for the Special Diabetes Program for Indians grants administered by IHS.
Funding Sources
The IHS has three major sources of funding, described here in order of magnitude: (1) discretionary appropriations, (2) collections, and (3) mandatory appropriations. Unlike most agencies within HHS, which receive their appropriations through the Labor, Health and Human Services, and Education appropriations act, the IHS receives its discretionary appropriations through the Interior/Environment appropriations act.8 IHS's discretionary appropriations are divided into three accounts: (1) Indian Health Services, (2) Contract Support Costs, and (3) Indian Health Facilities.
As a second source of funding, IHS collects and expends funds received as payment for health services provided. IHS has the authority to receive payments from other federal programs such as Medicaid, Medicare, CHIP, and the Department of Veterans Affairs. IHS also receives payments from state programs (such as workers compensation) and from private insurance. IHS, under its IHCIA collection authority, is able to retain these payments to increase services available to its beneficiaries. In addition to these collections, IHS collects rent from facilities it owns.
The third and smallest source of IHS funding is a mandatory appropriation of $150 million annually to support the Special Diabetes Program for Indians.9 This mandatory funding was extended through FY2019 in the Bipartisan Budget Act of 2018 (BBA 2018, P.L. 115-123). The President's budget request proposes to shift the FY2019 appropriation to discretionary funding.10
FY2019 Budget Request and Funding History
Table 1 presents IHS's funding from FY2014 through the proposed President's FY2019 budget submission. The table generally shows increases in both appropriated funds and funds collected by IHS through FY2018. The table presents IHS's three budget accounts—Indian Health Services, Contract Support Costs, and Indian Health Facilities—and the funds collected and allocated to programs under these accounts. Collections and proposed and actual mandatory funding are subtracted from program-level funding to show the agency's discretionary budget authority. Although appropriations for IHS have increased over time, the FY2018 appropriation represents a larger increase than in prior years. In particular, the FY2018 appropriation included increases for a number of programs funded under the Indian Health Facilities account, which includes maintenance and improvement and construction of new facilities. In addition, the FY2018 appropriation increased funding for mental health and alcohol and substance abuse services, provided new funding for the Indian Health Care Improvement Fund, and included language to require IHS to conduct an analysis of IHS locations and services relative to the IHS user population.
The FY2019 President's request represents a decrease from FY2018 levels for a number of IHS programs and activities. However, final FY2018 appropriations had not been enacted during the period in which the FY2019 President's request was being formulated. While the total request for IHS represents a decrease from FY2018-enacted levels, it represents an increase from FY2017-enacted levels and the FY2018 annualized continuing resolution levels that were in place at the time the FY2018 request levels were being determined.
|
Program or Activity |
2014 |
2015 |
2016 |
2017 |
2018 |
FY2019 Request |
|
Indian Health Services Account |
4,714a |
4,820a |
4,909 |
5,035 |
5,295 |
5,290 |
|
Clinical and Preventive Services |
4,566 |
4,652 |
4,737 |
4,860 |
5,117 |
5,122 |
|
Clinical Services |
4,271 |
4,348 |
4,431 |
4,553 |
4,796 |
4,883 |
|
Hospitals and Health Clinics |
1,791 |
1,837 |
1,857 |
1,935 |
2,045 |
2,190 |
|
Purchased/ Referred Careb |
879 |
914 |
914 |
929 |
963 |
955 |
|
Collections |
1,172 |
1,151 |
1,194 |
1,194 |
1,194c |
1,194c |
|
Mental Health/Alcohol and Substance Abuse |
264 |
272 |
287 |
312 |
328 |
340 |
|
Indian Health Care Improvement Fund |
— |
— |
— |
— |
72 |
— |
|
Dental Services |
165 |
174 |
178 |
183 |
195 |
204 |
|
Preventive Health |
148 |
154 |
156 |
160 |
170 |
89 |
|
Special Diabetes Program for Indians |
147d |
150 |
150 |
147d |
150 |
150 |
|
Other Health Services |
148 |
168 |
171 |
175 |
178 |
168 |
|
Urban Health Projects |
41 |
44 |
44 |
48 |
49 |
46 |
|
Indian Health Professions |
33 |
48 |
48 |
49 |
49 |
43 |
|
Tribal Management/Self-Governance |
6 |
8 |
8 |
8 |
8 |
5e |
|
Direct Operations |
68 |
68 |
72 |
70 |
72 |
73 |
|
Contract Support Costs Accountf |
587 |
663 |
718 |
718 |
718 |
822 |
|
Indian Health Facilities Account |
460 |
469 |
532 |
554 |
876 |
515 |
|
Maintenance and Improvement |
62 |
62 |
82 |
84 |
176 |
84 |
|
Rental of Staff Quartersg |
8 |
8 |
9 |
9 |
9 |
9 |
|
Sanitation Facilities Construction |
79 |
79 |
99 |
102 |
192 |
102 |
|
Health Care Facilities Construction |
85 |
85 |
105 |
118 |
243 |
80 |
|
Facilities/Environmental Health Support |
211 |
220 |
223 |
227 |
241 |
229 |
|
Medical Equipment |
23 |
23 |
23 |
23 |
24 |
20 |
|
Total, Program Level |
5,761 |
5,951 |
6,160 |
6,307 |
6,889 |
6,627 |
|
Less Funds from Other Sources |
||||||
|
Collections |
1,172 |
1,151 |
1,194 |
1,194 |
1,194 |
1,194 |
|
Rental of Staff Quarters |
8 |
8 |
9 |
9 |
9 |
9 |
|
Special Diabetes Program for Indiansb |
147 |
150 |
150 |
147 |
150 |
—h |
|
Total, Discretionary Budget Authority |
4,435 |
4,642 |
4,808 |
4,957 |
5,536 |
5,424 |
Sources: Funding amounts are from HHS Budget documents available at https://www.ihs.gov/budgetformulation/congressionaljustifications/. Amounts for FY2014-FY2015 and FY2019 request are from IHS's congressional justifications. FY2016 and FY2017 are from IHS's operating plan for FY2017, available at https://www.ihs.gov/budgetformulation/includes/themes/newihstheme/display_objects/documents/FY2017-IHS-Operating-Plan.pdf. FY2018 discretionary amounts are from joint explanatory statement accompanying the Consolidated Appropriations Act, 2018 (P.L. 115-141) (Congressional Record, March 22, 2018, https://www.congress.gov/crec/2018/03/22/CREC-2018-03-22-bk2.pdf) and Special Diabetes Program for Indians amounts are from CRS's analysis of BBA 2018 (P.L. 115-123).
Notes: Individual amounts may not add to subtotals or totals due to rounding.
a. In FY2014 and FY2015, Contract Support Costs were included in the Indian Health Services account.
b. This was previously referred to as "Contract Health Services."
c. Estimated amount of collections included in the FY2019 budget justification.
d. PHSA Section 330C provides an annual appropriation of $150 million for this program; this amount was reduced in FY2013, FY2014, and FY2017 by 2% because of budget sequestration. See CRS Report R42050, Budget "Sequestration" and Selected Program Exemptions and Special Rules.
e. The FY2019 budget does not request funds for Tribal Management Grants.
f. Beginning in FY2016, Contract Support Costs were funded as an indefinite discretionary appropriation.
g. For information on IHS collections, see IHS budget requests, available at https://www.ihs.gov/budgetformulation/congressionaljustifications.
h. The President's FY2019 budget requests that the Special Diabetes Program for Indians be funded from the discretionary appropriation. See Letter from Mick Mulvaney, Director Office of Management and Budget, to The Honorable Paul D. Ryan, Speaker of the House of Representatives, February 12, 2018, https://www.whitehouse.gov/wp-content/uploads/2018/02/Addendum-to-the-FY-2019-Budget.pdf.
IHS Third-Party Collections
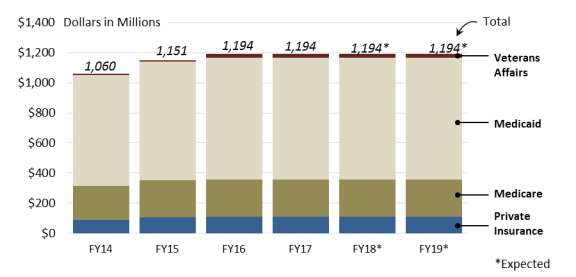
IHS facilities collect payments from third-party payors for services provided to IHS beneficiaries who are also enrolled in other programs. These collections are an important source of IHS's clinical services (see Table 1). Medicaid is the largest source of IHS's collections—accounting for approximately 68% of all third-party collections in FY2017, the most recent year of final data available—followed by Medicare (21% in FY2017) and private insurance (9% in FY2017). Beginning in FY2014, IHS began receiving payments from the VA for services provided to IHS beneficiaries who were also enrolled in the VA (these payments were 2% of all of IHS's third-party collections in FY2017).
|
Figure 1. IHS Reimbursements, by Source: FY2015-FY2017 (Actual) and FY2018-FY2019 (Expected) |
 |
|
Sources: Figure created by CRS. Funding amounts are from FY2015-FY2019. HHS Budget documents available at https://www.ihs.gov/budgetformulation/congressionaljustifications/. |