The U.S. Army Corps of Engineers (USACE) provides engineering services and capabilities in support of national interests. As part of its overall mission, USACE prepares for and responds to national emergencies in support of the Department of Defense and other federal agencies and efforts. In response to the Coronavirus Disease 2019 (COVID-19) pandemic emergency, the Federal Emergency Management Agency (FEMA) had assigned USACE missions totaling $1.8 billion as of mid-May 2020, which have led to USACE
- assessing over 1,000 sites for potential use as alternate care sites (ACSs, also called alternate care facilities) that can function as temporary health care facilities;
- developing standardized designs for ACSs (with other federal agencies' input); and
- contracting to convert structures into ACSs.
Congressional oversight of the COVID-19 response may include ACSs. Some USACE-converted ACSs reportedly are expected to close shortly after their conversions or are to be put on standby (referred to as warm sites). Others have served fewer patients than the facilities' capacity, but there is some reporting that health care professionals have found that ACSs provided relief for hospitals and their staff.
Legislation also may address ACS topics, such as changes to the nonfederal cost share for many ACS activities, which is typically 25% under the Stafford Act's requirement for public assistance. For example, H.R. 6800 would make the costs 100% federal for Stafford Act Public Assistance provided under the President's COVID-19 emergency declaration.
USACE Role in Alternate Care Sites
Conversion of Structures into ACSs
Federal involvement in an ACS begins with a state, local, tribal, or territorial authority's request to the President (typically through FEMA). FEMA may task USACE to participate in some, but not all, aspects of an ACS. USACE may assess structures for potential use as ACSs. USACE also may be responsible for converting structures into ACSs. USACE contracts with private companies to perform the conversions. USACE's standard designs are tailored to the specific structure and to the specific health care demand the site is intended to address (acute, hospital, or non-acute care and COVID-19 or non-COVID-19 patients).
For most USACE-led conversions, the requesting authority is responsible for providing any additional equipment and for supplying, operating, and staffing the ACS. Once the ACS conversion is complete, USACE's role ends, and the requesting authority becomes responsible for operating the ACS, including when to close the ACS. The federal government can supply and staff a specific type of ACS, called a Federal Medical Station (FMS), if a state, local, tribal, or territorial authority requests and is approved for such a facility. An FMS, such as occurred for the Javits Center in New York, can be supplied from the Strategic National Stockpile and staffed through the federal government.
Some governors have acted independently, using USACE's site assessments and designs but contracting directly for ACS conversions.
USACE Conversions
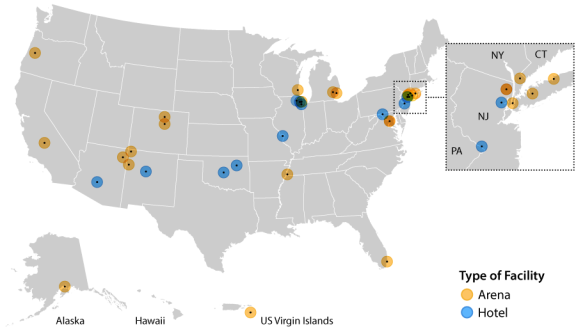
Figure 1 shows the locations of USACE-converted ACSs and whether the ACSs are for large, open spaces (arena conversions) or structures such as hotels or dormitories with closed rooms (hotel conversions).
|
Figure 1. USACE Contracts for Converting Structures into Alternate Care Sites
|
 |
|
Source: CRS, using USACE data for contracts as of May 4, 2020.
Notes: Arena = conversion of arena or convention center; Hotel = conversion of hotel or dormitory. District of Columbia and Paramus, NJ, each had two contracts; these appear darker in the figure due to overlap. USACE also developed a closed hospital conversion design. Nonfederal-led ACS conversions are not shown.
|
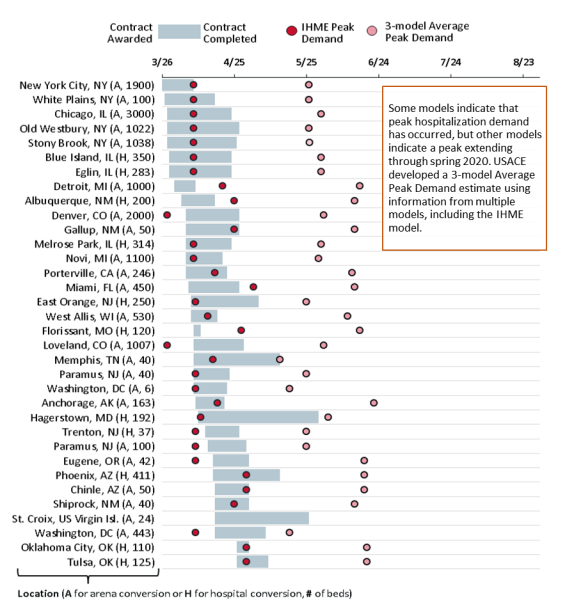
Figure 2 shows the contract duration for USACE conversions. Contract initiation depends on various factors, including when the request was made and approved and the length of the contract award process. According to government contracting data, USACE has used various contracting mechanisms for ACS assignments. For example, it awarded some contracts using full and open competition, whereas others were not competed due to the urgency for the ACS.
To put the ACS contracts in the context of local COVID-19 conditions, Figure 2 shows two USACE-provided dates estimating peak hospitalization demand: a statistically estimated date from the IHME hospitalization model and a USACE-calculated estimated date based on the average of three hospitalization models (including the IHME hospitalization model). Variations in peak demand estimates are due to underlying differences in the characteristics and assumptions inherent in each model. Some models (e.g., IHME's model) indicate that peak hospitalization demand may have occurred. The USACE "3-model average peak demand" produces estimates of peak hospitalization demand extending through late spring.
|
Figure 2. Dates for USACE Contracts for Alternate Care Site Conversions
and USACE Data on Estimated Dates of Local Peak Hospitalization Demand
|
 |
|
Source: CRS, using data posted by USACE on May 4, 2020, at https://www.usace.army.mil/Coronavirus/.
Notes: Completion dates beyond May 4, 2020, are tentative. IHME Peak Demand estimate is based on USACE's data for Institute for Health Metrics and Evaluation's (IHME's) Peak Hospitalization Model. Data for the 3-model Average Peak Demand are a USACE calculation of the average peak date using IHME, COVID-19 Hospital Impact Model for Epidemics (CHIME), and Center for Army Analysis models. Not shown are hospitalization demand dates for U.S. Virgin Islands (due to an inability to verify USACE data) and nonfederal-led ACS conversions.
|
For various USACE conversions, the ACSs were reduced in size following the initial request. Other ACS projects are on hold. Table 1 shows the number of beds in ACSs provided through USACE conversion contracts.
Table 1. Beds in USACE-Converted Alternate Care Sites
Completed or Under Contract by State, Territory, and Tribe
|
|
Beds
|
|
Beds
|
|
Beds
|
|
New York
|
4,060
|
New Jersey
|
427
|
Missouri
|
120
|
|
Illinois
|
3,947
|
Arizona
|
411
|
Navajo Nation
|
50
|
|
Colorado
|
3,007
|
New Mexico
|
290
|
Oregon
|
42
|
|
Michigan
|
2,100
|
California
|
246
|
Tennessee
|
40
|
|
Wisconsin
|
530
|
Oklahoma
|
235
|
U.S. Virgin Islands
|
24
|
|
Florida
|
450
|
Maryland
|
192
|
|
|
|
District of Columbia
|
449
|
Alaska
|
163
|
TOTAL
|
16,783
|
President Trump lauded the USACE commander, Lieutenant General (LTG) Todd Semonite, for delivering on COVID-19 mission assignments despite the low use of some requested ACSs. LTG Semonite characterized ACSs as providing "insurance" in response to a dynamic situation. As the pandemic's effect on the health care system evolves, attention has shifted away from addressing hospital bed availability for patients.
Oversight topics may include