On January 7, 2020, the Department of Defense (DOD) reported that the Islamic Republic of Iran launched a number of ballistic missiles at certain Iraqi military bases hosting U.S. and coalition military forces. These forces utilize Iraqi military bases to support counter-terrorism operations within the region, including military actions against the Islamic State under Operation Inherent Resolve. DOD initially reported no U.S. or coalition casualties, then later stated that 34 U.S. servicemembers assigned to these locations were subsequently diagnosed with mild traumatic brain injury (mTBI) resulting from the missile blasts. On February 10, 2020, numerous media sources reported that DOD revised its count to 109 servicemembers diagnosed, with 76 of those members already having returned to duty. These numbers may increase in the future as servicemembers are further assessed.
This Insight provides a brief overview of DOD policies and programs to screen, assess, and manage mTBI, which includes deployment-related concussions.
What is Traumatic Brain Injury?
DOD defines TBI as a "traumatically induced structural injury or physiological disruption of brain function, as a result of an external force, that is indicated by new onset or worsening of at least one of the following clinical signs" immediately after an event:
- altered mental status;
- memory loss (before or after the injury); or
- decreased, or loss of, consciousness (self-reported or observed).
Examples of external forces include blunt trauma to the head, acceleration or deceleration movement to the head, or exposure to blasts or explosions, including penetrating injuries. DOD organizes TBI diagnoses into four levels of severity: mild, moderate, severe, and penetrating. An assessment conducted at the time of the injury or event determines the level of severity. Individuals with TBI can experience a wide variety of acute or chronic physical, cognitive, or emotional signs and symptoms.
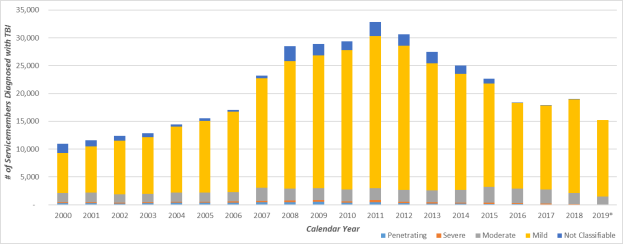
Since 2000, mTBI has been the most common type of TBI among servicemembers (see Figure 1). In 2018, DOD reported that 18,949 servicemembers were diagnosed with TBI. Of those, 88.7% (16,801) were mTBI.
|
Figure 1. Servicemembers Diagnosed with TBI
Calendar Year 2000-2019*
|
 |
|
Source: CRS graphic based on data compiled from the Defense and Veterans Brain Injury Center (DVBIC), "DoD Worldwide Numbers for TBI," accessed January 28, 2020.
Notes: Data represent the number of servicemembers diagnosed with TBI during that calendar year. For servicemembers with multiple TBI within a year, DVBIC only counts their most severe TBI category in this dataset. *Full-year data for 2019 are not yet available.
|
mTBI Screening and Assessment
Deployed servicemembers conducting military operations are generally at higher risk for mTBI than non-deployed servicemembers. As such, DOD conducts two types of screenings and assessments on deploying or deployed servicemembers: neurocognitive assessment and concussion evaluation.
Neurocognitive Assessment
Since 2008, Congress has required (10 U.S.C. §1074f note) DOD to conduct neurocognitive assessments on servicemembers before and after they deploy. DOD Instruction 6490.13 directs all deploying servicemembers to undergo a baseline neurocognitive assessment prior to departure. If a deployed servicemember is diagnosed with mTBI, reassessments are conducted after the injury and upon return from deployment. Medical providers typically compare assessment findings to inform return-to-duty decisions, or indications for follow-on evaluation and treatment.
Concussion Evaluation
DOD Instruction 6490.11 requires all servicemembers exposed to a potentially concussive event (PCE) (e.g., a ballistic missile impact blast), to be identified, tracked, and medically evaluated for mTBI. If exposed to a PCE, servicemembers undergo an "Injury/Evaluation/Distance (IED)" assessment to determine if further medical evaluation is necessary. Military commanders are required to place servicemembers exposed to a PCE on a 24-hour rest period, provide for a medical evaluation, and submit an incident report to the Joint Trauma Analysis and Prevention of Injury in Combat (JTAPIC). Depending on the servicemember's safety, location, and status of ongoing military operations, a commander can delay or postpone the rest period.
Management of mTBI
In general, DOD health care providers treat servicemembers with mTBI in accordance with the Department of Veterans Affairs (VA)/Department of Defense Clinical Practice Guideline for the Management of Concussion-Mild Traumatic Brain Injury. Servicemembers diagnosed with mTBI in a deployed setting may return to duty after completing the necessary evaluations, rest periods, and resolution of mTBI symptoms. The return to duty time varies for servicemembers based on the number of previous concussions they may have experienced:
- First concussion—no earlier than 24 hours after the event.
- Second concussion (within a 12-month period)—no earlier than seven days after symptoms have resolved.
- Third concussion (within a 12-month period)—delayed until a recurrent concussion evaluation is completed.
If there are sustained or worsening mTBI symptoms, servicemembers may be medically evacuated to an appropriate medical facility for follow-on care.
TBI Research Efforts
DOD funds and conducts numerous research efforts to prevent, mitigate, and treat the effects of TBI among servicemembers. Various military research entities administer such efforts, including the
DOD's TBI research programs often coordinate other departments participating in the Federal Interagency Traumatic Brain Injury Research Informatics System, as well as private and academic medical research organizations.
Congressional Interest
Over the past three decades, Congress has enacted numerous provisions to support DOD's TBI research and treatment efforts. In 1992, Congress appropriated $3.2 million in the DOD Appropriations Act to establish the DVBIC (previously referred to as the "Head and Neck Injury Initiative"). Since then, Congress has maintained its interest in DOD's TBI research and treatment efforts by enacting numerous provisions, typically within the annual defense appropriations bill or the National Defense Authorization Act (NDAA). Congress also continues to exercise close oversight of DOD's TBI efforts. In the FY2020 NDAA (P.L. 116-92) and accompanying conference and committee reports, several TBI-related reporting or briefing requirements are included:
- Report on TBI research activities specific to chronic traumatic encephalopathy.
- Briefing on the U.S. Army's efforts to mitigate TBI, including an overview of preventative devices.
- Report on evidence-based TBI mitigation efforts with the "best clinical effectiveness."