In accordance with 10 U.S.C. §115, Congress annually authorizes the end strength for active duty and reserve component personnel. End strength is the maximum number of personnel permitted in each military service (e.g., Army, Marine Corps, Navy, Air Force) as of September 30, the last day of the fiscal year. For fiscal year (FY) 2019, Congress authorized a total end strength of 1,338,100 active duty personnel and 824,700 reserve component personnel, including subtotals by force. Each military service then decides how to organize, train, and equip the people who compose its authorized end strength in order to meet combatant commander or service-specific requirements.
This decision includes determining the number of military medical personnel required in each service. The size of each service's medical force is often dependent on total end strength levels authorized by Congress, demands for medical capabilities in military operations, and the priority of those demands compared to other nonmedical capabilities. As major combat operations decreased over the past decade, DOD gradually reduced the active duty military medical end strength at an average annual rate of 1% (815 personnel). However, for FY2020, DOD proposes to reduce its active duty medical force by 13% (14,707 personnel).
Military Medical Force
DOD's total medical force includes military (active duty and reserve component), civil service, and contract personnel. Currently, the active duty medical force is comprised of 116,154 personnel from the Army, Navy, and Air Force–approximately 65% of the total medical force. This includes uniformed physicians, nurses, medics, and other health care professionals. Most of the active duty medical force (71%) is assigned to the Military Health System (MHS). The MHS provides health care worldwide to approximately 9.6 million beneficiaries (i.e., servicemembers, retirees, family members) in military hospitals and clinics and through civilian health care providers participating in TRICARE. The remaining active duty medical force (29%) is generally assigned to health service support positions in deployable or warfighting units, military service headquarters, or combatant commands.
DOD's Proposal to Reduce Military Medical End Strength
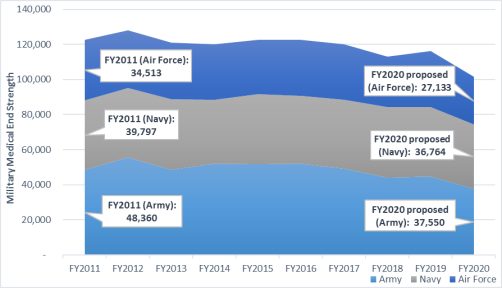
DOD's budget request for FY2020 proposes an overall active duty end strength of 1,339,500 personnel. If authorized by Congress, this would be a 0.1% increase from FY2019 end strength levels. Budget documents detailing this request indicate that DOD plans to reduce its active duty medical force by 13% (14,707 personnel) in order to "support the National Defense Strategy." Compared to FY2019 levels, the Army would have the largest reduction in medical forces (-16%), followed by the Air Force (-15%), and the Navy (-7%).
Table 1. Active Duty Medical Force, FY2019 vs. FY2020
|
|
FY2019 (estimated)
|
FY2020 (proposed)
|
Proposed Change (#)
|
Proposed Change (%)
|
|
Army
|
44,643
|
37,550
|
-7,093
|
-16%
|
|
Navy
|
39,600
|
36,764
|
-2,836
|
-7%
|
|
Air Force
|
31,911
|
27,133
|
-4,778
|
-15%
|
|
Total
|
116,154
|
101,447
|
-14,707
|
-13%
|
|
Figure 1. Active Duty Medical Force, FY2011-FY2020
|
 |
|
Source: Department of Defense (DOD), "Defense Health Program Fiscal Year (FY) 2020 Budget Estimates," March 2019; DOD, "Defense Health Program Fiscal Year (FY) 2019 Budget Estimates," February 2018; DOD, "Defense Health Program Fiscal Year (FY) 2018 Budget Estimates," May 2017; DOD, "Defense Health Program Fiscal Year (FY) 2017 Budget Estimates," February 2016; DOD, "Defense Health Program Fiscal Year (FY) 2016 Budget Estimates," February 2015; DOD, "Defense Health Program Fiscal Year (FY) 2015 Budget Estimates," March 2014; DOD, "Defense Health Program Fiscal Year (FY) 2014 Budget Estimates," April 2013; DOD, "Defense Health Program Fiscal Year (FY) 2013 Budget Estimates," February 2012; DOD, "Defense Health Program Fiscal Year (FY) 2012 Budget Estimates," February 2011.
Notes: Reserve component personnel are not reflected above.
|
The proposed reductions stem from several medical workforce assessments and reforms directed by the National Defense Authorization Act for FY2017 (P.L. 114-328). These mandates require DOD to
- establish and report to Congress a process to define military medical and dental personnel requirements (by position) necessary to meet "operational medical force readiness requirements;" (§721)
- convert certain military medical and dental positions to civilian medical and dental positions; (§721)
- develop measures to maintain critical wartime medical readiness skills; (§725)
- implement a "performance-based, strategic sourcing acquisition strategy for health care professional staff." (§727)
DOD's initial plan to implement these reductions include: (1) transferring positions (also known as billets) from the MHS to new health service support positions in deployable or warfighting units, military service headquarters, or combatant commands; (2) transferring billets from the MHS to the military departments for repurposing as nonmedical assets; and (3) converting certain military billets to civilian billets.
Considerations for Congress
In the coming months, Congress will consider the National Defense Authorization Act for FY2020 and annual defense appropriations. The following possible questions may be of interest to Members of Congress seeking further clarification on DOD's proposal to reduce its active duty medical force and conducting congressional oversight of the MHS.
Costs
- What are the estimated cost-savings and opportunity costs (e.g., increased private sector care costs, reduced military medical capabilities and surge capacity, narrowed recruitment and training pipelines) from reducing military medical personnel numbers over the fiscal year defense program (FYDP)?
- How might reductions in personnel affect costs for the TRICARE program?
Impact to Military Operations
- What are the benefits or risks to military operations posed by reducing the medical force?
- How might a smaller medical force affect military readiness?
Implementation
- How do the military services plan to implement a reduction of military medical personnel?
- How might reductions in military medical personnel affect access to health care by servicemembers, family members, or retirees?
Recruitment and Retention
- How might proposed changes impact recruitment and retention of military medical personnel, particularly those with critically short wartime skills?
- Are current recruitment and retention tools (e.g., special pays, accession/retention bonuses, graduate medical education opportunities) adequate to meet military medical end strength requirements?