On August 1, 2018, the World Health Organization (WHO) reported that a new Ebola outbreak was detected in the eastern part of the Democratic Republic of Congo (DRC), about one week after having declared that a separate outbreak had ended in the western part of the country. This new outbreak is occurring in North Kivu, a province experiencing its own humanitarian crisis with over 1 million displaced people. WHO will shift staff that had just completed working to contain the previous outbreak in the Equateur province to North Kivu. Health experts have reportedly determined that the strain in North Kivu is the same one for which a vaccine is available and has been used to control past Ebola outbreaks, though ongoing conflict in the province may complicate control efforts. As of August 2, press reports indicate that 20 people, including two health workers, died after showing symptoms of hemorrhagic fever. Four of six samples collected tested positive for Ebola.
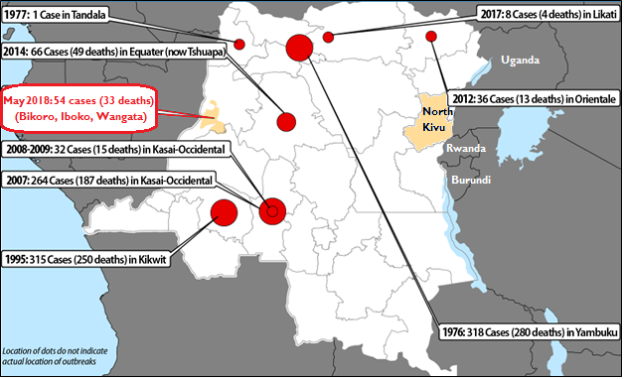
About one week ago on July 24, 2018, WHO reported that an Ebola outbreak in the DRC had ended after having infected 54 people, 33 of whom died. The outbreak began on May 8, 2018, when DRC health officials reported to WHO that two Ebola cases had been detected in the Equateur province, a rural area in the northwestern portion of the country. The disease later spread to Mbandaka, a city that holds 1.2 million people and serves as a regional trade hub. This was the ninth Ebola outbreak in DRC since the disease was discovered in 1976, when an outbreak infected 318 people and killed 280 (Figure 1).
In contrast to the 2014-2016 West Africa Ebola outbreak, the WHO response was swift. On the same day that the outbreak was reported, WHO released $2 million from its Contingency Fund for Emergencies (CFE), deployed a team to the region, and activated an emergency incident management system. WHO also issued a $57 million appeal to control the outbreak. The international community exceeded the request, having provided $63 million. The largest contributions were provided by Germany (€5 million), United Kingdom (£5 million), and the United States ($5.3 million). Other types of support included in-kind contributions for medical evacuations and intercountry air transport from Norway and the European Union, respectively; technical assistance from Germany, Guinea, the United Kingdom, and the United States; and the provision of vaccines to protect over 3,300 people.
|
Figure 1. Ebola Virus Outbreaks in the Democratic Republic of Congo: 1976-2018
|
 |
|
Source: Adjusted by CRS from World Health Organization, Ebola Outbreak Response in The Democratic Republic of The Congo, Briefing to Committee A at the World Health Assembly, Geneva, Switzerland, May 23, 2018.
Note: CRS adapted the graphic to include information on Ebola cases and deaths in May 2018 and to identify the location of North Kivu and its proximity to Uganda, Rwanda, and Burundi.
|
The DRC's Ministry of Health, WHO, and other stakeholders took several steps to contain the outbreak. Notably, a new vaccine, which was used for the first time in the field during the 2014-2016 West Africa Ebola outbreaks, was provided to all primary and secondary contacts to prevent disease transmission. Merck provided more than 7,500 doses for the vaccination effort. In addition, health officials approved the use of investigational drugs to treat those infected with Ebola. This marks the first time in which investigational drugs were used in the field during an outbreak.
Health experts were particularly troubled by this outbreak, because it occurred in a province that is densely populated (2.5 million people) and hosts a portion of the Congo River that is vital for regional transportation. Previous outbreaks occurred primarily in sparsely populated, rural areas. The only other urban outbreak occurred in Kikwit in 1995, which held 400,000 people at the time. WHO conducted operational readiness and preparedness assessments in the nine countries bordering the DRC and placed particular emphasis on the Central African Republic due to its proximity to the outbreak area. The assessment plans were aimed at identifying operational needs should the outbreak have spread to the country and providing technical support for the development and implementation of contingency plans.
U.S. Support
The United States committed to provide $8.0 million in support of Ebola control efforts in the country, drawing on $5.0 million in FY2017 appropriations for USAID-administered Global Health Program (GHP) funding and $3 million in GHP funds appropriated in FY2015 for Ebola response in West Africa. Roughly $5.0 million of the funds were provided to WHO for case management, entry screenings, diagnosis testing, and support for other laboratory functions. About $2.0 million was for the United Nations Children's Fund (UNICEF) to implement Ebola awareness communication campaigns and water, sanitation, and hygiene (WASH) projects. An estimated $700,000 was used by the International Federation of the Red Cross/Red Crescent Societies (IFRC) for promoting safe burial practices and Ebola prevention education campaigns. In addition, the U.S. Centers for Disease Control and Prevention (CDC) provided technical assistance for communications, logistics, operational and personnel support, laboratory capacity building, and the development and implementation of an outbreak response plan.
On June 5, the White House withdrew proposed rescissions of $252 million in unobligated emergency International Disaster Assistance (IDA) funds appropriated in 2015 to control the West Africa Ebola outbreak and bolster response capacity in affected countries. These funds may be made available for future Ebola control efforts.