Title X Program Administration and Grants
The federal government provides grants for family planning services through the Family Planning Program, Title X of the Public Health Service Act (42 U.S.C. §§300 to 300a-6). Enacted in 1970, Title X is the only domestic federal program devoted solely to family planning and related preventive health services. By law, Title X clients' participation in family planning services is voluntary.1
Although Title X is the only federal domestic program primarily focused on family planning, other programs also finance family planning, among their other services. These programs include Medicaid, the Health Center program under Section 330 of the Public Health Service Act, Maternal and Child Health Block Grants, Social Services Block Grants, and Temporary Assistance for Needy Families. In FY2015, Medicaid accounted for 75% of U.S. public family planning expenditures (including federal, state, and local government spending). In comparison, Title X accounted for 10%.2
Administration
Title X is administered by the Office of Population Affairs (OPA) under the Office of the Assistant Secretary for Health in the U.S. Department of Health and Human Services (HHS). Although the program is administered through OPA, funding for Title X activities is provided through in HHS's Health Resources and Services Administration (HRSA). Authorization of appropriations expired at the end of FY1985, but the program has continued to be funded through appropriations bills for the Departments of Labor, Health and Human Services, and Education, and Related Agencies (Labor-HHS-Education).
OPA administers three types of project grants under Title X: family planning services;3 family planning personnel training;4 and family planning service delivery improvement research.5
Family Planning Services Grants
Services
In FY2017, OPA used approximately 90% of Title X funds for clinical services.6 Family planning services grants fund family planning and related preventive health services, such as contraceptive services; natural family planning methods; infertility services; adolescent services; breast and cervical cancer screening and prevention; sexually transmitted disease (STD) and human immunodeficiency virus (HIV) prevention education, counseling, testing, and referral; preconception health services; and reproductive life plan counseling .7 These services must be provided "without coercion and with respect for the privacy, dignity, social, and religious beliefs of the individuals being served."8
OPA has increased efforts to integrate HIV-prevention services in family planning clinics.9 OPA provided supplemental grants to help Title X projects implement the Centers for Disease Control and Prevention's (CDC's) "Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health Care Settings."10
Although females make up the majority of Title X clients, services offered to males include condoms, education and counseling, STD testing and treatment, HIV testing, and, in some cases, vasectomy services.11
Client Charges
Priority for services is given to persons from low-income families, who may not be charged for care.12 Clients from families with income between 100% and 250% of the federal poverty guidelines are charged on a sliding scale based on their ability to pay. Clients from families with income higher than 250% of the federal poverty guidelines are charged fees designed to recover the reasonable cost of providing services. If a third party (such as a state Medicaid program or a private health insurance plan) is authorized or legally obligated to pay for a client's services, all reasonable efforts must be made to obtain the third-party payment without discounts.13
Client Characteristics
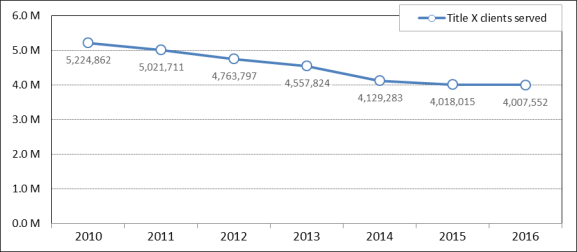
In 2016, Title X-funded clinics served 4.008 million clients, primarily low-income women and adolescents.14 Of those clients, 11% were male, 64% had incomes at or below the federal poverty guidelines, and 85% had incomes at or below 200% of the federal poverty guidelines.15 An earlier survey found that for 61% of clients, Title X clinics were their "usual" or only regular source of health care.16 In 2016, 43% of Title X clients were uninsured.17
The number of Title X clients served in 2016 was slightly lower than in 2015 (when there were 4.018 million clients). The 2016 client count was 23% lower than in 2010 (when there were 5.225 million clients).18 Figure 1 shows the number of Title X clients each year from 2010 to 2016.
|
Figure 1. Number of Title X Family Planning Clients Served, 2010-2016 |
 |
|
Source: Christina Fowler, Julia Gable, Jiantong Wang, and Beth Lasater, Family Planning Annual Report: 2016 National Summary, RTI International, Research Triangle Park, NC, August 2017, Exhibit A-2a, p. A-6, https://www.hhs.gov/opa/sites/default/files/title-x-fpar-2016-national.pdf. |
The Family Planning Annual Report and the HRSA FY2017 Budget Justification suggested several reasons for grantees' decreased capacity to serve clients,19 including
- clinic closures or clinics no longer participating in Title X;
- staffing shortages for family planning projects due to difficulties in provider recruitment and retention; and
- increased unit cost of providing services and upfront costs for infrastructure improvements (such as purchasing new health information technology and entering new contracts with insurers);
Grantees also suggested several potential reasons for a decrease in demand,20 including
- newly insured clients choosing to seek care from other non-Title X providers;
- increased use of long-acting reversible contraception (LARC), which could reduce the frequency of client visits in the long run, compared with some other types of contraception (such as oral contraceptives that require refills);21 and
- recent clinical guideline changes, such as pap tests are now recommended every three years instead of annually.22
Grantees and Clinics
In 2016, there were 91 Title X family planning services grantees. These grantees included 48 state, local, and territorial health departments and 43 nonprofit organizations, such as community health agencies, family planning councils, and Planned Parenthood affiliates.23
Title X grantees can provide family planning services directly or subaward Title X monies to other public or nonprofit entities to provide services. Although there is no fixed matching amount required for grants, regulations specify that no Title X projects may be fully supported by Title X funds.24 In 2016, Title X provided services through 3,898 clinics located in the 50 states, the District of Columbia, and the U.S. territories and Freely Associated States.25
Family Planning Training and Research Grants
Family planning training grants are used to train staff and improve the use and career development of paraprofessionals.26 Staff are trained through a Family Planning National Training Center and a National Clinical Training Center.27 These programs have produced provider education resources, training tools, podcasts, and webinars on topics such as the Zika virus, caring for women with opioid use disorders, mandated child abuse reporting, human trafficking, and clinical efficiency, among other topics.28 Family planning service delivery improvement research grants are used for studies to improve the service delivery of Title X projects.29
For more information on the Title X program, see https://www.hhs.gov/opa/title-x-family-planning.
Funding
Title X is a discretionary program, meaning its funding is provided in and controlled by annual appropriations acts. It has received appropriations every year since the program started in FY1971.
Annual appropriations acts have also specified certain program guidelines, such as requiring all Title X pregnancy counseling to be nondirective and prohibiting the use of Title X funds for abortion. This section describes recent funding amounts and proposals.30
FY2018 Funding
On March 23, 2018, the President signed the Consolidated Appropriations Act, 2018 (P.L. 115-141). P.L. 115-141 provides $286.479 million for Title X in FY2018, the same as the FY2017 enacted level.31 The FY2018 act continues previous years' requirements that Title X funds not be spent on abortions, among other requirements (see the text box below).
FY2018 appropriations are subject to a clause, known as the Weldon amendment, stating that "None of the funds made available in this Act may be made available to a Federal agency or program, or to a State or local government, if such agency, program, or government subjects any institutional or individual health care entity to discrimination on the basis that the health care entity does not provide, pay for, provide coverage of, or refer for abortions."32 Some groups have argued that the Weldon amendment conflicts with regulations that require Title X family planning services projects to give pregnant women the opportunity to receive information, counseling, and referral upon request for several options, including "pregnancy termination."33 In the February 23, 2011, Federal Register, HHS stated that potential conflicts would be handled on a case-by-case basis: "The approach of a case by case investigation and, if necessary, enforcement will best enable the Department to deal with any perceived conflicts within concrete situations."34
|
Requirements on the Use of Title X Funds in P.L. 115-141, P.L. 115-141 continues previous years' requirements regarding the use of Title X funds:
Sources: P.L. 115-141, Division H, Title II, and §207 and §208; Office of Management and Budget (OMB), The Budget of the U.S. Government, Fiscal Year 2019, Appendix, pp. 419, 483, https://www.whitehouse.gov/wp-content/uploads/2018/02/hhs-fy2019.pdf. |
FY2019 Budget Request
President Trump's FY2019 budget request, submitted February 12, 2018, includes $286.479 million for Title X, the same as the FY2017 enacted level.36 The FY2019 budget would continue previous years' provisions in appropriations laws prohibiting the use of Title X funds for abortion, among other requirements (see text box above).
According to the HRSA Justification of Estimates for Appropriations Committees, the proposed FY2019 funding level would support family planning services for 4 million clients, of which 90% would have family incomes at or below 200% of the federal poverty guidelines.37 The program's FY2019 goals include preventing 903,000 unintended pregnancies and reducing infertility by screening 1.2 million young women for chlamydia.38 The FY2018 target for cost per client served is $345.11, with the goal of maintaining the increase in cost per client below the medical care inflation rate.39 According to the Justification, the Title X program has encouraged clinics to improve financial sustainability by having more contracts with insurance plans and by recovering more costs through reimbursements and billing third-party payers.40 The Justification emphasizes that family planning projects should "optimally" have primary health services onsite or "in close proximity."41 The Justification also states that the program will likely continue addressing the Zika virus and other conditions affecting reproductive-age persons.42
The FY2019 budget states that it "includes provisions prohibiting certain abortion providers from receiving Federal funds from HHS, including those that receive funding under the Title X Family Planning program and Medicaid, among other HHS programs."43 One such provision would block HHS discretionary funds from being made available to a prohibited entity "either directly, through a State (including through managed care contracts with a State), or through any other means[.]" This prohibition would apply "[n]otwithstanding any other provision of law[.]" The provision defines prohibited entity as an entity, including its affiliates, subsidiaries, successors, and clinics, that meets the following criteria at the time of enactment:
(1) It is a nonprofit organization under Internal Revenue Code Section 501(c)(3);44
(2) It is an essential community provider primarily engaged in family planning services, reproductive health, and related medical care;45
(3) It performs, or provides any funds to any other entity that performs, abortions (other than in cases of rape, incest, and certain physician-certified cases in which the woman is in danger of death unless an abortion is performed);
(4) Total federal Title X grants to the entity (including affiliates, subsidiaries, or clinics) exceeded $23 million in FY2017.
The prohibited entity definition would no longer apply to an entity that certifies that it will no longer perform, nor fund any other entity that performs, an abortion (other than in cases of rape, incest, and when the woman is in danger of death unless an abortion is performed). The HHS Secretary would be required to seek repayment of any federal assistance if the certification's terms are violated.
The proposed provision does not mention Planned Parenthood Federation of America (PPFA). However, PPFA may meet the criteria for a prohibited entity.46 In March 2017, the New York Times reported that, in response to congressional proposals to restrict federal funds to PPFA, the White House informally proposed to preserve federal funding if PPFA stopped providing abortions. PPFA rejected that informal White House proposal.47
History of Funding
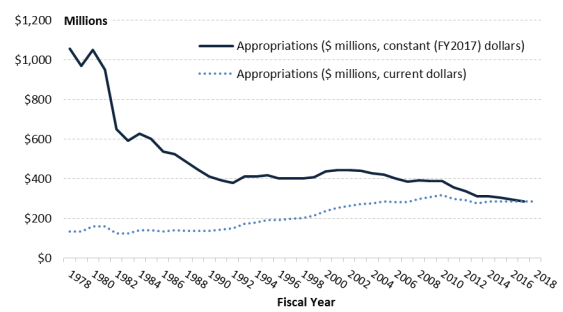
Table 1 shows Title X appropriations amounts since FY1971, when the program was created. Figure 2 shows Title X appropriations amounts since FY1978, in current dollars (not adjusted for inflation) and constant FY2017 dollars (adjusted for medical care inflation).
Table 1. Title X Family Planning Program Appropriations, FY1971-FY2018
(in millions, current dollars, not adjusted for inflation)
|
FY |
Appropriation |
FY |
Appropriation |
FY |
Appropriation |
|||||
|
|
|
1987 |
|
2003 |
$273.4 |
|||||
|
|
|
1988 |
|
2004 |
$278.3 |
|||||
|
|
|
1989 |
|
2005 |
$286.0 |
|||||
|
|
|
1990 |
|
2006 |
$282.9 |
|||||
|
|
|
1991 |
|
2007 |
$283.1 |
|||||
|
|
|
1992 |
|
2008 |
$300.0 |
|||||
|
|
|
1993 |
|
2009 |
$307.5 |
|||||
|
|
|
1994 |
|
2010 |
$317.5 |
|||||
|
|
|
1995 |
|
2011 |
$299.4 |
|||||
|
|
|
1996 |
|
2012 |
$293.9 |
|||||
|
|
|
1997 |
|
2013 |
$278.3 |
|||||
|
|
|
1998 |
|
2014 |
$286.5 |
|||||
|
|
|
1999 |
|
2015 |
$286.5 |
|||||
|
|
|
2000 |
|
2016 |
$286.5 |
|||||
|
|
|
2001 |
|
2017 |
$286.5 |
|||||
|
|
|
2002 |
|
2018 |
$286.5 |
Sources: For FY1971-FY2005, Department of Health and Human Services, Office of Population Affairs, Title X Funding History, https://www.hhs.gov/opa/title-x-family-planning/about-title-x-grants/funding-history/index.html; FY2006, Senate Appropriations Committee, S.Rept. 109-287, p. 325; FY2007, Consolidated Appropriations Act, 2008 Committee Print of the House Committee on Appropriations on H.R. 2764/P.L. 110-161, Division G, p. 1793, http://www.gpo.gov/fdsys/pkg/CPRT-110HPRT39564; FY2008-FY2009, "Explanatory Statement Submitted by Mr. Obey, Chairman of the House Committee on Appropriations, Regarding H.R. 1105, Omnibus Appropriations Act, 2009," Congressional Record, daily edition, vol. 155, no. 31 (February 23, 2009), p. H2378; FY2010, P.L. 111-117, 123 Stat. 3239; FY2011, P.L. 112-10, §1810 and §1119; FY2012, HHS, HRSA, Fiscal Year 2013 Justification of Estimates for Appropriations Committees, p. 347; FY2013, HHS, HRSA, Sequestration Operating Plan for FY2013, https://web.archive.org/web/20170429160747/https://www.hrsa.gov/about/budget/operatingplan2013.pdf; FY2014, P.L. 113-76, Division H, Title II; FY2015, P.L. 113-235, Division G, Title II; FY2016, P.L. 114-113, Division H, Title II; FY2017, P.L. 115-31, Division H, Title II; and FY2018, P.L. 115-141, Division H, Title II.
|
Figure 2. Title X Family Planning Program Appropriations, FY1978-FY2018 |
 |
|
Sources: Current dollars, see Table 1. Constant (FY2017) dollars, calculated by CRS using a fiscal year inflation adjustment based on monthly data for the Consumer Price Index All - Urban Consumers for Medical Care published by the Bureau of Labor Statistics, http://data.bls.gov/timeseries/CUUR0000SAM/. |
Institute of Medicine Evaluation
In 2009, at the request of OPA's Office of Family Planning, the Institute of Medicine (IOM, now the National Academy of Medicine) of the National Academy of Sciences independently evaluated the Title X program and made recommendations in A Review of the HHS Family Planning Program: Mission, Management, and Measurement of Results.48
IOM found that family planning—"helping people have children when they want to and avoid conception when they do not—is a critical social and public health goal" and that the "federal government has a responsibility to support the attainment of this goal." IOM argued, for example, that family planning can prevent unintended and high-risk pregnancies, thereby reducing fetal, infant, and maternal mortality and morbidity. IOM also stated that the appropriate use of contraception can reduce abortion rates and cited "ample evidence that family planning services are cost-effective."49 IOM made specific recommendations to increase program funding and improve program management, administration, and evaluation.
Among IOM's recommendations was that OPA's Office of Family Planning "review and update the Program Guidelines to ensure that they are evidence-based." IOM noted, for example, that the guidelines required female Title X clients, including adolescents, to have pelvic and breast examinations within six months of their initial visit, though "relevant abnormalities are rarely found in adolescents." At the time of the IOM report, Title X program guidelines had not been updated since 2001.50
In response to IOM's recommendations, OPA released new program guidelines in April 2014.51 The new guidelines draw on systematic literature reviews and existing recommendations from organizations, such as the CDC, the U.S. Preventive Services Task Force, the American College of Obstetricians and Gynecologists, the American Academy of Pediatrics, the American Society for Reproductive Medicine, and the American Urological Association. For example, the new guidelines state that pelvic exams and clinical breast exams are "not needed routinely to provide contraception safely to a healthy client" (though they may be recommended for some cases, such as inserting an intrauterine device, fitting a diaphragm, screening for cancer of nonadolescents, assessing gestational age after a positive pregnancy test, if the client has certain STD symptoms, as part of infertility care, or to address other noncontraceptive health needs). OPA stated that the new guidelines have "a foundation of empirical evidence and information supporting clinical practice."52 In addition, in response to the IOM report, HHS contracted with IOM to convene a standing committee to advise the Title X program on issues raised by the 2009 report, as well as other emerging family planning issues.53
FY2018 Funding Opportunity Announcement
The Title X funding opportunity announcement (FOA), which is released by OPA, lays out grant application requirements, program priorities, and other key issues. A significant delay in the FOA for FY2018 Title X Family Planning Services grants raised concern.54 Some current grantees feared services could be interrupted because of a potential lapse in grant funding.55 A press release accompanied the FOA: "Recognizing the announcement has been delayed, HHS is committed to ensuring that services continue unabated. Current grantees received notification today inviting them to submit a request for grant extension, so there is no gap in services."56
Key Differences Between the FY2017 and FY2018 FOAs
There are several differences between the FY2018 FOA and the FY2017 FOA that was posted under the previous Administration.57 Key differences are as follows:
The FY2018 FOA has a new requirement for clients under the age of consent. A client under the age of consent will be subject to a preliminary screening to rule out victimization after he or she presents with an STD, pregnancy, or any suspicion of abuse.58
The FY2018 FOA states that Title X projects should communicate the benefits of avoiding sexual risk, delaying sex, and returning to "sexually risk-free status," especially for adolescents.59 The FY2017 FOA did not use the phrase "sexually risk-free." The FY2017 FOA required projects to have written clinical protocols in accordance with "Providing Quality Family Planning Services: Recommendations of CDC and the U.S. Office of Population Affairs and Program Requirements for Title X Funded Family Planning Projects" (QFP).60 The QFP document states, "Providers should give comprehensive information to adolescent clients about how to prevent pregnancy. This information should clarify that avoiding sex (i.e., abstinence) is an effective way to prevent pregnancy and STDs."61
Both FOAs require that projects encourage family participation with respect to services to minors.62 But unlike the FY2017 FOA, the FY2018 FOA additionally states that this requirement applies to all clients, not just to minors.63 Under the FY2018 FOA, successful projects will use "counseling techniques that encourage family participation for all clients, including the involvement of parents, spouses or family where practicable."64
The FY2018 FOA emphasizes care coordination by noting that "each Title X project should ensure that family planning is contextualized within a holistic conversation of health, with the project optimally offering primary health services onsite, or having robust referral linkages to primary health providers in close proximity to the Title X site."65 The FY2017 FOA did not mention onsite or nearby primary care, but it did list among the program's priorities: "Addressing the comprehensive health care needs of clients through formal, robust linkages or integration with comprehensive primary care providers."66
Under the FY2017 FOA, final award selections were made by the applicable Public Health Service Region's regional health administrator (RHA), in consultation with the Deputy Assistant Secretary for Population Affairs (DASPA) and the Assistant Secretary for Health (ASH) or their designees.67 In contrast, under the FY2018 FOA, final award selections will be made by the DASPA or designee.68 This is a change from program practices in place since the 1980s. The IOM's 2009 report A Review of the HHS Family Planning Program stated that "Although the original language of the Title X statute provides decision-making authority to the DASPA, the Secretary of HHS transferred this authority from the DASPA to the RHAs in the 1980s. This transfer has helped maintain the integrity of the funding processes associated with the Title X program."69 The IOM report also stated that "the DASPA's status as a political appointee is one of the most significant issues affecting the Title X program."70
The FY2018 FOA encourages applications for "innovative" services and methods that have been "historically underrepresented" in the Title X program.71 The FY2017 FOA did not use those terms.
Finally, among the program's key issues, the FY2017 FOA explicitly mentioned access to "contraceptive options, including long acting reversible contraceptives (LARC), other pharmaceuticals, and laboratory tests, preferably on site" whereas the FY2018 FOA does not.72 A Questions and Answers document accompanying the FY2018 FOA does clarify that projects must provide contraception.73
Rule Nullification on Selecting Subrecipients
As mentioned, Title X grantees can provide family planning services directly or subaward Title X funds to other government or nonprofit entities (subrecipients) to provide services. In December 2016, OPA promulgated the final rule "Compliance With Title X Requirements by Project Recipients in Selecting Subrecipients."74 The rule became effective January 18, 2017, but P.L. 115-23 nullified the rule on April 13, 2017.75
The rule would have applied to grantees that make subawards; it would not have affected grantees that provide all their Title X services directly. It would have added language that "No recipient making subawards for the provision of services as part of its Title X project may prohibit an entity from participating for reasons other than its ability to provide Title X services" to Title X Family Planning Services grant program regulations.76
The President signed P.L. 115-23, "Providing for congressional disapproval under chapter 8 of title 5, United States Code, of the final rule submitted by Secretary of Health and Human Services relating to compliance with title X requirements by project recipients in selecting subrecipients." P.L. 115-23 nullified the rule under the Congressional Review Act.77 As a result, the rule "shall be treated as though such rule had never taken effect."78 That is, the rule is deemed not to have had any effect at any time. Furthermore, HHS is prohibited from reissuing the nullified rule in "substantially the same form" or issuing a "new rule that is substantially the same" as the nullified rule.79
In the December 2016 preamble accompanying the rule, OPA explained that some states had taken actions to limit Title X participation by certain types of providers.80 For example, some states enacted laws to prohibit state and local agencies from giving Title X subawards to abortion providers.81 Some other states had established a priority system for allocating Title X subawards, for example, by giving preference to state health departments, primary care providers, and community health centers over specialized family planning clinics.82 OPA argued that "these policies, and varying court decisions on their legality, have led to uncertainty among recipients, inconsistency in program administration, and reduced access to services for Title X priority populations."83
The rule would have limited the criteria a grantee could use to restrict entities from Title X subawards, disallowing "reasons other than [the entity's] ability to provide Title X services." The preamble explained that applicants for new and continuingTitle X grants would be required to describe their criteria for choosing subrecipients.84 The preamble stated that, under this rule, HHS would have reviewed these submissions for rule compliance and would have made "every effort to help entities come into compliance, and will award replacement grants to other providers when necessary to minimize any disruption of services."85
Supporters of the rule argued that it would have protected funding to specialized family planning providers, such as Planned Parenthood,86 and that it would have protected vulnerable individuals' access to family planning services.87 Critics of the rule argued that states should have the discretion to administer Title X funds consistently with state policy,88 and that the rule would have violated the conscience rights of voters and states that object to public funding of abortion providers.89
Abortion and Title X
The law prohibits the use of Title X funds in programs in which abortion is a method of family planning.90 On July 3, 2000, OPA released a final rule with respect to abortion services in family planning projects.91 The rule updated and revised regulations that had been promulgated in 1988.92 The major revision revoked the "gag rule," which restricted family planning grantees from providing abortion-related information. The regulation at 42 C.F.R. §59.5 had required, and continues to require, that abortion not be provided as a method of family planning. The July 3, 2000, rule amended the section to add the requirement that a project must give pregnant women the opportunity to receive information and counseling on prenatal care and delivery; infant care, foster care, or adoption; and pregnancy termination. If the woman requests such information and counseling, the project must give "neutral, factual information and nondirective counseling on each of the options, and referral upon request, except with respect to any option(s) about which the pregnant woman indicates she does not wish to receive such information and counseling."93
According to OPA, family planning projects that receive Title X funds are closely monitored to ensure that federal funds are used appropriately and that funds are not used for prohibited activities, such as abortion. The abortion prohibition does not apply to all Title X grantees' activities, but applies only to Title X projects' activities. The grantee's abortion activities must be "separate and distinct" from the Title X project activities.94 Safeguards to maintain this separation include (1) careful review of grant applications to ensure that the applicant understands the requirements and has the capacity to comply with all requirements; (2) independent financial audits to examine whether there is a system to account for program-funded activities and nonallowable program activities; (3) yearly comprehensive reviews of the grantees' financial status and budget report; and (4) periodic and comprehensive program reviews and site visits by OPA regional offices.95
It is unclear precisely how many Title X clinics also provide abortions through their non-Title X activities. In 2015, the Guttmacher Institute surveyed a nationally representative sample of publicly funded family planning clinics. Respondents included 535 clinics that received Title X funds. Based on that survey, an estimated 10% of clinics that received any Title X funding reported offering abortions separately from their Title X project.96
In 2004, following appropriations conference report directions, HHS surveyed its Title X grantees on whether their clinic sites also provided abortions with nonfederal funds.97 Grantees were informed that responses were voluntary and "without consequence, or threat of consequence, to non-responsiveness." The survey did not request any identifying information. HHS mailed surveys to 86 grantees and received 46 responses. Of these, 9 indicated that at least one of their clinic sites (17 clinic sites in all) also provided abortions with nonfederal funds, 34 indicated that none of their clinic sites provided abortions with nonfederal funds, and 3 responses had no numerical data or said the information was unknown.
Title X supporters argue that family planning reduces unintended pregnancies, thereby reducing abortion.98 HHS estimates that Title X services helped avert 901,838 unintended pregnancies in FY2016, and the Guttmacher Institute estimates that Title X services helped avert 822,300 unintended pregnancies in calendar year 2015.99 It is unclear exactly how many unintended pregnancies would have ended in abortion; however, the Guttmacher Institute estimates that in 2015, clinics receiving Title X funds helped avert 277,800 abortions, including 54,500 abortions among teens.100
In contrast, Title X critics argue that federal funds should be withheld from any organization, such as PPFA, that performs abortions. They argue that federal funding for nonabortion activities frees up Planned Parenthood's other resources for its abortion activities.101 Some critics also argue that if a family planning program is operated by an organization that also performs abortions, the implicit assumption and the message to clients is that abortion is a method of family planning.102
Teenage Pregnancy and Title X
In 2016, 18% of Title X clients were aged 19 or younger.103 Critics argue that by funding Title X, the federal government is implicitly sanctioning nonmarital sexual activity among teens. These critics argue that a reduced teenage pregnancy rate could be achieved if family planning programs emphasized efforts to convince teens to delay sexual activity, rather than efforts to decrease the percentage of sexually active teens who become pregnant.104 (See CRS Report RS20301, Teenage Pregnancy Prevention: Statistics and Programs.)
The program's supporters, in contrast, argue that the Title X program should be expanded to serve more people in order to reduce the rate of unintended pregnancies. The Guttmacher Institute estimates that in 2015, Title X family planning services helped avert an estimated 188,700 unintended teen pregnancies.105 The Guttmacher Institute estimates that without Title X clinics' services, the 2015 U.S. teen pregnancy rate would have been 44% higher.106 Supporters of expanding family planning services argue that the United States has a higher teen pregnancy rate than some countries (such as Sweden) where a similar percentage of teens are sexually active, in part because U.S. teens use contraception less consistently. Some also argue that recent declines in U.S. teen birth rates can be explained in part by changes in teen contraceptive use.107
Confidentiality for Minors and Title X
By law, Title X providers are required to "encourage" family participation when minors seek family planning services.108 However, confidentiality is required for personal information about Title X services provided to individuals, including adolescents.109 OPA instructs grantees on confidentiality for minors:
It continues to be the case that Title X projects may not require written consent of parents or guardians for the provision of services to minors. Nor can any Title X project staff notify a parent or guardian before or after a minor has requested and/or received Title X family planning services.110
The April 2014 Title X guidelines state,
Providers of family planning services should offer confidential services to adolescents and observe all relevant state laws and any legal obligations, such as notification or reporting of child abuse, child molestation, sexual abuse, rape, or incest, as well as human trafficking. Confidentiality is critical for adolescents and can greatly influence their willingness to access and use services. As a result, multiple professional medical associations have emphasized the importance of providing confidential services to adolescents.
Providers should encourage and promote communication between the adolescent and his or her parent(s) or guardian(s) about sexual and reproductive health. Adolescents who come to the service site alone should be encouraged to talk to their parents or guardians. Educational materials and programs can be provided to parents or guardians that help them talk about sex and share their values with their child. When both parent or guardian and child have agreed, joint discussions can address family values and expectations about dating, relationships, and sexual behavior.111
Although minors are to receive confidential services, Title X providers are not exempt from state notification and reporting laws on child abuse, child molestation, sexual abuse, rape, or incest.112
Some minors who use Title X clinics have dependent health coverage through a parent's private health insurance policy. However, for confidentiality reasons, they may not wish to bill family planning or STD services to their parent's health insurance.113 In one study conducted at 17 Title X sites, 4% of family planning visits were by clients who said they had insurance but did not want to use it. Of those, 44% cited confidentiality concerns. Of those citing confidentiality concerns, 39% were under the age of 18.114 According to OPA, Title X clinics "commonly forgo billing" health insurers to maintain confidentiality.115
As for payment of services provided to minors, Title X regulations indicate that "unemancipated minors who wish to receive services on a confidential basis must be considered on the basis of their own resources."116 Program requirements instruct that "eligibility for discounts for unemancipated minors who receive confidential services must be based on the income of the minor."117
Supporters of confidentiality argue that parental notification or parental consent requirements would lead some sexually active adolescents to delay or forgo family planning services, thereby increasing their risk of pregnancy or sexually transmitted diseases.118
Critics argue that confidentiality requirements can interfere with parents' right to know of and to guide their children's health care. Some critics also disagree with discounts for minors without regard to parents' income, because the Title X program was intended to serve "low-income families."119
Planned Parenthood and Title X
PPFA operates through a national office and 56 affiliates, which operate approximately 600 local health centers.120 Affiliates participating in Title X can receive funds directly from HHS or indirectly from other Title X grantees, such as their state or local health departments. The Guttmacher Institute found that in 2015, Planned Parenthood clinics made up 13% of Title X clinics, but served 41% of female Title X clients.121
In March 2018, the Government Accountability Office (GAO) released a report with data on the obligations, disbursements, and expenditures of federal funds for several nonprofit organizations, including PPFA and its affiliates.122
According to the GAO report, in FY2015, HHS reported obligating $23.41 million and disbursing $21.07 million, to PPFA affiliates through the Title X program.123 These figures reflected funds that HHS provided directly to these organizations. They did not include Title X funds that reached Planned Parenthood or its affiliates indirectly through subgrants or that passed through from state agencies or other organizations.
The GAO report also showed PPFA affiliates' expenditures of Title X funds, identified through audit reports that PPFA affiliates submitted to comply with Office of Management and Budget audit requirements. Expenditures included federal funds provided directly or indirectly to these organizations. The most recent expenditure data were from FY2015, when Planned Parenthood and its affiliates reported spending $57.28 million from the Title X Family Planning Services program.124
On September 22, 2015, the Congressional Budget Office estimated that PPFA and its affiliates receive approximately $60 million annually through the Title X program.125