Introduction
The State Children's Health Insurance Program (CHIP) is a federal-state program that provides health coverage to certain uninsured, low-income children and pregnant women in families that have annual income above Medicaid eligibility levels but do not have health insurance.1 CHIP is jointly financed by the federal government and the states and is administered by the states. Participation in CHIP is voluntary, and all states, the District of Columbia, and the territories participate.2 The federal government sets basic requirements for CHIP, but states have the flexibility to design their own version of CHIP within the federal government's basic framework. As a result, there is significant variation across CHIP programs.
States may design their CHIP programs in one of three ways: a CHIP Medicaid expansion, a separate CHIP program, or a combination approach in which the state operates a CHIP Medicaid expansion and one or more separate CHIP programs concurrently. CHIP benefit coverage and cost-sharing rules depend on program design. CHIP Medicaid expansions must follow the federal Medicaid rules for benefits and cost sharing. For separate CHIP programs, the benefits are permitted to look more like private health insurance, and states may impose cost sharing, such as premiums or enrollment fees, with a maximum allowable amount that is tied to annual family income.
FY2017 is the last year federal CHIP funding has been appropriated in statute. States are expected to have federal CHIP spending in FY2018 because states will have access to unspent funds from their FY2017 allotments and to unspent FY2016 allotments redistributed to shortfall states (if any). However, the Patient Protection and Affordable Care Act's (ACA's; P.L. 111-148, as amended) maintenance of effort (MOE) provision requires states to maintain income eligibility levels for CHIP children through September 30, 2019, as a condition for receiving federal Medicaid payments (notwithstanding the lack of corresponding federal CHIP appropriations for FY2018 and FY2019).3
This report provides an overview of CHIP financing, beginning with an explanation of the federal matching rate. It describes various aspects of federal CHIP funding, such as the federal appropriation, state allotments, the Child Enrollment Contingency Fund, redistribution funds, and outreach and enrollment grants. The report ends with a section about the future of CHIP funding, including the options for extending CHIP funding and what could happen if federal funding expires.
|
CHIP funding was not extended before the beginning of FY2018. As a result, states do not currently have FY2018 CHIP allotments, and states are funding their CHIP programs with unspent federal CHIP funds from their FY2017 allotments and with unspent FY2016 allotments redistributed to shortfall states. Some states are expected to exhaust this funding within the first fiscal quarter of FY2018. On October 4, 2017, both the Senate Finance Committee and the House Energy and Commerce Committee had markups on different bills that would extend CHIP federal funding through FY2022, among other things. The Senate Finance Committee approved the Keeping Kids' Insurance Dependable and Secure (KIDS) Act (S. 1827), which would extend federal CHIP funding through FY2022 and extend the increased E-FMAP rates for one year (i.e., through FY2020) but with an 11.5 percentage point increase instead of a 23 percentage point increase under current law. The bill also includes extensions of other CHIP provisions (e.g., the Express Lane eligibility option and the MOE for children with incomes below 300% of the federal poverty level) and other programs and demonstrations (e.g., the Child Obesity Demonstration Project and the Pediatric Quality Measures Program). The House Energy and Commerce Committee approved the Helping Ensure Access for Little Ones, Toddlers, and Hopeful Youth by Keeping Insurance Delivery Stable (HEALTHY KIDS) Act of 2017 (H.R. 3921), which included almost identical language that would extend CHIP federal funding through FY2022 and extend the increased E-FMAP for one year at 11.5 percentage points. The HEALTHY KIDS Act also would extend the same CHIP provisions and other programs and demonstrations as the KIDS Act. The HEALTHY KIDS Act also included some provisions that were not in the KIDS Act, such as modifying the Medicaid disproportionate share hospital (DSH) allotment reductions and providing additional Medicaid funding to Puerto Rico. The HEALTHY KIDS Act included the following provisions as offsets: modifications to Medicaid third-party liability requirements, treatment of lottery winnings for Medicaid eligibility, and adjustments to Medicare Part B and D premium subsidies for higher-income individuals. |
Federal Matching Rate
The federal government's share of CHIP expenditures (including both services and administration) is determined by the enhanced federal medical assistance percentage (E-FMAP) rate. The E-FMAP rate is based on the FMAP rate, which is the federal matching rate for the Medicaid program. The FMAP formula compares each state's average per capita income with average U.S. per capita income. The formula provides higher reimbursement to states with lower incomes (with a statutory maximum of 83%) and lower reimbursement to states with higher incomes (with a statutory minimum of 50%).4
The E-FMAP rate is calculated by reducing the state share under the regular FMAP rate by 30%.5 Statutorily, the E-FMAP (or federal matching rate) can range from 65% to 85%.6 For some CHIP expenditures, the federal matching rate is different from the E-FMAP rate. For instance, the matching rate for translation and interpretation services is the higher of 75% or states' E-FMAP rate plus 5 percentage points. Also, the Children's Health Insurance Program Reauthorization Act (CHIPRA; P.L. 111-3) included a provision that reduced the matching rate to the regular FMAP rate for children with family incomes exceeding 300% of the federal poverty level (FPL) with an exception for certain states.7
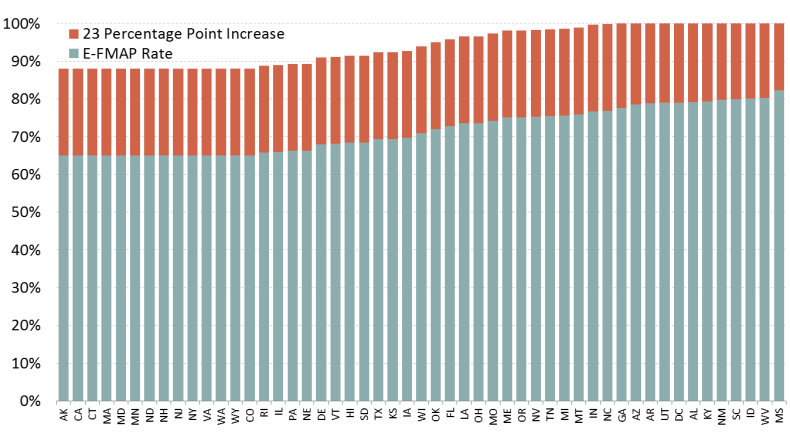
The ACA included a provision to increase the E-FMAP rate by 23 percentage points (not to exceed 100%) for most CHIP expenditures from FY2016 through FY2019. The 23 percentage point increase does not apply to certain expenditures, such as translation services, CHIP children above 300% of FPL (with an exception for certain states), expenditures for administration of citizenship documentation requirements, expenditures for administration of payment error rate measurement (PERM), and Medicaid coverage of certain breast or cervical cancer patients.
This provision increased the statutory range of the E-FMAP rate to between 88% and 100%. In FY2017, 12 states have E-FMAP rates of 100%. Figure 1 shows the state distribution of E-FMAP rates for FY2017 with the 23 percentage point increase. Because the federal share of CHIP is significantly higher with this increase, states are spending through the federal CHIP funding allocated to them (i.e., state CHIP allotments) faster with the increased E-FMAP rate.
Federal CHIP Funding
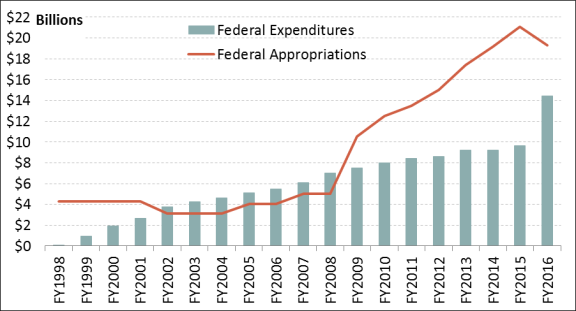
Federal CHIP funding is mandatory spending (i.e., funding controlled outside of the annual appropriations process through authorizing laws), and this funding is an entitlement to states that adhere to the federal CHIP rules. The funding for this program is provided through a mandatory appropriation set in statute. Figure 2 shows the federal appropriation amounts and federal expenditures for CHIP from FY1998 through FY2016.
|
Figure 2. CHIP Federal Expenditures and Federal Appropriations (FY1998 through FY2016) |
 |
|
Sources: §2104 of the Social Security Act, §108 of the Children's Health Insurance Program Reauthorization Act (CHIPRA, P.L. 111-3) as amended by §10203(d)(2)(F) of the Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended), and §301(b)(3) of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA; P.L. 114-10); and Medicaid Financial Management Reports. Note: Federal CHIP expenditures increased significantly from FY2015 to FY2016 due to the Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) provision that increased the E-FMAP rate (or federal matching rate) by 23 percentage points for most CHIP expenditures from FY2016 through FY2019. |
The federal appropriation amount is the maximum amount of federal funding for CHIP. Most of the federal CHIP expenditures are from state CHIP allotments, which are the federal funds allocated to each state to finance its CHIP program. In addition to allotments, states could receive shortfall funding, such as Child Enrollment Contingency Fund payments, redistribution funds, or Medicaid funds. Some CHIP funding is used to finance some Medicaid expenses. In addition, states can receive outreach and enrollment grants.
Federal Appropriation
The federal appropriation for CHIP is provided in Section 2104(a) of the Social Security Act. This amount is the overall annual ceiling on federal CHIP spending to the states, the District of Columbia, and the territories. CHIPRA increased the annual appropriation amounts substantially beginning in FY2009 and provided funding through FY2013. The ACA provided funding for an additional two years (i.e., through FY2015), and the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA; P.L. 114-10) added appropriations for FY2016 and FY2017 at $19.3 billion and $20.4 billion,8 respectively.9
If the federal appropriations were not large enough to cover state allotments in any given year, the state allotments would be reduced proportionally. However, Figure 2 shows the federal appropriation has been more than sufficient to fund federal CHIP expenditures since FY2009.10 In fact, from FY2011 through FY2017, multiple appropriations laws have rescinded a total of $42.8 billion in funding from CHIP (see text box entitled "CHIP Changes in Mandatory Programs" for more detail about these rescissions).
|
CHIP Changes in Mandatory Programs Changes in mandatory programs (CHIMPs) are provisions in appropriations acts that reduce or constrain mandatory spending. From FY2011 through FY2017, multiple appropriations laws have rescinded a total of $42.8 billion in funding from CHIP through CHIMPs. As shown in Table 1, most of these rescissions have come from the performance bonus payment fund. The Children's Health Insurance Program Reauthorization Act (CHIPRA; P.L. 111-3) established performance bonus payments for states that increase their Medicaid (not CHIP) enrollment among low-income children above a defined baseline. States were eligible for performance bonus payments from FY2009 through FY2013. The fund balance for the performance bonus payments increased significantly every year because the transfers into the fund were substantially higher than the actual performance bonus payments to states. From FY2011 through FY2017, a total of $30.0 billion was rescinded from the performance bonus payment fund. Funds also have been rescinded from unobligated national allotments, which are federal appropriations funds not allocated for state allotments. In FY2015 through FY2017, a total of $11.1 billion was rescinded from unobligated national allotments. In FY2016, funds were rescinded from the Child Enrollment Contingency Fund in the amount of $1.7 billion. The Child Enrollment Contingency Fund is one potential CHIP shortfall funding source available to states (see the "Child Enrollment Contingency Fund" section).
Sources: Defense and Full-Year Appropriations, 2011 (P.L. 112-10); Consolidated Appropriations Act, 2012 (P.L. 112-74); Consolidated and Further Continuing Appropriations Act, 2013 (P.L. 113-6); Consolidated Appropriations Act, 2014 (P.L. 113-76); Continuing Appropriations Resolution, 2015 (P.L. 113-164); Consolidated and Further Continuing Appropriations Act, 2015 (P.L. 113-235); Continuing Appropriations Act, 2016 (P.L. 114-53); Consolidated Appropriations Act, 2016 (P.L. 114-113); Continuing Appropriations and Military Construction, Veterans Affairs, and Related Agencies Appropriations Act, 2017, and Zika Response and Preparedness Act (P.L. 114-223); Further Continuing and Security Assistance Appropriations Act, 2017 (P.L. 114-254); and Consolidated Appropriations Act, 2017 (P.L. 115-31). Note: Totals may not add due to rounding. |
State Allotments
State allotments are the federal funds allocated to each state and territory for the federal share of its CHIP expenditures. CHIPRA established a new allocation of federal CHIP funds among the states based largely on states' actual use of and projected need for CHIP funds.11 There are two formulas for determining state allotments: an even-year formula and an odd-year formula.12
In even years, such as FY2016, state CHIP allotments are each state's allotment for the prior year plus any Child Enrollment Contingency Fund (described below) payments from the previous year adjusted for growth in per capita National Health Expenditures and child population in the state.
In odd years, state CHIP allotments are each state's spending for the prior year (including federal CHIP payments from the state CHIP allotment, payments from the Child Enrollment Contingency Fund, and redistribution funds) adjusted using the same growth factor as the even-year formula (i.e., per capita National Health Expenditures growth and child population growth in the state).
Since the odd-year formula is based on states' actual use of CHIP funds, it is called the re-basing year because a state's CHIP allotment can either increase or decrease depending on that state's CHIP expenditures in the previous year. Figure 3 shows how the re-basing for FY2011 significantly decreased the aggregate amount for state allotments from FY2010 to FY2011, and in FY2015, CHIP allotments increased due to state spending in FY2014.
|
Figure 3. CHIP Allotments and Federal Expenditures (FY2009 through FY2016) |
 |
|
Sources: Various Federal Register notices; Medicaid and CHIP Payment and Access Commission (MACPAC), "Federal CHIP Allotments, FYs 2015-2017," MACStats Exhibit 33, posted online May 10, 2017; and the Medicaid Financial Management Reports. Note: Federal CHIP expenditures increased significantly from FY2015 to FY2016 due to the Patient Protection and Affordable Care Act (ACA; P.L. 111-148, as amended) provision that increased the E-FMAP rate (or federal matching rate) by 23 percentage points for most CHIP expenditures from FY2016 through FY2019. The FY2016 allotments were calculated under a special rule that took into account the 23 percentage point increase in the E-FMAP that begins in that year. |
State CHIP allotment funds are available to states for two years, which explains why federal expenditures are higher than the state allotments in some years. The federal CHIP expenditures can include federal funding from states' allotments for the specified year and the prior year in addition to shortfall funding.
The allotment is available to states to cover the federal share of both CHIP benefit and administrative expenditures.13 However, no more than 10% of the federal CHIP funds that a state draws down from its CHIP allotment can be spent on nonbenefit expenditures, including expenditures for administration, translation services, and outreach efforts.
MACRA added special rules to the state allotments for FY2016 and FY2018. The special rule for FY2016 establishes the states' allotments by taking into account the 23 percentage point increase in the E-FMAP that begins in that year. Specifically, the FY2016 allotments are each state's FY2015 allotment (including Child Enrollment Contingency Fund payments and redistribution funds), determined as if the 23 percentage point increase in the E-FMAP were in place for FY2015. Then, that amount was adjusted using the same growth factor as the even- and odd-year formulas (i.e., growth in per capita National Health Expenditures and child population in the state).
For FY2018, MACRA included a provision that will reduce the amount of states' unspent funds from their FY2017 allotments available for expenditures in FY2018 by one-third. Although FY2017 is the last year for which federal CHIP funding is provided under current law, states could have federal CHIP spending in FY2018 because states could have access to unspent funds from their FY2017 allotments and unspent FY2016 allotments redistributed to shortfall states.
Shortfall Funding
If a state's CHIP allotment for the current year, in addition to any allotment funds carried over from the prior year, is insufficient to cover the state's projected CHIP expenditures for the current year, a few different shortfall funding sources are available. These sources include the Child Enrollment Contingency Fund, redistribution funds, and Medicaid funds.
Child Enrollment Contingency Fund
CHIPRA established the Child Enrollment Contingency Fund and made its funds available to states for FY2009 through FY2013. The ACA extended the availability of the Child Enrollment Contingency Fund and of payments from the fund through FY2015, and MACRA extended the fund and payments through FY2017.14 A state is eligible for Child Enrollment Contingency Fund payments if it has both a funding shortfall15 and CHIP enrollment (for children) that exceeds a target level.16 As a result, not all states with funding shortfalls are eligible for Child Enrollment Contingency Fund payments.
The Child Enrollment Contingency Fund was funded with an initial deposit equal to 20% of the appropriated amount for FY2009 (i.e., $2.1 billion). In addition, for FY2010 through FY2017, such sums as are necessary for making Child Enrollment Contingency Fund payments to eligible states are to be deposited into the fund, but these transfers cannot exceed 20% of the federal appropriation for the fiscal year.
The Child Enrollment Contingency Fund payment formula is based on a state's growth in CHIP enrollment and per capita spending, which means a state may receive a payment from the fund that does not equal its actual shortfall. Iowa, Michigan, and Tennessee are the only states that have received Child Enrollment Contingency Fund payments since FY2009, when the funds were first available.17
Redistribution Funds
After two years, any unused state CHIP allotment funds are redistributed to shortfall states.18 For redistribution funds, a shortfall state is defined as a state that will not have enough money to meet projected costs in the current year after counting (1) the current year's state allotment, (2) unspent funds from the prior year's state allotment, and (3) available Child Enrollment Contingency Fund payments. If redistributed funds are insufficient to meet the needs of all shortfall states, each shortfall state receives a proportionate share of the available funds based on the shortfall in each state. Since FY2009, Michigan and four territories (Puerto Rico, American Samoa, the Commonwealth of the Northern Mariana Islands, and Guam) have received redistribution funds.19
Medicaid Funds
States that design their CHIP program as a CHIP Medicaid expansion or a combination program and face a shortfall after receiving Child Enrollment Contingency Fund payments and redistribution funds may receive federal Medicaid matching funds to fund the shortfall in the CHIP Medicaid expansion portion of their CHIP program. When Medicaid funds are used to fund CHIP, the state receives the lower regular FMAP rate (i.e., the federal Medicaid matching rate) rather than the higher E-FMAP rate provided for other CHIP expenditures. However, although federal CHIP funding is capped, federal Medicaid funding is open-ended, which means there is no upper limit or cap on the amount of federal Medicaid funds a state may receive.
Federal CHIP Funds Finance Some Medicaid Expenditures
In some situations, such as the qualifying state option and the stairstep children, federal CHIP funding is used to finance Medicaid expenditures.
Qualifying State Option
Certain states had significantly expanded Medicaid eligibility for children prior to the enactment of CHIP in 1997, and these states are allowed to use their CHIP allotment funds to fund the difference between the Medicaid and CHIP matching rates (i.e., FMAP and E-FMAP rates, respectively) to finance the cost for children in Medicaid above 133% of FPL. This provision is referred to as the qualifying state option. FY2015 was the last year for which the qualifying state option was authorized until MACRA extended the qualifying state option through FY2017.
The following 11 states meet the definition of a qualifying state: Connecticut, Hawaii, Maryland, Minnesota, New Hampshire, New Mexico, Rhode Island, Tennessee, Vermont, Washington, and Wisconsin. Although 11 states are eligible for this option, only 6 states (Connecticut, Minnesota, New Hampshire, Vermont, Washington, and Wisconsin) had CHIP expenditures under the qualifying state option in FY2016.20
Stairstep Children
The ACA required states to transition CHIP children aged 6 through 18 in families with annual income less than 133% of FPL to Medicaid, beginning January 1, 2014.21 Coverage for such children continues to be financed with states' CHIP annual allotment funding at the E-FMAP rate as long as their income eligibility is greater than the state's March 31, 1997, Medicaid income standard for children.22 However, the E-FMAP rate is not available for children between the ages of 6 and 18 who have access to private health insurance.
Outreach and Enrollment Grants
CHIPRA established outreach and enrollment grants aimed at reducing the number of children eligible for but not enrolled in Medicaid and CHIP and improving retention so that eligible children stay covered for as long as they are eligible for the programs. CHIPRA provided $100 million to fund the outreach and enrollment grants for FY2009 through FY2013. The ACA extended the outreach and enrollment grants through FY2015 and provided an additional $40 million in funding. MACRA extended the outreach and enrollment grants through FY2017 and authorized another $40 million in funding.
Ten percent of the allocation was to be directed to a national enrollment campaign, and 10% was to be targeted to outreach for American Indian and Alaska Native children. The remaining 80% was to be distributed among state and local governments and to community-based organizations for purposes of conducting outreach campaigns, with a particular focus on rural areas and underserved populations. Grant funds also were targeted at proposals that address cultural and linguistic barriers to enrollment.
Future of CHIP Funding
Federal funding for CHIP is set to end after FY2017, absent further action by Congress. In considering the future of CHIP, it is helpful to recall why the program was created in 1997: to provide affordable health coverage at a time when there were few other insurance coverage options for low-income children outside of Medicaid. The health insurance market is far different today, with the enactment of the ACA. Now, if CHIP funding is exhausted, current CHIP-eligible children could be eligible for Medicaid or potentially for subsidized coverage in the health insurance exchanges. However, not all CHIP-eligible children would be eligible for these programs, and some could end up being uninsured if CHIP is no longer available.
With FY2017 being the final year for which federal CHIP funding is provided in statute, Congress's action or inaction will determine the future of CHIP and of health coverage for CHIP children. In considering the future of CHIP, Congress has a number of policy options, including extending federal CHIP funding and continuing the program, or letting CHIP funding expire.
Extending Federal CHIP Funding
If Congress decides to extend federal CHIP funding after FY2017, there are a number of policy options regarding how long to extend funding and whether to make programmatic changes. Funding could be extended for just a few years (e.g., two or four years) or indefinitely, and the extension could maintain, phase down, or eliminate the 23 percentage point increase to the E-FMAP rate (i.e., the federal matching rate for CHIP). (See the textbox "Federal Cost of Extending CHIP Funding" for more information about extending CHIP funding.)
|
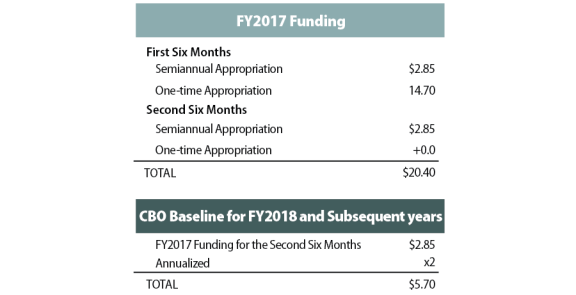
Federal Cost of Extending CHIP Funding The Congressional Budget Office (CBO) is required to assume that mandatory spending programs in existence on or before the enactment of the Balanced Budget Act of 1997 (P.L. 105-33), which would include CHIP, that lack future appropriations and have current-year outlays of at least $50 million will continue operating as they had been immediately prior to their expiration. This requirement is in the Balanced Budget and Emergency Deficit Control Act of 1985, Section 257(b)(2). Under current law, as shown in Figure 4, funding for CHIP in FY2017 consists of two semiannual appropriations of $2.85 billion—amounts that are much smaller than the appropriations in other years. The first semiannual appropriation in FY2017 will be supplemented by a one-time appropriation in the amount of $14.70 billion provided in the first six months of FY2017 that will remain available until expended. To calculate the CHIP program levels that will continue in the baseline pursuant to these scorekeeping rules, CBO annualizes the $2.85 billion provided for the allotment for the last six months of its authorization for the remainder of the baseline period. CBO does not include the other amounts provided to CHIP for the earlier part of FY2017 because these are not available immediately before the program expires at the end of the fiscal year. For this reason, CBO's baseline for CHIP includes $5.7 billion in federal CHIP funding for each year after FY2017.
Because the baseline projections assume $5.7 billion in federal CHIP spending for FY2018 and subsequent years within the budget window, CBO's estimated cost of extending federal CHIP funding is lower than it would have been without this assumption. In addition, the federal costs of extending CHIP funding would be offset by reductions in federal spending for Medicaid and subsidized exchange coverage because some CHIP children would receive Medicaid coverage or subsidized exchange coverage if CHIP were to expire. |
If Federal CHIP Funding Expires
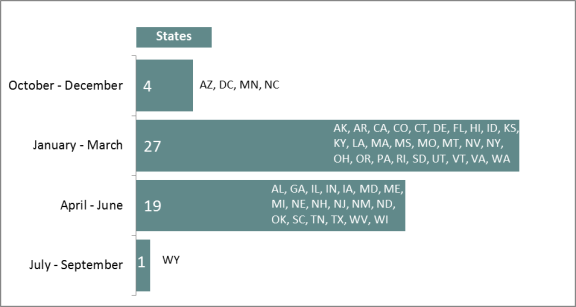
Although FY2017 is the last year for which federal CHIP funding is provided under current law, states are expected to have federal CHIP spending in FY2018 because states will have access to unspent funds from their FY2017 allotments and to unspent FY2016 allotments redistributed to shortfall states (if any). States are expected to exhaust their federal CHIP funding at different times throughout FY2018. According to a projection conducted by the Medicaid and CHIP Payment and Access Commission (MACPAC), three states (Arizona, Minnesota, and North Carolina) and the District of Columbia are projected to exhaust federal CHIP funds in the first fiscal quarter, and more than half of states are expected to exhaust their federal CHIP funding by the second fiscal quarter of FY2018 (see Figure 5). Wyoming is projected to be the last state to exhaust federal CHIP funding, in July 2018.23
If federal CHIP funding expires after FY2017, the loss of funding and the ACA MOE requirements would affect states' CHIP programs differently depending on whether the program is a CHIP Medicaid expansion or a separate CHIP program.
The CHIP enrollees in CHIP Medicaid expansion programs (almost 60% of CHIP enrollees)24 likely would continue to receive coverage through their state's Medicaid program due to the ACA MOE requirement, which requires states to maintain income eligibility levels for CHIP children through September 30, 2019, as a condition for receiving any Medicaid funding (notwithstanding the lack of corresponding federal CHIP appropriations for FY2018 and FY2019).25 This switch would cause the federal share of expenditures to decrease from the E-FMAP rate to the regular FMAP rate, which means the cost of covering these children would increase for states.
For the CHIP enrollees in separate CHIP programs (roughly 40% of CHIP enrollees),26 if CHIP funding expires, states would have to enroll eligible children in Medicaid or certified qualified health plans in the health insurance exchanges. A certified qualified health plan is a qualified health plan that has been certified by the Secretary of Health and Human Services (HHS) to be "at least comparable" to CHIP in terms of benefits and cost sharing. The HHS Secretary was required by statute to review the benefits and cost sharing for children under qualified health plans in the exchanges and certify those plans that offer benefits and cost sharing that are at least comparable to CHIP coverage.27 In the review released November 25, 2015, the HHS Secretary was not able to certify any qualified health plans as comparable to CHIP coverage because out-of-pocket costs were higher under the qualified health plans and the CHIP benefits were generally more comprehensive for child-specific services (e.g., dental, vision, and habilitation services).28 States with separate CHIP programs would not be required to continue coverage after enrolling eligible children in Medicaid or certified qualified health plans.