Introduction
The Maternal and Child Health (MCH) Services Block Grant is administered by the Maternal and Child Health Bureau (MCHB) of the Health Resources and Services Administration (HRSA) in the Department of Health and Human Services (HHS). This block grant is intended to improve the well-being of the low-income maternal and child population. According to HRSA, the MCH Services Block Grant serves as a "safety-net provider for the [maternal and child health] population by providing gap-filling health care services, as well as essential public health services, to the [maternal and child health] population."1 Generally, these services are provided to pregnant women, mothers, children, and children with special health care needs (CSHCNs), some of whom are also eligible for and receive services from Medicaid2 or the State Children's Health Insurance Program (CHIP).3
The MCH Services Block Grant is composed of three funding programs. The first is a block grant and is the largest of the three funding programs. It is provided to states and territories (referred to collectively as states in this report)4 to enable them to coordinate programs, develop systems, and provide a broad range of health services.5 The second funding program is the Special Projects of Regional and National Significance (SPRANS) program. SPRANS is a competitive grant program that funds research and training projects that focus on low-income pregnant women, mothers, and children, including CSHCNs. The third funding program is the Community Integrated Service Systems (CISS) program. CISS is a competitive grant program that funds projects that support the development and expansion of integrated services at the community level.
The MCH Services Block Grant is the oldest federal-state partnership program.6 A federal-state partnership is a program that joins a federal agency with a state or jurisdiction, in order for the two to address a certain issue. Under this federal-state partnership, states make available federal and nonfederal funds to provide health care services to their maternal and child health populations (see the "Requirements of Block Grant Allocation and Distribution" section of this report). The FY2015 dollar amounts from these sources, the latest available, are presented in Table A-1. Congress established this block grant under Title V of the Social Security Act (SSA, P.L. 74-271, as amended).
Program History
The MCH Services Block Grant was established to serve as a single block grant under the previous SSA statutory heading, "Title V – Grants to States for Maternal and Child Welfare";7 which was referred to as "Title V." In 1981, Congress combined the MCH Services Block Grant with other maternal and child health services and programs.8 Such services and programs aimed to improve the health of mothers and children, particularly those in low-income households.9 They included maternal and child health services, services for disabled children, child welfare services, and vocational rehabilitation services. Title V services included activities related to abstinence, postpartum depression, and personal responsibility educational services and programs.
The 97th Congress named this consolidation the MCH Services Block Grant and renamed it in statute as the "Title V MCH Services Block Grant," which is commonly referred to as "Title V." This change was implemented by the Omnibus Budget Reconciliation Act (OBRA)10 of 1981 (P.L. 97-35), as amended.11 The 1981 OBRA gave states more flexibility in determining how to use federal funds to address maternal and child health needs. In addition, the 1981 OBRA required that each state receive, at a minimum, the combined funding of the programs consolidated under it.
Congress made additional changes to the MCH Services Block Grant under the Omnibus Budget Reconciliation Act of 1989 (P.L. 101-239). These changes increased the authorization of appropriations; called for greater accountability; and created stricter rules for application and reporting requirements for states, including a statewide needs assessment requirement. Over time, additional programs targeting CSHCNs and low-income women and children were added to the SSA and the Public Health Service Act (PHSA).12 Title V also supports services that are offered by the Maternal, Infant, and Early Childhood Home Visiting (MIECHV) program and the state-based CSHCNs program.13
The Maternal and Child Health Services Block Grant
Purpose
The MCH Services Block Grant program creates partnerships between the federal government and states. The aim of the federal-state partnerships is to give attention to the health care needs of the maternal and child health populations.14 The MCH Services Block Grant enables states to
- ensure that quality health care is provided to mothers and children, particularly to those with low incomes or limited availability of care;
- reduce the number of infant deaths, preventable diseases, and handicapping conditions among children;
- reduce hospital inpatient and long-term care services;
- increase the number of low-income children who receive health assessments and follow-up diagnostic and treatment services;
- provide perinatal care15 to low-income, at-risk women and provide preventive and primary care services to low-income children;
- provide rehabilitation services that are not under subchapter XIX16 of the SSA to blind and disabled children who are under the age of 16 and who are beneficiaries under subchapter XVI17 of the SSA;
- provide family-centered, community-based, and care-coordinated services; and
- enable the development of community-based systems for CSHCNs.18
Population Served
The population served by the MCH Services Block Grant consists of pregnant women, infants, children, CSHCNs, and others. HRSA defines these as follows:
- Pregnant Women. Pregnant women are served from the date of conception to 60 days after the child or fetus is delivered or "expulsion of the fetus" happens.19 Expulsion may occur, for example, when a miscarriage takes place.
- Infants. Infants are babies aged one year and less.20
- Children. Children are served from the age of one year, up to the day before their 22nd birthday. If a female child becomes pregnant, HRSA classifies her as a pregnant woman rather than as a child.
- Children with Special Health Care Needs. CSHCNs are infants and children who have or are at risk of having a disability, chronic illness/condition, or educational/behavioral issue.21
- Others. This category includes women who are over 21 years of age (referred to by HRSA as child-bearing age) and other individuals who are not defined by a state as being in one of the categories above.22
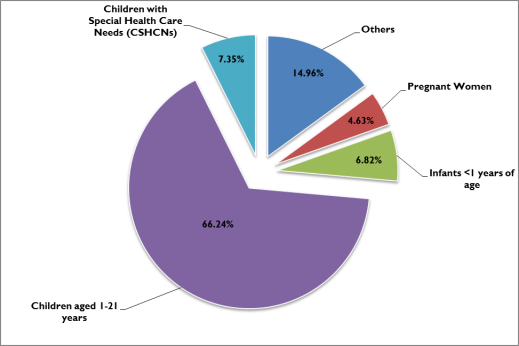
In FY2015 (the year in which the most recent data are available), 57,064,187 individuals were served by programs funded by the MCH Services Block Grant (see Figure 1). Of the total served, 2,640,078 were pregnant women, 3,891,644 were infants, 37,797,789 were children, 4,195,464 were CSHCNs, and 8,539,212 were "others" (women of childbearing age and any others who are not classified by the state).23
|
Figure 1. Percentage of Individuals Served Under the MCH Services Block Grant, by Classification, FY2015 |
 |
|
Source: Health Resources and Services Administration, "Explore the Title V Federal-Partnership," https://mchb.tvisdata.hrsa.gov/. Note: "Others" includes women of childbearing age and any others who are not classified by the state. Individuals who received direct and enabling services were counted for each health care service that was provided to them. |
Programs and Services
The primary use of funds under the MCH Services Block Grant, including formula grants to states, competitive grants for Special Projects of Regional and National Significance (SPRANS), and competitive grants for projects through the Community Integrated Services Systems (CISS) program, is to provide core public health services for low-income mothers and children. Projects funded by SPRANS include maternal and child health workforce development, genetic services, and diagnostic and treatment services for hemophilia. CISS grants fund projects that support integrated maternal and child health services at the community level.
Block Grants to States
Block grant funds are to be used by the states "to provide and to assure mothers and children (in particular those with low income or with limited availability of health services) access to quality maternal and child health services."24 States determine the actual services provided under the block grant. For example, such services may include
- counseling services,
- dental care,
- family planning,
- immunization,
- inpatient services,
- prenatal care,
- screening services for lead-based poisoning,
- support for community health centers,
- vision and hearing screening services, and
- well-child care.25
Participation
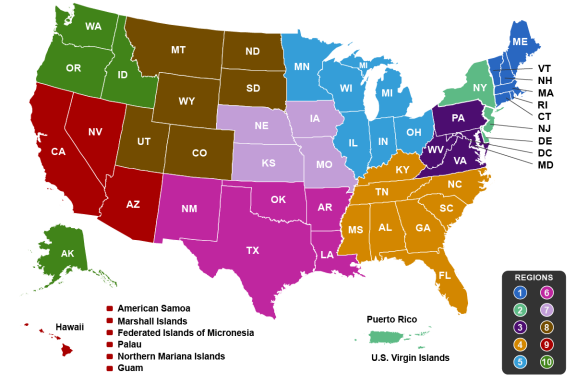
All 50 states and nine jurisdictions26 may apply for the MCH Services Block Grant.27 In FY2015 (the year in which the most recent data are available), block grant funding to each of the states and nine jurisdictions ranged from $154,000 to $38,909,810 (see Table A-1).28 According to HRSA, "within each state, the state health agency is responsible for the administration (or supervision of the administration) of programs carried out with Title V allotments."29 States are organized within the 10 general regions of HHS (see Figure 2).
 |
|
Source: Figure prepared by CRS based on information from Health Resources and Services Administration, MCH Public Health 101, https://mchb.hrsa.gov/about/timeline/in-depth-1-mchph101.asp. Notes: This figure illustrates the general regions of the Department of Health and Human Services (HHS). See Department of Health and Human Services, Regional Offices, https://www.hhs.gov/about/agencies/iea/regional-offices/. |
Types of Funded Services
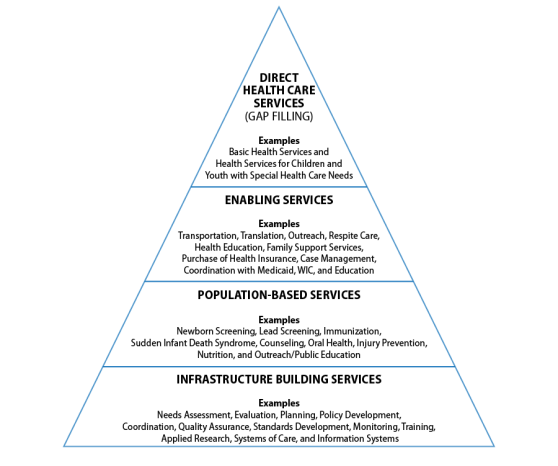
There are four types of funded services: (1) direct health care services, (2) enabling services, (3) population-based services, and (4) infrastructure building services. Generally, these core services are presented as a four-level pyramid (see Figure 3).30
|
Figure 3. Four-Level Pyramid of Core Maternal and Child Health Services |
 |
|
Source: Figure prepared by CRS based on information from Health Resources and Services Administration, MCH Public Health 101, https://mchb.hrsa.gov/about/timeline/in-depth-1-mchph101.asp. Notes: Under the enabling services category, WIC stands for the Special Supplemental Nutrition Program for Women, Infants, and Children and Education refers to the Department of Education. |
Although states deliver four types of services, direct health care services incurred the largest proportion (57.62%) of expenditures under the MCH Services Block Grant program in FY2015.31 Direct health care services are intended to fill the gaps in primary and preventive health care that are not otherwise available through other funding sources or providers, such as private insurance, Medicaid, or CHIP. In FY2015, approximately $3.87 billion went to direct services.32 In that same fiscal year, the MCH Services Block Grant program incurred $6.29 billion in expenditures (see Table A-1 in Appendix A). Other federal and nonfederal funds combine with the actual (appropriated) funding level of the block grant to yield the larger figure, reflecting the nature of the grant's federal-state partnership.
Permitted Service Use
States may use their block grants "to provide and to assure [that] mothers and children (in particular those with low income or with limited availability of health services) [have] access to quality maternal and child health services."33 States determine the actual services provided under the block grant. For example, a state may provide medical services in sectors where public and private health insurers offer limited coverage options, such as coverage for dental and durable medical equipment (e.g., wheelchairs and oxygen equipment). In addition, states may use their MCH Services Block Grant to support the following activities:
- expand the capacity of state and local health care systems;
- engage in community capacity building to deliver enabling services, such as transportation, nutrition counseling, and care coordination;
- offer education and outreach programs, technical assistance, and provider training;
- increase newborn screening and genetic services, as well as injury and lead poisoning prevention;
- promote health care and safety in child care settings; and
- provide additional support for CSHCNs.34
According to HRSA's FY2017 Annual Performance Report, "the MCH Services Block Grant program also serves as the payer of last resort. In cases where no resources or services are available, states use their block grants to fund direct care services, such as prenatal care, pediatric specialty care, or services for children with special health care needs."35
Prohibited Service Use
Certain uses of block grant funds are prohibited under Section 504 of the SSA:36
- Funds may not be used to pay for inpatient services, other than for children with special health care needs, high-risk pregnant women, and infants (unless approved by the Secretary of HHS).
- States may not use the block grant funds to provide cash payments to recipients of health services, or for the purchase of land, facilities, or major medical equipment.
- States may not use funds to satisfy any requirement for the expenditure of nonfederal funds, and may not transfer block grant funds to any other program.
- Block grant funds may not be used for research or training at a private, for-profit entity.
In addition, block grant funds are subject to any restrictions that are included in Division H of the Consolidated Appropriations Act, 2017 (P.L. 115-31). For example, funds from the MCH Services Block Grant may not be used to promote or advocate for gun control.37
Requirements to Receive Funds
To receive block grant funds, states must submit to the Secretary of HHS an application that includes a statewide needs assessment (to be conducted once every five years) and a plan for meeting the needs that were identified in the needs assessment. The needs assessment must identify statewide goals that intend to meet national health objectives; the need for preventive and primary care services for pregnant women, mothers, infants, and children; and services for CSHCNs.38 The plan to address those needs must describe how and where block grant funds will be used within the state.
Coordination with Related Programs
State block grant administrators must coordinate with other related programs, including the state's Medicaid program (specifically the Early Periodic Screening, Diagnosis, and Treatment [EPSDT] Program);39 the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC);40 related education programs; and other health, developmental disability, and family planning programs. The primary purpose of this coordination effort is to make Medicaid services accessible, to enroll those who are eligible, and to avoid duplication of effort among the programs. Coordination varies among states and jurisdictions.41
Some state Medicaid and maternal and child health agencies have created interagency agreements that outline the expected areas and levels of coordination between the programs. Within these agreements, some states specify the services that are provided by each agency. Generally, the Title V agency contracts with health providers to provide the services, and the agency administering the state's Medicaid program assumes responsibility for reimbursing those services, when possible. HRSA performed an analysis of the coordination efforts between state Medicaid and maternal and child health agencies in 2008. This analysis showed a wide variety in the scope and level of formality among interagency agreements.42
Special Projects of Regional and National Significance (SPRANS)
The SPRANS program is a competitive grant for research and training programs and services related to maternal and child health and children with special health care needs. SPRANS may be used for genetic disease testing, counseling, and information development and dissemination programs; for grants relating to hemophilia without regard to age; for the screening of newborns for sickle cell anemia and other genetic disorders; and for follow-up services.43 Eligible grantees include (1) public or nonprofit private institutions of higher learning that train health care and maternal and child health personnel and (2) public or nonprofit private organizations or institutions of higher learning that conduct maternal and child health research. Preference is given to applicants who carry out their projects in areas with a high infant mortality rate.44
A high infant mortality rate is defined as an infant mortality rate that is higher than the average national infant mortality rate or higher than the average infant mortality rate within a state.45 For example, the national infant mortality rate was 5.82 for every 1,000 live births in 2014.46 As reported by the Centers for Disease Control and Prevention (CDC), Indiana's infant mortality rate in 2014 was 7.08.47 Accordingly, relative to the national average, Indiana had a high infant mortality rate in 2014. That same year in Indiana, the infant mortality rate for black infants was 14.34, more than twice as much as the state's infant mortality rate of 7.08.48 As a result, compared with the state's overall infant mortality rate, the rate for black infants was high in Indiana, in 2014.
Community Integrated Service Systems (CISS)
CISS is a competitive grant program that funds projects that support the development and expansion of integrated services at the community level. Public and private organizations or institutions are eligible for these grants. CISS projects must "seek to increase service delivery capacity" at the local level and promote community-based health systems for mothers and children, particularly for children in rural areas and those with special health care needs.49 Section 502 of the SSA authorizes CISS funds to be made available for various programs, such as the MIECHV program, community-based health service programs for CSHCNs, and programs for the maternal and child health population that reside in rural areas. CISS funds may also be made available for various activities, such as integrating maternal and child health systems and increasing the participation of obstetricians and pediatricians under Medicaid and the Title X Family Planning program.
Funding by Program
The MCH Services Block Grant is allocated by formula. The following allocation requirements are provided by 42 U.S.C §702(a):
- SPRANS: 15% of the appropriation that does not exceed $600 million, and 15% of funds remaining above $600 million after CISS funds are set aside.
- CISS: 12.75% of the appropriation that is above 600 million.
- Block grants to states: remainder of the total appropriation.
These allocation requirements have not always been implemented; for example, they were not implemented for the FY2016 funding (see the "Appropriations History" section of this report).
Block Grants to States
Individual state allocations are determined by a formula that compares the proportion of low-income children in a state with the total number of low-income children within all states. Specifically, the first $422 million of the amount appropriated is distributed to each state based on the amount the state received under the consolidated maternal and child health programs in 1983.50 Any funds above that amount are distributed based on the number of children in each state who are at or below 100% of the federal poverty level (FPL)51 as a proportion of the total number of children at or below 100% of the FPL for all states.52
State matching funds and other sources of maternal and child health funding are not required to follow the allocation requirements of federal funds, giving the states flexibility to direct those funds where they are needed. Similarly, state funds are not required to be directed toward specific populations in the same proportions as the federal block grant allocation.
Block grant funds are awarded each fiscal year in quarterly installments and remain available for spending in the current and subsequent fiscal year.53 Table A-1 shows the federal allocation and state match for FY2015, by state.
Requirements of Block Grant Allocation and Distribution
For the purposes of allocating block grant funds for this program, low-income mothers and children are defined as those with family income below 100% of federal poverty guidelines.54 However, due to the broad reach of Title V programs and services, this definition is used only in the allocation formula, and not as a criterion for receiving Title V-funded services. There is no federally prescribed means test for recipients of services funded by the block grants to states.
States are required to use at least 30% of their block grant allocations for the population of CSHCNs, 30% for services for preventive and primary care services for children, and 40% for services for either of these groups or for other appropriate maternal and child health activities. However, states may use no more than 10% of their federal allocations for administrative costs.55 Beyond these broad requirements, states determine the actual services provided under the block grant.
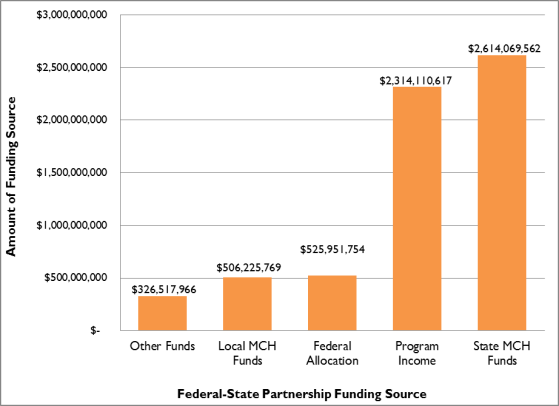
A state that partners with the federal government under this program must sustain a level of state funding for its maternal and child health programs and services that matches, at a minimum, its FY1989 level of state funding.56 HRSA categorizes the funding for federal-state partnerships as coming from five sources:57
- 1. Federal allocation is the funding that a state receives from the federal government.
- 2. Local MCH funds are from local jurisdictions within a state.
- 3. Other funds include, but are not limited to, funds from the Centers for Disease Control and Prevention (CDC); Emergency Medical Services for Children (EMSC); Healthy Start; and the Special Supplemental Nutrition Program for Women, Infants and Children (WIC).
- 4. Program income funds are collected by state maternal and child health agencies that include health maintenance organization (HMO) payments, insurance payments, and Medicaid reimbursements.
- 5. State MCH funds are the funds that states match to their federal allocations. States are required to match at least $3 for every $4 given by the federal government.
In FY2015, the federal-state partnership was funded at $6.3 billion (see Figure 4).58 Two sources—State MCH funds and program income—accounted for more than 78% of combined federal and state spending.
|
Figure 4. Federal-State Partnership Funding, by Source, FY2015 |
 |
|
Source: Figure prepared by CRS based on data from Health Resources and Services Administration, Funding by Source, https://mchb.tvisdata.hrsa.gov/Financial/FundingBySource. |
Nonuse of Funds
If a state chooses not to apply for block grant funds, is not qualified for such funds, or indicates that it does not plan to use its full allotment, that state's allotment is redistributed among the remaining states in the proportion otherwise allotted to the state.59
SPRANS
By law, of the amount appropriated to the MCH Services Block Grant (up to $600 million), 15% is awarded on a competitive basis to public and private not-for-profit organizations for SPRANS. Congress has directed some SPRANS funds through authorizations and appropriations for specific programs. The program also receives 15% of funds remaining above $600 million after CISS funds are set aside.
Generally, the priority for funding SPRANS projects is determined by HRSA. However, Congress has sometimes provided specific directives for certain programs, including set-asides. For example, the FY2017 Consolidated Appropriations Act included appropriations language that provided SPRANS set-aside funds for oral health ($5.25 million, an increase of 5% from FY2016), epilepsy ($3.64 million, same allocation from FY2016), sickle cell ($3.00 million, an increase of 1.35% from FY2016), and fetal alcohol syndrome ($0.48 million, same allocation as FY2016).60 In FY2016, these congressional directives comprised about 16% of SPRANS funding.61 Additionally and under the Continuing Appropriations and Military Construction, Veterans Affairs, and Related Agencies Appropriations Act, 2017, and Zika Response and Preparedness Act (P.L. 114-223), Congress provided $20 million in supplemental funding to the SPRANS program to help territories respond to the Zika virus.62 In FY2016, HRSA awarded $17 million to American Samoa, U.S. Virgin Islands, and Puerto Rico under the SPRANS program, to help the territories address the Zika virus.63
Currently, SPRANS has additional funding of $5 million to develop Family-to-Family Health Information Centers (F2F HICs) through FY2017. (See Appendix B for the appropriation history of F2F HICs.) The F2F HICs program funds family-staffed and family-run centers64 in 50 states and the District of Columbia.65 The F2F HICs provide information, education, technical assistance, and peer support to families of children (including youth) with special health care needs and health professionals who serve such families. In addition, the centers help ensure that families and health professionals are partners in decisionmaking at all levels of care and service delivery.
CISS
The SSA requires Congress to appropriate over $600 million to the MCH Services Block Grant in order to initiate any funding for the CISS program. The CISS program will receive a set-aside of 12.75% of any amount appropriated over $600 million.66 Since HRSA began providing CISS competitive grants in 1996, Congress has not appropriated any amount less than $600 million to the MCH Services Block Grant program.67 Funds are distributed on a competitive basis to public and private nonprofit organizations, with preference given to entities that propose activities focusing on areas with high infant mortality rates.68
Appropriations History
In FY2016, HRSA received $638.2 million for the MCH Services Block Grant program. This funding was allocated differently from what is stated in 42 U.S.C. §702(a) (as described in the "Funding by Program" section of this report). The appropriations were not allocated in this manner because under the Consolidated Appropriations Act, 2016 (P.L. 114-113), Congress mandated that no more than $77.1 million (rounded) would be made available to SPRANS, "notwithstanding sections 502(a)(1) and 502(b)(1) of the SSA."69 As a result of the FY2016 appropriation and as shown in HRSA's FY2018 congressional budget justification report, $77.1 million (12.08%; the SSA calls for 15%) was for SPRANS, $10.3 million (1.61%) was for CISS, and $550.8 million (86.31%) was for block grants to states.70 Table 1 shows the FY2016 appropriation of $638.2 million if funding allocation followed what is stated in the SSA.
|
MCH Programs |
SSA Formula |
FY2016 Appropriation |
FY2016 Appropriation by SSA Formula |
Difference |
|
SPRANS |
|
$77.1 |
$95.0a |
-$17.9 |
|
CISS |
|
$10.3 |
$4.9b |
$5.4 |
|
Block grants to states |
|
$550.8 |
$538.3c |
$12.5 |
Source: Table prepared by CRS using data from Health Resources and Services Administration, FY2018 Justification of Estimates for Appropriations Committees, 2017, p. 151 https://www.hrsa.gov/sites/default/files/hrsa/about/budget/budget-justification-2018.pdf; 42 U.S.C. §702(a)(1); 42 U.S.C. §702(b)(1); and 42 U.S.C. §702(c).
a. $95 million is the sum of 15% of $600 million plus 15% of $33.3 million. $33.3 million is what remains after CISS funds are set aside.
b. $4.9 million is 12.75% of $38.2 million.
c. $538.3 million is the remainder after subtracting $95.0 million and $4.9 million from the $638.2 million total appropriation.
Mandatory Reporting at the State and National Levels
At the state and national levels, Section 505 of the SSA71 requires three reporting mechanisms:
- 1. A needs assessment, which must be performed every five years (as discussed in the "Requirements to Receive Funds" section of this report).
- 2. An annual report, including program participation data, state maternal and child health measures, and state pediatric and family workforce measures.
- 3. An independent audit, which must be performed every two years.
State Reporting Requirements72
Each state must prepare and submit an annual report to the Secretary of HHS on all Title V activities.73 The reports must be presented in a standardized format. States must provide a list of activities and recipients of Title V funding, along with a description of progress toward meeting national and state health objectives, and their consistency with the state's needs assessment. Specifically, these reports must include information on program participation, standardized measures of maternal and child health, and data on maternal and child health systems, including measures of the pediatric and family practice workforce. While the measures are designed to standardize reporting across the states, states vary in terms of their capacity for collecting and reporting data.
For example, states must provide the number of individuals served, either in person or by phone, by the Title V block grant. The numbers provided by states may be estimates if the actual numbers are not available. States are also required to report expenditures by the four broad categories of service (direct health care services, enabling services, population-based services, and infrastructure-building services).
States are required to annually report pediatric and family practice workforce data to HRSA, including information on the number of obstetricians, family practitioners, certified family nurse practitioners, certified nurse midwives, pediatricians, and certified pediatric nurse practitioners who were licensed in the state in that year. States are also required to report data on whether individuals who are eligible for programs such as Medicaid74 and Supplemental Security Income (SSI)75 are receiving services, or whether pregnant women have access to adequate prenatal care. For example, states report the number of Medicaid-eligible individuals who received a service paid for by the Medicaid program.
In addition to the above-mentioned annually reported indicators, states select and report 7 to 10 priority needs in their five-year strategic plans; states may annually adjust the strategic plans as their priorities change. Priority needs that were frequently identified in states' FY2017 MCH Services Block Grant applications include family support services, oral health services, childhood obesity prevention and treatment, mental and behavioral health systems, and access to services for children with disabilities.
National Reporting Requirement
HRSA must annually compile the information reported by states and present the data to the House Committee on Energy and Commerce and the Senate Committee on Finance in a report to Congress.76 This report must include a summary of the information reported to the Secretary of HHS by the states (described in the previous section) and a compilation of specified maternal and child health indicators, nationally and by state. States can access their vital statistics and health data from the National Center for Health Statistics (NCHS) of CDC. The NCHS does not collect vital statistics or health data for American Samoa, Commonwealth of the Northern Mariana Islands, Federated States of Micronesia, Guam, Marshall Islands, Palau, Puerto Rico, or U.S. Virgin Islands.77 Therefore, these jurisdictions must report their own data. The Secretary must also provide a report on funded SPRANS and CISS projects to those committees.
Appendix A. Source of Funding for Title V Block Grants to States, the District of Columbia, and Other Jurisdictions, by State, FY2015
|
State |
Federal Allocation |
Total State Funds |
Other Funds (including local MCH funds) |
Program Income (Reimbursements)b |
Total |
||||||||||||
|
Alabama |
11.3 |
30.6 |
|
|
|
||||||||||||
|
Alaska |
|
|
|
|
|
||||||||||||
|
Arizona |
7.2 |
7.8 |
5.9 |
|
|
||||||||||||
|
Arkansas |
|
|
|
|
|
||||||||||||
|
California |
|
|
|
|
|
||||||||||||
|
Colorado |
|
|
|
|
|
||||||||||||
|
Connecticut |
|
|
|
|
|
||||||||||||
|
Delaware |
|
|
|
|
|
||||||||||||
|
District of Columbia |
|
|
|
|
|
||||||||||||
|
Florida |
|
|
|
|
|
||||||||||||
|
Georgia |
|
|
|
|
|
||||||||||||
|
Hawaii |
|
|
|
|
|
||||||||||||
|
Idaho |
|
|
|
|
|
||||||||||||
|
Illinois |
|
|
|
|
|
||||||||||||
|
Indiana |
|
|
|
|
|
||||||||||||
|
Iowa |
|
|
|
|
|
||||||||||||
|
Kansas |
|
|
|
|
|
||||||||||||
|
Kentucky |
|
|
|
|
|
||||||||||||
|
Louisiana |
|
|
|
|
|
||||||||||||
|
Maine |
|
|
|
|
|
||||||||||||
|
Maryland |
|
|
|
|
|
||||||||||||
|
Massachusetts |
|
|
|
|
|
||||||||||||
|
Michigan |
|
|
|
|
|
||||||||||||
|
Minnesota |
|
|
|
|
|
||||||||||||
|
Mississippi |
|
|
|
|
|
||||||||||||
|
Missouri |
|
|
|
|
|
||||||||||||
|
Montana |
|
|
|
|
|
||||||||||||
|
Nebraska |
|
|
|
|
|
||||||||||||
|
Nevada |
|
|
|
|
|
||||||||||||
|
New Hampshire |
|
|
|
|
|
||||||||||||
|
New Jersey |
|
|
|
|
|
||||||||||||
|
New Mexico |
|
|
|
|
|
||||||||||||
|
New York |
|
|
|
|
|
||||||||||||
|
North Carolina |
|
|
|
|
|
||||||||||||
|
North Dakota |
|
|
|
|
|
||||||||||||
|
Ohio |
|
|
|
|
|
||||||||||||
|
Oklahoma |
|
|
|
|
|
||||||||||||
|
Oregon |
|
|
|
|
|
||||||||||||
|
Pennsylvania |
|
|
|
|
|
||||||||||||
|
Rhode Island |
|
|
|
|
|
||||||||||||
|
South Carolina |
|
|
|
|
|
||||||||||||
|
South Dakota |
|
|
|
|
|
||||||||||||
|
Tennessee |
|
|
|
|
|
||||||||||||
|
Texas |
|
|
|
|
|
||||||||||||
|
Utah |
|
|
|
|
|
||||||||||||
|
Vermont |
|
|
|
|
|
||||||||||||
|
Virginia |
|
|
|
|
|
||||||||||||
|
Washington |
|
|
|
|
|
||||||||||||
|
West Virginia |
|
|
|
|
|
||||||||||||
|
Wisconsin |
|
|
|
|
|
||||||||||||
|
Wyoming |
|
|
|
|
|
||||||||||||
|
Other Jurisdictions |
|||||||||||||||||
|
American Samoa |
|
|
|
|
|
||||||||||||
|
Federated States of Micronesia |
|
|
|
|
|
||||||||||||
|
Guam |
|
|
|
|
|
||||||||||||
|
Marshall Islands |
|
|
|
|
|
||||||||||||
|
Northern Mariana Islands |
|
|
|
|
|
||||||||||||
|
Palau |
|
|
|
|
|
||||||||||||
|
Puerto Rico |
|
|
|
|
|
||||||||||||
|
Virgin Islands |
|
|
|
|
|
||||||||||||
|
Total |
|
|
|
|
|
||||||||||||
Source: Table prepared by CRS based on data from HRSA, Title V Information System, Federal-State Title V Block Grant Partnership Budget FY2015, https://mchb.tvisdata.hrsa.gov/.
Notes: Some totals are imprecise because of rounding. Not every state submitted data to HRSA on their other funds and program income. These data is shown as $0 in the table.
a. States are allowed to exceed the matching requirement of at least $3 for every $4 of federal funds awarded. This amount is an "overmatch."
b. Program income includes funding from private entities and income collected from insurance payments and Medicaid. For purposes of meeting the state match requirement, states are allowed to use nonfederal program income toward their match.
Appendix B. Appropriation History of the Family-to-Family Health Information Centers
The Family-to-Family Health Information Centers (F2F HICs) program was authorized under the following legislation:
- The Deficit Reduction Act of 2005 (P.L. 109-171) received a direct appropriation of $3 million for FY2007, $4 million for FY2008, and $5 million for FY2009.
- The Patent Protection and Affordable Care Act (ACA; P.L. 111-148)78 replaced the $5 million to be appropriated in FY2009 and provided $5 million for each of FY2009-FY2012 for the program.
- The American Taxpayer Relief Act of 2012 (P.L. 112-240) funded the program at $5 million for FY2013.
- The Bipartisan Budget Act of 2013 (P.L. 113-67) provided a half year of funding ($2.5 million), which expired April 1, 2014.
- Protecting Access to Medicare Act of 2014 (PAMA; P.L. 113-93) provided $2.5 million for the remainder of FY2014 (from April 1, 2014, to September 30, 2014), and it provided $2.5 million for the first half of FY2015 (October 1, 2014, through March 31, 2015).
- The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA; P.L. 114-10)79 struck the partial funding provided and provided full-year funding of $5 million for FY2015. It also provided $5 million for each of FY2016 and FY2017.
Appendix C. MCH Services Block Grant Funding History for the Past 10 Years
|
Fiscal Year |
Amount of Grants to States |
Amount of Grants for SPRANS |
Amount of Grants for CISS |
Total Appropriations |
|
2006 |
566.1 |
115.9 |
10.6 |
692.5 |
|
2007 |
561.7 |
115.9 |
10.6 |
693.0 |
|
2008 |
551.2 |
99.2a |
10.4 |
666.2 |
|
2009 |
553.8 |
92.6b |
10.4 |
662.1 |
|
2010 |
558.0 |
92.4 |
10.4 |
660.7 |
|
2011 |
555.7 |
90.2 |
10.4 |
656.3 |
|
2012 |
549.7 |
78.6 |
10.3 |
638.6 |
|
2013 |
520.7 |
74.5 |
9.7 |
604.9 |
|
2014 |
545.3 |
76.9 |
10.3 |
632.4 |
|
2015c |
549.6 |
77.1 |
10.3 |
637.0 |
|
2016 |
550.8 |
77.1d |
10.3 |
638.2 |
Source: Table prepared by CRS using annual Department of Health and Human Services, Health Resources and Services Administration budget justifications and appropriations legislation for the relevant years. Funding levels are not adjusted for inflation.
a. In FY2008, $20 million was transferred from SPRANS to the Autism program line.
b. In FY2009, $6.9 million was transferred from SPRANS to the Heritable Disorders line. The Autism program and the Heritable Disorder program also are administered by HRSA's Maternal and Child Health Bureau.
c. The FY2015 appropriation of $637 million is different from HRSA's source of funding, which is shown as $6.29 billion in Table A-1 in Appendix A.
d. In FY2016, Congress provided $20 million in supplemental funding to the SPRANS program to help territories respond to the Zika virus. In FY2016, HRSA awarded $17 million to American Samoa, U.S. Virgin Islands, and Puerto Rico under the SPRANS program, to help the territories address the Zika virus.
Appendix D. Abbreviations Used in This Report
|
ACA |
Affordable Care Act |
|
ACS |
American Community Survey |
|
CC |
Crippled Children's Program |
|
CDC |
Centers for Disease Control and Prevention |
|
CHIP |
State Children's Health Insurance Program |
|
CISS |
Community-Integrated Services System Program |
|
COBRA |
Consolidated Omnibus Budget Reconciliation Act |
|
CSHCNs |
children and youth with special health care needs |
|
EMSC |
Emergency Medical Services for Children Program |
|
EPSDT |
Early Periodic Screening, Diagnosis, and Treatment Program |
|
F2F HICs |
Family-to-Family Health Information Centers |
|
FPL |
federal poverty level |
|
FY |
fiscal year |
|
HHS |
Department of Health and Human Services |
|
HMO |
health maintenance organization |
|
HRSA |
Health Resources and Services Administration |
|
TVIS |
Title V Information System |
|
MACRA |
Medicare Access and CHIP Reauthorization Act of 2015 |
|
MCH Services Block Grant |
Maternal and Child Health Services Block Grant |
|
MCHB |
Maternal and Child Health Bureau |
|
MIECHV |
Maternal, Infant, and Early Childhood Home Visiting Program |
|
OMB |
Office of Management and Budget |
|
NHIS |
National Health Interview Survey |
|
PAMA |
Protecting Access to Medicare Act of 2013 |
|
PHSA |
Public Health Services Act |
|
SPRANS |
Special Projects of Regional and National Significance Program |
|
SSA |
Social Security Act |
|
WIC |
Special Supplemental Nutrition Program for Women, Infants, and Children |